



Notes on Practice: “Stretching” Negative Pressure Wound Therapy: Can Dressing Change Interval be Extended in Patients with Open Abdomens?
Negative pressure wound therapy (NPWT) has evolved significantly since its humble beginnings as an improvised vacuum-based surgical wound dressing. Now viewed as a safe, patient- and provider-friendly, effective option in wound management, modern applications of NPWT include treatment of infected surgical wounds, traumatic wounds, open abdominal wounds, diabetic and pressure ulcers, wounds with exposed bone and hardware, burn wounds, and venous stasis ulcers.1 New applications for NPWT technology continue to evolve and understanding of NPWT dressing-tissue interactions is growing.2
The classic paradigm of NPWT dressing changes is based on the recommended interval of 48 hours in non-infected wounds3; however, whether NPWT dressings can be safely changed on a less frequent basis in this setting of non-infected wounds as well as open abdominal wounds has not yet been determined. Few clinical reports have examined this question (many of them indirectly).4-8 This preliminary report evaluates the interval between NPWT dressing changes among 60 patients with open abdominal (OA) wounds and assesses its potential effect on outcomes.
Materials and Methods
A retrospective database was created using chart review data from all patients with open abdomens (OA) at St. Luke’s Regional Trauma Center (a member of the University of Pennsylvania Trauma Network) from September 2001 to January 2006. The data were abstracted by single investigator and included demographics (age and gender), primary diagnoses at the time of laparotomy, surgical techniques utilized, types of wound closure, complications associated with OA, observed 28-day mortality, and complications involving enteric fistula, abscess, enteric leak, pressure ulceration, and deep venous thrombosis (DVT).
Calculated parameters included Simplified Acute Physiology Score (SAPS II) and predicted 28-day mortality9; the former was utilized because of its applicability to both traumatic and non-traumatic etiologies and recorded at the time the patient was determined to need OA management. A recent comparison study of six prediction models among patients admitted to the intensive care unit demonstrated that SAPS II provided accurate overall mortality prediction.10
Resource utilization measurements included hospital length of stay (LOS) starting at the point of initiation of the OA approach to patient discharge or death and time to abdominal closure, as well as procedures per patient and the average number of days between procedures until abdominal closure.
Operative/Procedural Management
All patients were managed according to a previously published treatment algorithm for OA patients.11 In the immediate postoperative period, all patients underwent NPWT. Two NPWT techniques were commonly employed according to surgeon preference: 1) polyethylene-covered surgical towel with suction drains layered above the towel and covered with an impervious adhesive drape or 2) a commercially prepared sponge device (V.A.C.® System, KCI USA, San Antonio, Tex).
All patients underwent re-exploration within 6 to 48 hours depending on clinical stability. When possible, a tension-free primary fascial closure was performed at that time – such closure performed within 24 hours of the initial surgery was termed early delayed primary closure (DPC). If patients continued to manifest clinical characteristics that obviated abdominal closure (eg, continued bleeding, bowel or retroperitoneal edema, gross contamination), NPWT was continued. Primary fascial closure within 7 days utilizing NPWT was termed DPC with NPWT.
Patients using prolonged NPWT (>7 days) were re-evaluated after definitive operative therapy and physiologic restoration was complete. When possible, primary fascial closure was performed. If the patient had lost abdominal domain, one of the two management options was entertained. Open wounds exhibiting gross contamination at any time during the resuscitation were managed as planned ventral hernias (PVH).
Patients with PVH had a split-thickness skin graft (STSG) ± vicryl mesh placed over the OA wound. Placement of vicryl mesh was based on the presence or absence of omental coverage over the underlying bowel. If ample omentum was present and no bowel was exposed, vicryl mesh was not used. If coverage of exposed bowel was needed, vicryl mesh was utilized before skin grafting. A STSG was not placed until a healthy, clean granulation bed formed. Abdominal wall reconstruction would be performed on these patients at a later time.
Patients without gross contamination had a Velcro® Wittmann Patch™ (WP; StarSurgical, Burlington, WI) sewn to their fascia.11 The Velcro® patch was advanced daily until the fascial edges could be approximated primarily. After each advancement, the patient was observed for any signs of intra-abdominal hypertension (high peak airway pressures, oliguria, decreased cardiac output). Patients who failed fascial closure using the WP were received either STSG coverage or skin flap closure (SFC) over a bioprosthetic fascial repair (Alloderm™, LifeCell Corp, Branchburg, NJ; or Permacol™, Tissue Science Laboratories, Covington, Ga) plus STSG coverage of the resulting lateral abdominal skin relaxing incision.12 Negative pressure wound therapy dressings placed over skin grafts were left in place for 4 to 5 days.
Statistical analysis. Statistical analysis was performed using SPSS for Windows™ (Chicago, Ill) software. Descriptive statistics utilized included categorical data as well as continuous variables (reported as mean ± standard deviation). Chi-square statistic was used to analyze categorical data. Student’s t-test statistic was utilized in analysis of continuous variables. Statistical significance was set at alpha = 0.05.
Results
Of the 60 patients with open abdomen (OA) managed from 2001 to 2006, 35 were non-trauma patients (NTP) and 25 were trauma patients (TP). Non-trauma patients were significantly older than TP (60.9 ± 15.9 and 38.3 ± 15.0 years, respectively). The NTP group included 17 men and 18 women and the TP group had 17 men and eight women (see Table 1). The most common diagnoses on initial presentation among NTP patients were perforated viscus (13 out of 35) and abdominal compartment syndrome following major abdominal operation (six out of 35). Among the 25 TP patients, the most common diagnoses were severe splenic (eight) and blunt liver injury (five), alone or in combination.
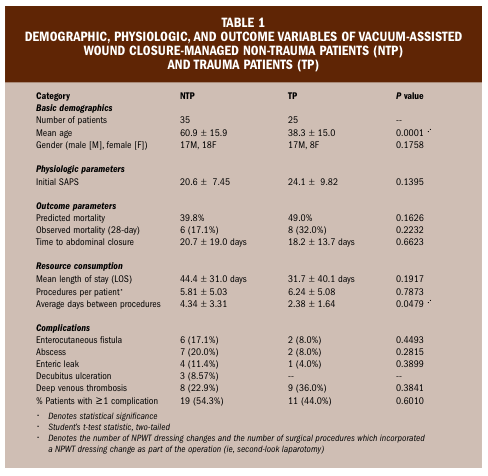 The initial mean SAPS score was not statistically different between the two groups (NTP: 20.6 ± 7.45; TP: 24.1 ± 9.82; P = 0.1395). The predicted mortality, as determined by SAPS scores, was 39.8% and 49.0% for NTP and TP, respectively (P = 0.1626). The observed 28-day mortality was 17.1% and 32.0% for NTP and TP, respectively (P = 0.1177).
The initial mean SAPS score was not statistically different between the two groups (NTP: 20.6 ± 7.45; TP: 24.1 ± 9.82; P = 0.1395). The predicted mortality, as determined by SAPS scores, was 39.8% and 49.0% for NTP and TP, respectively (P = 0.1626). The observed 28-day mortality was 17.1% and 32.0% for NTP and TP, respectively (P = 0.1177).
Mean time to abdominal closure was 20.7 ± 19.0 and 18.2 ± 13.7 days for NTP and TP, respectively (P = 0.6623). The hospital length of stay (LOS) was not significantly different between TP and NTP, with a trend toward longer LOS for NTP (44.4 ± 31.0 days for NTP versus 31.7 ± 40.1 days for TP, P = 0.1917). The average number of procedures per patient was 5.81 ± 5.03 for NTP and 6.24 ± 5.08 for TP (P = 0.7873), with an average of 4.34 and 2.38 days between procedures for NTP and TP, respectively (P = 0.0479).
Abdominal closure methods included DPC (in 20% of patients), attempted WP in 8%, successful WP-aided closure in 15%, STSG ± vicryl mesh in 33%, and skin flap closure in 12%. The remaining 23% of patients died before definitive abdominal closure.
Overall, both TP and NTP groups had a significant rate of complications, with at least one complication in 54% of NTP and 44% of TP.
Discussion
Despite the evolving number of indications for NPWT, some controversial points persist regarding this modality. Specifically, it has not been definitively determined whether the current recommended 24- to 72-hour NPWT dressing change regimen is optimal. While it is appropriate to change NPWT dressings frequently (ie, every 12 to 24 hours) in the setting of severe and moderate wound contamination, it seems that dressing change regimens in the setting of minimally contaminated and clean wounds may be spaced farther apart than the currently recommended 24- to 72-hour interval.
Potentially important differences between more frequent (every 24 to 72 hours) and less frequent (every 72 to 144 hours) NPWT dressing change regimens for minimally contaminated and clean wounds include: 1) cost considerations associated with dressing supplies, 2) frequency of the unpleasant and frequently painful dressing change experience, and 3) differences in the amount of healthcare personnel and/or operating room resources involved.
This review of NPWT data shows that NTP treated with dressing changes 4.34 days apart demonstrated similar mortality, morbidity, time to abdominal closure, and length of stay figures when compared to TP. Trauma patients were, on average, treated with NPWT dressing change every 2.38 days. Due to the retrospective nature of this study, ascribing the above observations to specific clinical parameters or patterns of practice at the authors’ institution is difficult. However, what is certain is that NTP were treated successfully utilizing dressing changes, on average, nearly two times less frequently than TP. In addition, NPWT dressings placed over skin grafts were kept in place between 4 and 5 days in this study.
Given other published reports and series, it appears that support is emerging for less frequent NPWT dressing changes.4-8 Negative pressure wound therapy applied over skin grafts can be safely left in place for 5 days.5,6 A 7-day regimen of NPWT dressing changes was used successfully in the setting of an extensive soft tissue defect following resection of deep infiltrating leiomyosarcoma, with no observed infectious complications.7 Reports utilizing an adjunctive silver-based dressings combined with NPWT, with significant labor- and cost-related savings secondary to a less frequent 5-day and 7-day dressing change regimens, seem encouraging.4,8
If proven safe, the potential implications of less frequent NPWT dressing changes would be noteworthy. In addition to altering the previously accepted dressing change paradigm, this new methodology would allow for significant savings from both human resource utilization and monetary perspectives. In addition, the less frequent dressing changes could be performed more conveniently on an outpatient basis, with potentially less patient discomfort and improved cost savings compared to inhospital treatment or more frequent outpatient/home care visits. Given the potential benefits of less frequent (>72 hours) NPWT dressing changes, further prospective evaluation of this emerging methodology should be conducted.
Conclusion
In this study, non-trauma patients with open abdomens underwent NPWT dressing changes at significantly greater intervals than trauma patients with open abdomens. Given the physiologic score similarity between trauma patients and non-trauma patients and the fact that no statistically significant differences were noted in mortality, morbidity, time to wound closure, and resource consumption between these groups, further study of feasibility of less frequent NPWT dressing changes (every 72 to 144 hours) in patients with open abdominal wounds appears to be warranted.
1. Venturi ML, Attinger CE, Mesbahi AN, Hess CL, Graw KS. Mechanisms and clinical applications of the vacuum-assisted closure (VAC) device: a review. Am J Clin Dermatol. 2005;6(3):185-194.
2. Greene AK, Puder M, Roy R, et al. Microdeformational wound therapy: effects on angiogenesis and matrix metalloproteinases in chronic wounds of 3 debilitated patients. Ann Plast Surg. 2006;56(4):418-422.
3. V.A.C.® Therapy Clinical Guidelines. San Antonio, Tex: KCI, USA; October 2005.
4. Comparative studies of combination therapy Silverlon®/VAC™ vs. VAC™ alone. Available at: http://www.silverlon.com/studies/vac_dressing_combination.html. Accessed, June 12, 2006.
5. Avery C, Pereira J, Moody A, et al. Negative pressure wound dressing of the radial forearm donor site. Int J Oral Maxillofac Surg. 2000;29(3):198-200.
6. Senchenkov A, Knoetgen J, Chrouser KL, Nehra A. Application of vacuum-assisted closure dressing in penile skin graft reconstruction. Urology. 2006;67:416-419.
7. Bartels CG, Voigt C, Blume-Peytavi U, et al. The vacuum sealing technique. A new procedure to cover soft tissue defects after resection of leiomyosarcoma. Hautarzt. 2001;52(7):653-657.
8. Carson SN, Rodriguez A, Hebert J, et al. Healing skin grafts over chronic wounds with vacuum assisted closure and silver dressings. Available at: http://www.silverlon.com/studies/HSG001.pdf. Accessed, June 12, 2006.
9. Reiter A, Mauritz W, Jordan B, et al. Improving risk adjustment in critically ill trauma patients: the TRISS-SAPS Score. J Trauma. 2004;57(2):375-380.
10. Arabi Y, Al Shirawi N, Memish Z, et al. Assessment of six mortality prediction models in patients admitted with severe sepsis and septic shock to the intensive care unit: a prospective cohort study. Crit Care. 2003;7(5):R116-122.
11. Cipolla J, Stawicki SP, Hoff WS, et al. A proposed algorithm for managing the open abdomen. Am Surg. 2005;71(3):202-207.
12. Guy JS, Miller R, Morris JA Jr, et al. Early one-stage closure in patients with abdominal compartment syndrome: fascial replacement with human acellular dermis and bipedicle flaps. Am Surg. 2003;69(12):1025-1028.
