



The AAWC Conceptual Framework of Quality Systems for Wound Care
In 2002, the Association for Advanced Wound Care (AAWC) formed and funded the multidisciplinary Quality of Care Task Force with the intent to improve the quality of wound care services. This task force, represented by podiatrists (DPMs), registered nurses (RNs), advanced practice registered nurses (APRNs), wound ostomy continence nurses (WOCNs), and physical therapists (PTs) who are consultants, clinicians, administrators, and manufacturers working in hospital-based, outpatient, freestanding, and home health service arenas is a diverse multidisciplinary group with insights into the full breadth of the healthcare system.
 After determining that no single universally accepted definition of quality existed as related to wound care, the Task Force moved to identify components of quality wound care that are applicable across disciplines, service sites, and the continuum of care. A framework of wound care quality indicators for practice was created; it was suggested this framework then could be used to create or critique a wound care service delivery system. The framework was designed to be responsive to the needs of not only the clinician, but also the managers and regulatory agencies that oversee care. The Task Force consensus paper provides the framework for a wound care delivery system that is grounded in quality, flexibility, and effectiveness while recognizing and being responsive to regulatory and managerial guidelines.
After determining that no single universally accepted definition of quality existed as related to wound care, the Task Force moved to identify components of quality wound care that are applicable across disciplines, service sites, and the continuum of care. A framework of wound care quality indicators for practice was created; it was suggested this framework then could be used to create or critique a wound care service delivery system. The framework was designed to be responsive to the needs of not only the clinician, but also the managers and regulatory agencies that oversee care. The Task Force consensus paper provides the framework for a wound care delivery system that is grounded in quality, flexibility, and effectiveness while recognizing and being responsive to regulatory and managerial guidelines.
Methods
Literature search. From May 2002 to May 2004, the Task Force performed a wound care literature search on the topic of “quality” and its subsets of “wound,” “ulcer,” “healing,” “health,” “clinical,” “hospital,” and “skin” and further subsets such as “arterial,” “venous,” “diabetic,” “vascular,” “neuropathic,” and “chronic” using sources such as the Cochrane Collaborative Databases and Reviews, National Institutes of Health, the Institutes of Medicine websites, and links from relevant national associations including the American Academy of Wound Management; the Wound, Ostomy, Continence Nursing Society; the American Medical Association; the National Pressure Ulcer Advisory Panel; the American Physical Therapy Association; the American Academy of Dermatology; and the American Podiatric Medical Association. Additionally, insurer websites such as the Center for Medicare and Medicaid Services, United Healthcare, and regional Blue Cross and Blue Shield members were searched for quality indicators or assessment tools. Articles were found that equated quality with outcomes and end points, but no articles were found that incorporated the full breadth of the relationships between the clinical providers, the institutional management system, and the regulatory organizations and their systems. When no citations were found, the Task Force expanded the search into the medical and business literature using websites from the Small Business Administration, The British Quality Foundation, and the US Chamber of Commerce; fewer than five articles were tangentially relevant. The list of articles from these searches were culled to include only those relevant to wound care or its delivery systems.
Framework formulation. Over the next 14 months, Task Force members discussed the issues affecting quality within their varied work environments. Using the information gleaned from the literature and Task Force members’ expertise, several components were unanimously agreed to be crucial to a successful wound care program: safety, effectiveness, patient-centeredness, timeliness, efficiency, and equitableness were recognized for their applicability regardless of patient diagnosis, site of service, and regulatory or pay source.
During review of the literature search, the Institute of Medicine framework article1 was presented and discussed. Two Task Force members developed a diagrammatic representation of quality as a building, with each portion of the building representing a different factor affecting quality. For example, the foundation is the patient and caregiver and their relationship and responsibilities to each other and the roof represents the regulatory and accreditation agencies and their responsibilities to the health delivery system and, ultimately, the patient.
Document review and acceptance. The work of writing the paper was divided among the Task Force subcommittees, with each section reviewed, critiqued, and re-written by the entire committee. Each section was reviewed for clarity, consistency with the other sections and with the goal of the paper, and reputable sources and citations supporting the assertions and was re-written until the full committee was in agreement with the results.
Discussion/Conclusion
When the AAWC Conceptual Framework of Quality Systems for Wound Care was completed, the Quality of Care Task Force had three goals: distribute it as widely as possible (publication in an indexed journal and on the AAWC website), stimulate discussion about intentionally creating and reinforcing quality care, and create a “baseline” document to serve as a foundation for others to use in their pursuit of quality care provision. During the 4 years the Quality of Care Task Force spent developing this framework, each of its versions has made it more applicable, flexible, and responsive to the variety of factors that affect quality. Future research is needed to create a body of literature addressing the process of quality wound care, rather than focusing only on outcomes.
AAWC Conceptual Framework of Quality Systems for Wound Care
The AAWC Conceptual Framework of Quality Systems for Wound Care describes an innovative conceptual model that serves as a basis for meeting the AAWC strategies to facilitate high quality wound care for patients and clients across the continuum of care. The framework also provides guidance and support to the systems that offer wound care services.
The framework uses the Institute of Medicine’s (IOM) Crossing the Quality Chasm: A New Health System for the 21st Century1 as an inspiration for defining quality systems for wound care (see Figure 1). Each segment is responsible to the others. The loss of any segment jeopardizes the integrity of the entire structure.

At the foundation of the framework is the patient/client. The concept of placing the patient at the base of the conceptual model facilitates patient empowerment and ownership in the decision-making processes related to wound management. The incorporation of the concept of the patient as the foundation of the pillars of quality requires that the patient have:
• Collaborative relationships with healthcare providers who share knowledge and cooperatively set treatment goals
• Shared governance in an environment where care is customized to patient needs and values
• A Wound Care Patient’s Bill of Rights©.2
Framework Applied to Wound Care
The six separate but interrelated components of the AAWC Conceptual Framework of Quality Systems for Wound Care include:
The patient — representing the patient and his/her support structure, experience, biases, goals, and fears
The pillars of quality — quality wound care is:
Safe: avoids injuries or untoward outcomes to patients from the care intended to help them
Effective: provides services based on scientific knowledge to all who could benefit and refrains from providing services to those not likely to benefit. Intervention is directed to provide the best patient outcome
Patient-centered: provides care that is respectful of and responsive to individual patient preferences, needs, and values; ensures that patient values guide all clinical decisions
Timely: reduces waits and delays for those who receive and give care
Efficient: avoids waste, especially of time, equipment, supplies, ideas, and energy
Equitable: provides quality care to all patients regardless of personal characteristics such as gender, ethnicity, geographic location, or socio-economic status.
The microsystem — providers, patient/client population, and their interaction with the information systems that support and guide care
The macrosystem — healthcare organizations, facilities, or agencies that house microsystems and are accountable to, as well as influenced by, regulators
The regulators — governmental and risk management organizations that have responsibility for, and impact on, the healthcare provider macrosystem. The key players of the macrosystem include industry regulators such as Centers for Medicare and Medicaid Services (CMS); Joint Commission on Accreditation of Healthcare Organizations (JCAHO); third-party payors; and federal, state, and local legislators
Outcomes — the effect the five framework components have on the patient’s quality of life as it relates to economic, clinical, and humanistic aspects of the wound. Recognizing that the macro-, micro-, and regulatory systems exist for the patient’s benefit, the patient’s placement as the foundation of the conceptual framework empowers him/her to actively participate in wound care decision-making.
Pillars of Quality
Safety. Patient safety is defined by the Agency for Healthcare Research and Quality (AHRQ) as “Freedom from accidental or preventable injuries produced by medical care.”3 Safety, therefore, is a result of providing the right care at the right time to the right person in the right manner. In the ideal wound care world, perfect safety means the patient heals as expected with the least amount of pain and no complications.
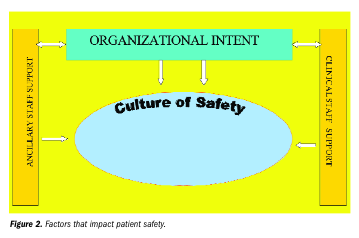
The National Agenda for Action: Patients and Families in Patient Safety4 identifies the changes necessary to facilitate patient safety in staff, systems, and corporate-centered operations (see Figure 2). Corporate leadership supports the creation of a culture of safety by providing the ancillary and clinical staff adequate material and educational training. For example, the leadership provides adequate cleaning material and training of the ancillary staff — the ancillary staff cleans the wound care clinic so the clinical staff may provide services with minimal risk of nosocomial infections.
 Healthcare providers and recipients both recognize the importance of receiving and providing safe therapeutic interventions. This was reinforced by JCAHO when it identified the urgent need for patient safety through its national patient safety goals. This has particular application to wound care: in 2006, pressure ulcers were recognized as targets for JCAHO patient safety initiatives, which are available at: https://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/.
Healthcare providers and recipients both recognize the importance of receiving and providing safe therapeutic interventions. This was reinforced by JCAHO when it identified the urgent need for patient safety through its national patient safety goals. This has particular application to wound care: in 2006, pressure ulcers were recognized as targets for JCAHO patient safety initiatives, which are available at: https://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/.
The practice of safe wound care is underscored in the AAWC’s Wound Care Bill of Rights© and includes:
• accurate diagnosis (or a working diagnosis)
• consistent communication
• appropriate evidence-based intervention
• clear documentation
• regular re-assessment to ensure progress toward identified goals set between patient and provider.
Accurate diagnosis. Many professional organizations, product manufacturers, and regulatory and governmental bodies have assessment guidelines/algorithms that are available to the public and healthcare providers.5-9 To improve the consistency of clinical assessment, wound care providers have the opportunity to adopt evidence-based assessment algorithms appropriate for their setting, population, and staff. One example is the Summary Algorithm for Venous Ulcer Care with Annotations of Available Evidence developed by the AAWC Government and Regulatory Task Force, available at the National Guideline Clearinghouse or at https://www.guidelines.gov.
Consistent communication. For communication with healthcare professionals, use of a common language and lexicon will provide the easiest means for mutual understanding. Because most medical communication is done in a written format, inconsistent use of terms and descriptors makes accurate information exchange difficult. For communicating with patients or their caregivers, using language that matches their level of understanding can maximize their understanding and ability to follow plans of care and ultimately improve outcomes.
Appropriate evidence-based intervention. “Evidence-based clinical practice is an approach to decision making in which the clinician uses the best evidence available, in consultation with the patient, to decide upon the option which suits that patient best.”10 Use of evidence-based interventions is considered to reflect leading-edge thinking and high quality healthcare services. Developing treatment protocols based on well-researched interventions allows for growth and change in treatment regimens as new products and concepts evolve.
Wound care providers needs to carefully review the source and content of their evidence-based interventions. Using a common Internet search engine for the phrase wound care with a subsearch for evidence-based interventions, the Task Force found 1,850,000 citations. These citations are from a variety of sources, including professional associations, insurers, regulators, product manufacturers, and researchers, as well as anecdotal listings. Reading the relevant research with a critical eye is the best way to use the best information in a manner consistent with the needs of the patient, provider, facility, and regulators.
Documentation. Documentation must meet the requirements of patients and the macrosystems that support and facilitate care. According to Task Force members’ combined experiences, the key to clear documentation is the use of a dual systems approach with a clinical and managerial documentation process. Clinical documentation describes actual patient-centered care; whereas, the managerial documentation describes and supports the organizational structure and processes in which the clinical services are provided.
Regular re-assessment. Re-assessment is more than a replay of the assessment. Re-assessment ensures that the updated patient status clearly reinforces or alters the current plan of care.
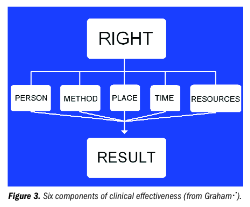
Wound care effectiveness. In the practice of wound care efficacy, effectiveness and outcomes have been elusive terms. Efficacy describes how well a treatment achieves the desired outcome in the ideal, controlled clinical trial setting.10 While evidence of effectiveness also must be obtained through clinical trials, effectiveness can be practiced at the bedside. Graham11 depicts the six components of clinical effectiveness as “six rights,” including the right person doing the right thing in the right way at the right time in the right place with the right results (see Figure 3). Research in wound care regarding effect of provider certification, place of service, and resource utilization on patient outcomes is currently sparse.
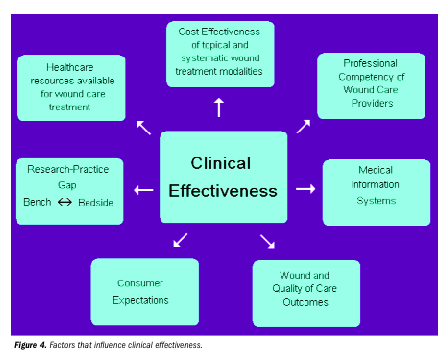
 Clinical and professional experience inform that clinical effectiveness is influenced by a number of different factors acting individually and collectively on wound healing (see Figure 4). If one of the factors in this model is inadequate, the effectiveness of the care provided is impaired.
Clinical and professional experience inform that clinical effectiveness is influenced by a number of different factors acting individually and collectively on wound healing (see Figure 4). If one of the factors in this model is inadequate, the effectiveness of the care provided is impaired.
Outcome-driven patient care serves as a guide to monitor quality. Providing outcome feedback to clinicians impacts clinical and non-clinical decisions, including clinician practice patterns, development of products, and reimbursement of materials and service. Effective wound care includes outcomes management and outcomes research. Outcomes management is defined as the use of data collected in the course of clinical care for a specified purpose. Outcomes research focuses on investigations to determine “what works and does not work” during the provision of clinical care.12-14
Physiological improvements, with the endpoint/outcome of complete wound closure, are often considered the standard definition of effective wound care. However, the Wound Care Bill of Rights, in concert with the other pillars of quality, requires that the definition of effective include quality of life, functional status, patient satisfaction, and costs associated with care14-16 due to the reality of multiple endpoints that do not include complete wound closure as the final outcome (eg, palliative care). A number of resources are available that support wound care effectiveness, including evidence-based literature reviews, the Cochrane database, and the Agency for Healthcare Research National Clinical Practice Guideline Clearinghouse, available at https://www.guidelines.gov.
Patient-centered wound care. Patients were once expected to be passive, unquestioning recipients of healthcare, but they are now expected to play a central role in their care, participating in discussions and helping to plan and sometimes implement their treatment. The IOM1 states, “Patient-centeredness encompasses qualities of compassion, empathy, and responsiveness to the needs, values, and expressed preferences of the individual patients and family.” The clinical philosophy “nothing about me without me” clearly expresses that patient involvement in care is integral to improving outcomes.4 Health Affairs: the Policy Journal of the Health Sphere17 states, “If patients are to play a critical role in care, then the degree to which providers support and improve patients’ capabilities for participation must also be part of the quality measurement picture.”
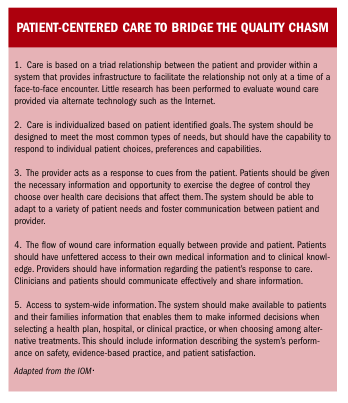
The Institute of Medicine Report1 lists 10 principles to follow when systemic improvements are being considered for the healthcare delivery system. Five principles underscore the importance of placing the patient at the center of information exchange and service delivery (see “Patient-centered care to bridge the quality chasm”).
In a patient-centered healthcare system, the patient or identified surrogate is encouraged to participate at every level of care. The patient, as the nexus of control, is provided relevant and understandable information so informed decisions may be made, waste minimized, and positive outcomes maximized.
Timeliness in wound care. Timeliness comprises three components. The first is the patient’s perception of obtaining prompt medical care, including time to obtain care. Most patients wait for appointments on the telephone, in the lobby, and in the treatment room. Once treatment is initiated, a delay between treatment orders and the implementation of those orders may occur. Timeliness impacts the delivery of effective patient care and the patient’s perception of the quality of care provided.1,18
The second component is the medical practitioner, for whom timeliness relates to work flow. The practitioner, much like the patient, waits to obtain a needed service (eg, necessary information, equipment, or room availability) before formulating or initiating a patient’s treatment plan. The wait causes delays for the patient and decreased efficiency for the practitioner; related frustration may result in real and perceived decreased outcomes for the patient and the practitioner.1,18
The third component is appropriate treatment. Acute and chronic disease states18 both require timely care throughout the treatment continuum. Failure to treat in a timely manner at any of the various stages in the disease process affects outcomes. For example, in a patient who develops a Stage I pressure ulcer, the optimal treatment involves intervention at initial time of injury to prevent further breakdown. If timely care is not provided, the Stage I ulcer may progress to Stage II or beyond. Every Stage III or Stage IV ulcer may be considered an ulcer that did not receive the appropriate treatment at the appropriate time.
Efficiency in wound care. Efficiency is the relationship between patient care and the resources required to deliver it.19 The most obvious way to increase efficiency is to reduce waste. Qualitative resource (ie, ideas, energy, and practitioner skill) and administrative costs (eg, non-qualitative expenses such as multiple entries, multiple layers of control, and classification systems) have been the primary focus in eliminating waste.1 An efficient system also reduces waste through reduction of redundant costs. In addition, errors and over- and underuse issues increase expenses, decrease outcomes, and decrease efficiency for the patient and for the healthcare system.1,3
As a clinical component in the healthcare system, the wound care practitioner is challenged to deliver wound care that is clinically efficient and cost-effective in the shortest time. Currently, no consensus exists regarding universally accepted wound treatment protocols. This is due to the development of new technologies in wound care, the varied regulatory and reimbursement systems, and the diverse training of different practitioners. Some practitioners are vehemently opposed to using advanced wound dressings, believing the “tried and true wet gauze changed three times per day” has proven and continues to prove itself the best dressing system in all situations and circumstances. As an emerging science, wound care relies on individual skill and knowledge to progress healing. This leads to disparate approaches, for example, to topical wound care and equally disparate costs and outcomes. As a result of these disparate approaches, available evidence on topical wound care cost effectiveness is limited.20-22
Efforts by professionals, organizations, and industry already have produced change and improvements in efficiency that emphasize appropriateness of care and adherence to professional standards.1 Interest in wound care cost effectiveness and outcomes are increasing. Continued cooperation between all parties will be imperative for future improvements.
Equity in wound care. Equitable wound care is defined as providing quality care to all patients, residents, and clients regardless of personal characteristics such as gender, ethnicity, geographic location, and socio-economic status. Despite the fact that professional organizations across healthcare agree that providing care of equal quality to everyone who needs it is a necessity, large disparities remain.23
In the IOM report,1 monetary expense often is cited as the primary barrier to equitable care. Part of the issue may be that many healthcare improvement initiatives focus on high-tech changes that may be cost-prohibitive for smaller organizations. Often, low-tech changes are viable options. The Institute for Healthcare Improvement (IHI)23 cites concepts and methods to improve access, patient flow, and care management as interventions that easily adapt to numerous care settings, regardless of material resources.
Although technological advances are an important, and necessary part of the healthcare system, the AAWC also supports “low-tech” solutions. For example, the AAWC promotes educating healthcare professionals on moist wound healing so everyone is offered a basic level of quality care.24 The AAWC also supports wound care as a specialty and acts as a resource to other professionals and the community. In addition, the AAWC educates the public to enhance understanding of the issues at stake and their role in the wound healing process.
Micro- and macrosystems. While the six pillars define the parameters of the care delivered, the actual care delivery is provided by the microsystem — the patient/client population and the information system(s) that support and guide care the delivery of care. Two examples of a microsystem are a care center/outpatient wound clinic and a wound care unit within a facility or agency. The microsystem uses comprehensive quality-based principles to help direct wound care services. These principles should be grounded in:
• Knowledge — care is committed to using the best scientific and clinical information available in the service of the patient. This means the patient is entitled to best-practice wound care
• Patient-centeredness — care that respects the individuality, values, ethnicity, social endowments, and informational needs of the patient. The patient is in control of his/her own care. Wound care customized according to individual needs, desires, and circumstances comes with a high level of microsystem accountability to the patient/client
• Systems-minded care — quality of care extends within the boundaries of the microsystem. Such care requires coordination, integration, and efficiency across traditional roles, disciplines, and services — these parameters will be defined by the needs of the system within which the care is provided (eg, a rural community health clinic funded through the county will have different microsystem needs than a large university-based hospital).
The macrosystems are the healthcare organizations, facilities, and/or agencies overarching multiple microsystems. The macrosystem has a strong interest in defining best practices and ensuring they become organizational standards. The macrosystem is responsible for holding the microsystems accountable for quality wound care outcomes, defining both the cost of excellence and the cost of poor quality.
The macrosystem is accountable to and influenced by multiple outside forces. These include but are not limited to federal, state, and local regulatory agencies, accreditation organizations, payors, consumer expectations, social policy, professional organizations/education, and potential and real litigation proceedings.
Conclusion
The AAWC has taken a leadership role in modeling the Institute of Medicine’s Quality Initiative by developing the “Wound Patient’s Bill of Rights.” The formation of the AAWC Task Forces is an important step in the creation of a culture of quality. Although it does not provide specific instruction or recipes for quality, it does provide the six ingredients needed to have quality services and a paradigm for implementing them.
The AAWC Conceptual Framework of Quality Systems for Wound Care is a tool that may be used by persons, organizations, or regulators who desire to improve the quality of patient services. Its flexibility allows it to be customized to meet the needs in a variety of settings. The AAWC Conceptual Framework of Quality Systems for Wound Care is a comprehensive quality management guide designed for wound care. Providers and the systems in which they practice are encouraged to narrow the research-practice gap evident in this framework. Until then, AAWC individual members are encouraged to use this framework within their setting to improve quality of care.
Financial support for this project was provided by the AAWC.
1. Committee on Quality Healthcare in America, Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
2. Association for Advancement of Wound Care. Wound Care Patient Bill of Rights. Malvern, Pa: Association for Advancement of Wound Care;1995.
3. Committee on Quality Healthcare in America, Institute of Medicine. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press;1999.
4. National Patient Safety Foundation. National Agenda for Action: Patients and Families in Patient Safety: Nothing about Me, Without Me. North Adams, Mass: National Patient Safety Foundation; 2002. Available at http://www.npsf.org/download/2002annualreport. Accessed February 3, 2006.
5. Han P, Ezquerro E. Diabetic foot wound care algorithms. J Am Podiatr Med Assoc. 2002;92(6):336–349.
6. Agency for Healthcare Research and Quality. National Guideline Clearing House. Available at: http://www.guidelines.gov. Accessed June 1, 2006.
7. American Medical Director Association. Clinical practice guidelines. Available at: http://www.amda.com/tools/guidelines.cfm. Accessed January 8, 2006.
8. Association for Advancement of Wound Care. Government and Regulatory Task Force, 2005. Summary algorithm for venous ulcer care with annotations of available evidence. Available at http://www.guidelines.gov/summary/summary.aspx?doc_id=7109&nbr=004280&string=venous+AND+ulcer. Accessed October 10, 2005.
9. Wound Ostomy Continence Nurses Society, 2005. Guideline for management of wounds in patients with lower-extremity venous disease. Available at http://www.guideline.gov/summary/summary.aspx?doc_id=7485&nbr=4431. Accessed January 15, 2006.
10. Muir Gray JA. Evidence-based Healthcare: How to Make Health Policy and Management Decisions. London, UK: Churchill Livingstone;1997.
11. Graham G. Evidence-based practice. An international perspective. Physio Forum. 2001;15(8):13–14.
12. Geddes J. Evidence-based practice in mental health. In: Trinder L, Reynolds S (eds). Evidenced-based Practice — A Critical Appraisal. Oxford, UK: Blackwell Science;2000.
13. Ramsey SD. Evaluating evidence from a decision analysis. In: Geyman JP, Deyo RA (eds). Evidence-Based Clinical Practice: Concepts and Approaches. Oxford, UK: Butterworth-Heinemann;2000.
14. Bolton L. Outcomes research. WOUNDS. 2004;16(5):148–149.
15. Soon S, Chen S. What are wound care outcomes? WOUNDS. 2004;16(5):150–156.
16. Macario A. The economic assessment of advanced wound care products: from research theory to practice. European Tissue Repair Society Bulletin. Available at: http://www.etrs.org/bulletin8_1/index.html. Accessed August 10, 2005.
17. Hibbard J. Perspective: moving toward a more patient-centered health care delivery system. Health Affairs: The Policy Journal of the Health Sphere. October 7, 2004. Available at: http://content.healthaffairs.org. Accessed August 10, 2005.
18. US Department of Health and Human Services, Agency for Healthcare Research and Quality. National Healthcare Quality Report 2004. Available at: http://www.qualitytools.ahrq.gov/qualityreport. Accessed August 10, 2005.
19. Health Care Quality Glossary. Overview. The Russia-United States of America Joint Commission on Economic and Technological Cooperation, The Health Committee, Access to Quality Health Care. Agency for Health Care Policy and Research, Rockville, Md. 1999:26. Available at http://www.ahrq.gov/qual/hcqgloss.htm. Accessed March 14, 2005.
20. Nelson EA, Bradley MD. Dressings and topical agents for arterial leg ulcers. Cochrane Database. 2003;1:CD001836.
21. Moore ZEH, Cowman S. Wound cleansing for pressure ulcers. Cochrane Database. 2005;4:CD004983.
22. Bergin SM, Wraight P. Silver-based wound dressings and topical agents for treating diabetic foot ulcers. Cochrane Database. 2006;1:CD005082
23. Institute for Healthcare Improvement. Leadership guide to patient safety. Available at http://www.ihi.org/IHI/Results/WhitePapers/LeadershipGuidetoPatientSafetyWhitePaper.htm. Accessed August 14, 2006.
24. Beitz JM. Overcoming barriers to quality wound care: a systems perspective. Ostomy Wound Manage. 2001;47(3):56–64.
