



Skin Matters: Effectiveness of a Non-Petrolatum Emollient Cream in Pediatric Care
Adapted from a poster presented at the Symposium on Advanced Wound Care, San Antonio, Tex, April 30–May 3, 2006
The skin of premature neonates may be overly susceptible to skin tears due to decreased skin elasticity. In addition, a risk exists for coagulase-negative Staphylococcus epidermidis infection or fungal infection in neonates when petrolatum products are used as emollients to control transepidermal water loss.1,2 Dry skin also is an issue for the pediatric population, with as many as 50% of PICU admissions exhibiting this symptom.3 Current clinical practice guidelines recommend applying an emollient every 12 hours or as needed; however, the acuity of the patients and current practices typically prevent compliance with this guideline.4
The authors wanted to document whether an emollient (Sween® 24 Superior Moisturizing Skin Protectant Cream, Coloplast Corp., Marietta, Ga) used once a day could effectively reduce xerosis.
Three case studies were used as part of the product evaluation to determine the efficacy of the emollient cream on neonatal and pediatric skin. The non-petrolatum emollient cream was applied daily after bathing. Unit doses were used to avoid container contamination.2 Cases were followed for 3 weeks. Xerosis was documented using a 4-point scale where 0 = absent, 1 = mild dry skin with minimum flaking, 2 = moderate dry skin with flaking, and 3 = severe dry skin with/without cracking/fissures.
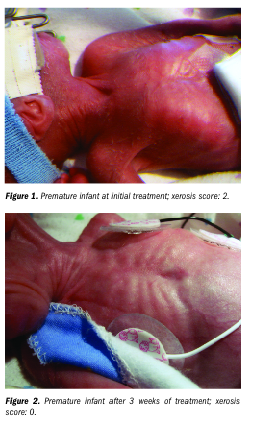
The first case involved a premature infant born at 25 weeks weighing 610 g. The baby’s skin was dry, scaly, and very fragile; the skin was susceptible to skin tears due to decreased skin elasticity. The non-petrolatum emollient cream was used for 3 weeks; weekly improvement was noted and by the second week, no scaly or dry skin was detected. By week 3, the skin exhibited a healthy appearance and improved elasticity (see Figures 1 and 2).
The second case involved a 30-week-old neonate weighing 680 g. The baby was septic following birth with necrotizing enterocolitis. Initially, the skin was red, tight, and peeling. After 3-week treatment with the emollient, the skin was no longer red and suppleness was improved. By week 3, the skin was no longer dry or peeling (see Figures 3 and 4).
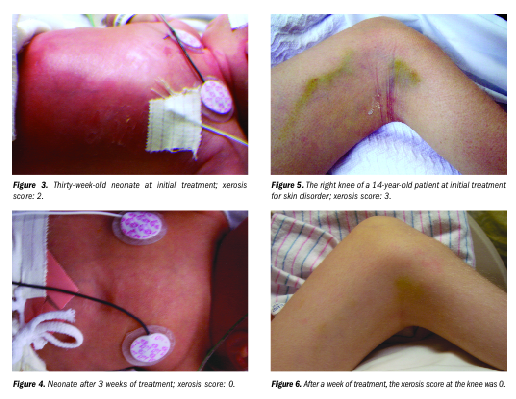
The third case involved a 14-year-old patient who weighed 27.2 kg at admission and suffered from seizures; this child had cerebral palsy since birth. The skin was dry and cracked at joints with skin breakage at the right knee. Generally, the skin was dry due to dehydration and emaciation. By day 7 of treatment, the skin at the knee was healed and moist (see Figures 5 and 6).
Post treatment, the skin of all three patients exhibited improved suppleness and was soft and free from breakdown; extra friction and multiple applications were avoided. The once-daily application was convenient and effective, with no adverse side effects or complications occurring as a result of emollient cream use. The product has become part of hospital protocol. Non-petrolatum creams should be a consideration for treatment of xerosis in young patients.
The Skin Matters series is made possible through the support of the Skin Health Division of Coloplast Corp., Marietta, Ga.
This article was not subject to the Ostomy Wound Management peer-review process.
1. Edwards W, Conner J, Gerdes J, et al. The effect of Aquaphor emollient ointment on nosocomial sepsis rates and skin integrity in infants of birthweight 500–1,000 grams. Presented at the Hot Topics Neonatology Conference, Washington, DC; 2005.
2. Campbell JR, Zaccaria E, Baker CJ. Systemic candidiasis in extremely low birthweight infants receiving topical petrolatum ointment for care: a case control study. Pediatr. 2000;105(5):1041–1045.
3. Suddaby E, Barnett S, Facteau L. Skin breakdown in acute care pediatrics. Pediatr Nurs. 2005;31(2):132–148.
4. Evidence-based Clinical Practice Guideline Development Team. Evidence-based clinical practice guideline. Neonatal skin care. AWHONN;2001.
