



Impact of Hypernatremia on Burn Wound Healing: Results of an Exploratory, Retrospective Study
Abstract
Severely burned patients need extensive initial fluid resuscitation. Formulas to calculate fluid needs during burn shock are well established. However, protocols for normalizing circulating fluid volume after cellular integrity has recovered do not exist.
Resultant electrolyte shifts can cause hypernatremia, a possible sign of hypovolemia, which may in turn result in decreased tissue perfusion, subsequently affecting burn wound healing. The purpose of this retrospective chart review was to explore the hypothesis that hypernatremia in burn patients is a possible sign of systemic dehydration and that dehydration may affect burn wound skin graft take. Medical chart data from otherwise healthy burn victims with deep partial-thickness burns (total burn surface area [TBSA] >10%) who underwent skin grafting 7 days post injury were reviewed. Thirty (11 female, 19 male) patients with an average TBSA of 30% (± 11%) and an Abbreviated Burn Severity Index (ABSI) score of 7.9 (± 1.8) were included. Of those, 17 had normal average serum levels between day 2 and 6 following injury and 13 developed hypernatremia (serum sodium ≥146 mmol/L) an average of 5.5 days (± 1.5) after injury.
Patients in this group underwent an average of 1.3 (± 0.8) re-grafting procedures compared to 0.35 (± 0.5) for patients without hypernatremia (P = 0.001). There was good correlation (r = 0.525) between daily infusion-diuresis ratios (IDR) and serum sodium levels, as well as between serum sodium levels and re-skin grafting occurrences (r = 0.62). The results indicate that research to confirm that hypernatremia is an indicator of dehydration and affects skin graft take is warranted and that protocols to optimize fluid volume following burn shock treatment are needed.
Potential Conflicts of Interest: none disclosed
 Water and electrolyte imbalances can provoke potentially devastating, irreversible neurologic, pulmonary, cardiac, or renal sequelae.1-4 Hypernatremia, defined as a serum sodium level ≥146 mmol/L, can be a laboratory indicator of hypovolemia.4 Hypernatremia that develops in hospital is usually iatrogenic, resulting from inadequate or inappropriate fluid prescription. 5 Nonspecific symptoms like lightheadedness, nausea, headache, fatigue, and confusion may be consistent in alert hypernatremic patients4; in unconscious patients, laboratory results have to be observed vigilantly because of the lack of these symptoms. Acute and chronic hypernatremia are associated with increased mortality in critically ill patients.6-10
Water and electrolyte imbalances can provoke potentially devastating, irreversible neurologic, pulmonary, cardiac, or renal sequelae.1-4 Hypernatremia, defined as a serum sodium level ≥146 mmol/L, can be a laboratory indicator of hypovolemia.4 Hypernatremia that develops in hospital is usually iatrogenic, resulting from inadequate or inappropriate fluid prescription. 5 Nonspecific symptoms like lightheadedness, nausea, headache, fatigue, and confusion may be consistent in alert hypernatremic patients4; in unconscious patients, laboratory results have to be observed vigilantly because of the lack of these symptoms. Acute and chronic hypernatremia are associated with increased mortality in critically ill patients.6-10
Severely burned patients need extensive fluid resuscitation to survive the acute phase of burn shock.11 Microvascular integrity is lost and a plasma-like fluid leaks into the interstitial space, producing edema. The time after injury at which capillary integrity is restored differs among individuals.11 During this time, the plasma volume must be maintained to ensure adequate oxygen delivery to the vital organs and peripheral tissues. After acute phase fluid resuscitation and recovery of cellular integrity, the circulating fluid volume has to be normalized; extensive water and electrolyte shifts can be provoked. Systemic hypovolemia can decrease perfusion in burn wounds and affect burn wound healing. Skin graft take is achieved by revascularization of the grafted skin from a well prepared tissue bed on the recipient site. Without sufficient recipient site tissue bed perfusion, revascularization cannot be realized.12-14
Zawacki et al15 demonstrated in an experimental animal burn model (guinea pigs) that the primary cause of burn wound necrosis is local wound dehydration. Further, the results of their study demonstrated that capillary stasis may be reversed and necrosis prevented by appropriate topical wound hydration. Using an experimental skin burn model, Kuroda et al16 showed that compared to normonatremic rats, the demarcating borderline of leukocyfic infiltration was deeper in hypernatremic rats after burn injury. The authors concluded that wound depth progression may be caused by osmotic injury. In an experimental study in rats, Harada et al17 described increased apoptosis of hair follicle cells in second-degree burn wounds under hypernatremic conditions.
The purpose of this retrospective study was to explore the hypothesis that hypernatremia in burn patients is a possible laboratory sign for systemic dehydration and that dehydration may affect burn wound skin graft take.
Materials/Methods
A 4-year retrospective chart review of all patients admitted to the authors’ burn unit was conducted. All charts were reviewed by the author. The rights and dignity of all subjects involved in this retrospective study were protected in accordance to the Declaration of Helsinki.
Variables. To facilitate comparisons, the following variables were abstracted: patient gender, age, total burn surface area (TBSA), Abbreviated Burn Severity Index (ABSI), daily infusion-diuresis ratio (IDR), serum sodium, serum creatinin, and number of second-degree burn wound skin grafts. Patient age was recorded because increased age may be associated with preexisting micro- or macroangiopathy, which can affect tissue perfusion. A high TBSA increases the risk of more extensive systemic consequences and may require a higher daily fluid intake to compensate for hypovolemia. Daily IDR, serum sodium, and creatinin were analyzed to examine the relationship between hypernatremia and hypovolemia.
Need for fluid intake is higher immediately after burn injury than after a few days; therefore, two time periods were analyzed — 1) the first 24 hours following injury and 2) day 2 to day 6 following injury. The period from day 2 to day 6 was defined retrospectively to evaluate the potential impact of IDR on the incidence of hypernatremia. Inclusion/exclusion criteria. To obtain comparable data, only otherwise healthy burn victims with a TBSA >10% and deep partial-thickness burns located on the back who underwent skin grafting on day 7 after burn injury were included. Patients with inhalation injury, cardiac or renal dysfunction, diabetes mellitus, or a postoperative wound infection were excluded from this study. All patients were mechanically ventilated for a minimum of 5 days after skin-graft surgery.
Patient care procedures. During the first 24 hours after burn injury, fluid resuscitation was performed, guided by the Parkland-Formula with 4 mL/kg/TBSA% of Ringer’s lactate.18,19 Fluid equilibration during the post-burn shock phase was achieved using furosemid in combination with colloid infusion and Ringer’s solution.
All burn wounds initially were debrided and covered with fluid antiseptic dressing (Serasept® 0.04%, Serag-Wiessner KG, Nalia, Germany), which was changed daily. All patients underwent a first skin-graft operation on day 7 after burn injury. A team of specialized plastic surgeons performed all operations. In case of a relevant skin-graft loss, re-operations were performed within 14 days after relevant skin graft loss was detected, depending on patients’ general condition and/or wound infection. Wound dressing after skin grafting included a 10% povidone iodine salve; no other wound dressing was used.
Data and statistical analysis. All variables were entered in a spreadsheet and analyzed using SPSS® 15.0 (SPSS Inc., Chicago, IL, US). To estimate a significant difference of mean values between patients with and without hypernatremia, the Mann-Whitney-U-Test was performed and the chi-square-test was used to detect significant differences of categorical variables between both subgroups (re-skin grafting: yes or no). Results are written in mean value ± standard deviation. Linear regression was performed to examine relevant relationships. A correlation coefficient (r) <0.4 was defined as poor correlation, r = 0.4 – 0.7 was defined as a good correlation, and r >0.7 showed a high correlation between both subgroups.
Results
 Thirty (11 female; 19 male) healthy patients with a mean age of 47 ± 17 years (range: 17–83 years), a TBSA of 30% ± 11% (range: 20%–70 %), and a mean ABSI score of 7.9 ± 1.8 (range: 4–11), met the chart review inclusion criteria and were included in the study.
Thirty (11 female; 19 male) healthy patients with a mean age of 47 ± 17 years (range: 17–83 years), a TBSA of 30% ± 11% (range: 20%–70 %), and a mean ABSI score of 7.9 ± 1.8 (range: 4–11), met the chart review inclusion criteria and were included in the study.
Of those, 17 were normonatremic, mean age of 50 ± 16 years (range: 21–72 years), mean TBSA of 28% ± 10% (range: 20%–60 %), and a mean ABSI score of 7.7 ± 2 (range: 4–11). Mean serum-creatinine value (day 1 to day 6) was 72 ± 15 µmol/L (range: 49–95 µmol/L) (see Table 1).
Thirteen patients had hypernatremia, mean age of 43 ± 19 years (range: 17–83 years), mean TBSA of 33% ± 13% (range: 20%–70 %), and mean ABSI score of 8.2 ± 1.7 (range: 5–11). Mean serum-creatinine value (day 1 to day 6) was 86 ± 12 µmol/L (range: 68–108 µmol/L) (see Table 1).
No significant difference was found in initial (24 hours after burn injury) fluid resuscitation between both groups (normonatremia versus hypernatremia: 2.9 ± 1.4 mL/kg/TBSA% versus 4.2 ± 2.7 mL/kg/TBSA%; P = 0.25). Hypernatremia occurred on day 5.5 ± 1.5 (range: day 4 to day 8) and remained ≥146 mmol/L for 5.8 ± 4 days (range: day 2 to day 14).
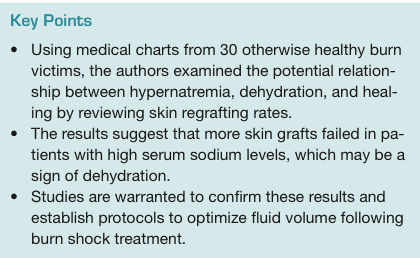
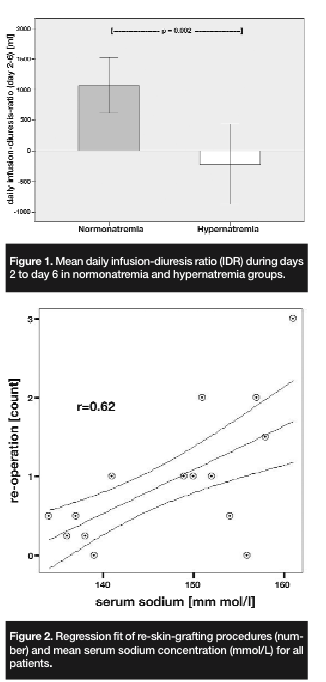
A significantly higher number of re-skin grafts was noticed in the hypernatremic group (normonatremia versus hypernatremia: 0.35 ± 0.5 versus 1.3 ± 0.8; P = 0.001). A significant association between hypernatremia and re-skin grafting was observed (odds ratio: 10.08; confidence interval: 1.66 – 61.3). Statistical analysis of IDR and serum-creatinin levels during days 2 to 6 showed a significantly higher amount of daily IDR in patients with hypernatremia compared to those with normal sodium levels (1,067 ± 889 mL versus -225 ± 1,089 mL; P = 0.002 (see Figure 1) and significantly higher serum-creatinine in hypernatremic patients than in normonatremic patients (72 ± 15 µmol/L versus 86 ± 12 µmol/L, respectively; P = 0.01). There was good linear correlation (r = 0.525) between daily IDR and serum sodium values for days 2 to 6, as well as between serum sodium and re-skin graft count (r = 0.62) (see Figure 2). The correlation between TBSA and hypernatremia as well as between TBSA and re-skin grafting was poor (r = 0.28 and r = 0.27, respectively).
Discussion
Deep partial-thickness burns are frequently covered with skin grafts to facilitate expedient healing.13,20 Partial skin graft failure is often unavoidable in severely burned patients (TBSA >10%). Risk factors for skin-graft loss include inadequate burn wound excision, shearing force, wound infection, and marginal tissue bed — ie, after tangential burn wound debridement, only a thin residual dermis layer remained in the burn wound. 13
The burn wound has to be well prepared before skin grafting can be performed. From their work on guinea pig burns in 1949, Sevitt et al21 concluded that capillary stasis in burn wounds was irreversible and that the most deeply situated hair follicles become necrotic when stasis involves the capillaries in the deepest part of the dermis. In 1953, Jackson et al’s22 observations of human burns confirmed Sevitt's conclusions. However, in 1969, Jackson et al23 noted that tangential excision of a recent burn revealed a dermal surface within the zone of stasis. They stated that the same human dermal surface that appeared histologically “dead” if ungrafted and dressed with petrolatum gauze bled from a few scattered arterioles and accepted an autograft if tangential excision was performed.
If the burn wound is well treated, capillary stasis may be partially reversible and the total burn wound area that has to be surgically debrided and skin grafted can be decreased. Burn wound necrosis can be diminished by using appropriate dressings to prevent local burn wound dehydration. Per Zawacki et al’s15 animal study involving 12 guinea pigs, a complete reversal of capillary stasis and burn wound necrosis was observed if the blister was replaced by porcine skin graft to prevent wound dehydration. Local burn wound dehydration has to be avoided until re-epithelialization is complete.
Prolonged blood supply interference in the zone of stasis also may deepen tissue necrosis and systemic dehydration can induce cell death and lead to an increase in the depth of necrotic tissue. Even a short period of hypernatremia leads to an induction of apoptosis and deepening of the burn wound.16,17 In an experimental skin burn model in Wistar rats, Harada et al17 observed a relationship between systemic hypernatremia and apoptosis induction. Kuroda et al16 found that systemic hypernatremia in rats deepens the demarcating borderline of leukocytic infiltration in burn wounds. The phenomenon of burn wound deepening is an important and unsolved problem for clinicians who care for more severely burned patients. The cause of hypernatremia following hospital admission is commonly iatrogenic.4-6 In severely burned patients, hypernatremia is frequently reported due to extensive initial fluid resuscitation/removal treatment conditioned by capillary hyperpermeability.11,18,20 Thus, hypernatremia after burn injury is often unavoidable, even in specialized burn centers.
Results of the current retrospective study showed a significant correlation between hypernatremia and skin-graft take after burn injury. Patients with normal sodium levels had significantly fewer re-skin grafting procedures than patients with hypernatremia. This led the researchers to hypothesize that hypernatremia in burn patients is a laboratory sign for systemic dehydration which, in turn, compromises perfusion of the burn wound. Also, if daily diuresis is higher than infusion over several days, this may be another indicator for dehydration. The wounds of burn victims should be well prepared before skin grafting is performed.
Several formulas facilitate calculation of fluid administration needs during burn shock. However, guidelines for fluid removal, including type and amount of diuretic agents to use and optimal IDR to minimize dehydration risk during the post-resuscitation phase, do not exist.11 Research to establish an optimal fluid-removal protocol to avoid systemic dehydration and optimize skin-graft-take and prospective, randomized, multicenter trials are needed.
Study Limitations
This was an exploratory study and the results should be interpreted with caution. The sample size of this retrospective chart review is small and although the two groups were very similar, post-burn shock fluid removal strategies, including the use of diuretics and intravenous fluids administered, are not standardized. Different types of saline (Ringer’s solution, dextrose 5%, sodium chloride) and colloid infusions (gelatin, hydroxyethylstark) were used. Finally, the study design and the lack of clearly defined criteria for re-skin grafting also limits the ability to generalize the results, including the observed rate of hypernatremia after burn injury.
Conclusions
Research suggests that systemic dehydration in burn patients may have a negative impact on skin-graft take and that hypernatremia may be an indicator of systemic relevant hypovolemia. The results of this retrospective chart review appear to confirm this hypothesis. Additional studies to explore the relationship between skin graft take and fluid removal strategies to establish optimal fluid removal strategies and avoid water imbalance in severely burned patient are warranted.
1. Adrogue HJ, Madias NE. Hypernatremia. N Engl J Med. 2000;342(20):1493–1499.
2. Fisher LA, Ko N, Miss J, et al. Hypernatremia predicts adverse cardiovascular and neurological outcomes after SAH. Neurocrit Care. 2006;5(3):180–185.
3. Hoorn EJ, Betjes MG, Weigel J, Zietse R. Hypernatraemia in critically ill patients: too little water and too much salt. Nephrol Dial Transplant. 2008;23(5):1562–1568.
4. Lin M, Liu SJ, Lim IT. Disorders of water imbalance. Emerg Med Clin North Am. 2005;23(3):749–770, ix.
5. Snyder NA, Feigal DW, Arieff AI. Hypernatremia in elderly patients. A heterogeneous, morbid, and iatrogenic entity. Ann Intern Med. 1987;107(3):309–319.
6. Janz T. Sodium. Emerg Med Clin North Am. 1986;4(1):115–130.
7. Mandal AK, Saklayen MG, Hillman NM, Markert RJ. Predictive factors for high mortality in hypernatremic patients. Am J Emerg Med. 1997;15(2):130–132.
8. O’Donoghue SD, Dulhunty JM, Bandeshe HK, Senthuran S, Gowardman JR. Acquired hypernatraemia is an independent predictor of mortality in critically ill patients. Anaesthesia. 2009;64(5):514–520.
9. Palevsky PM, Bhagrath R, Greenberg A. Hypernatremia in hospitalized patients. Ann Intern Med. 1996;124(2):197–203.
10. Polderman KH, Schreuder WO, Strack van Schijndel RJ, Thijs LG. Hypernatremia in the intensive care unit: an indicator of quality of care? Crit Care Med. 1999;27(6):1105–1108.
11. Pham TN, Cancio LC, Gibran NS. American Burn Association practice guidelines burn shock resuscitation. J Burn Care Res. 2008;29(1):257–266.
12. Desai MH, Herndon DN, Broemeling L, Barrow RE, Nichols RJ Jr, Rutan RL. Early burn wound excision significantly reduces blood loss. Ann Surg. 1990;211(6):753–759; discussion 759–762.
13. Herndon DN. Total Burn Care, 3rd ed. Philadelphia, PA: Saunders;2007.
14. Zellweger G (ed). Die Behandlung der Verbrennungen: Praktische Hinweise für Diagnose, Therapie, Rehabilitation. Köln: Deutscher Ärzte Verlag;1985.
15. Zawacki BE. Reversal of capillary stasis and prevention of necrosis in burns. Ann Surg. 1974;180(1):98–102.
16. Kuroda T, Harada T, Tsutsumi H, Kobayashi M. Hypernatremia deepens the demarcating borderline of leukocytic infiltration in the burn wound. Burns. 1997;23(5):432–437.
17. Harada T, Izaki S, Tsutsumi H, Kobayashi M, Kitamura K. Apoptosis of hair follicle cells in the second-degree burn wound under hypernatremic conditions. Burns. 1998;24(5):464–469.
18. Baxter CR. Fluid volume and electrolyte changes of the early postburn period. Clin Plast Surg. 1974;1(4):693–703.
19. Baxter CR, Shires T. Physiological response to crystalloid resuscitation of severe burns. Ann NY Acad Sci. 1968;150(3)(1):874–894.
20. Heimbach D, Engrav L, Grube B, Marvin J. Burn depth: a review. World J Surg. 1992;16(1):10–15.
21. Sevitt S. Local blood-flow changes in experimental burns. J Pathol. 1949;61:427.
22. Jackson DM. [The diagnosis of the depth of burning.]. Br J Surg. 1953;40(164):588–596.
23. Jackson DM. Second thoughts on the burn wound. J Trauma. 1969;9(10):839–862.
