



Continence Coach: Differential Assessment of Trunk Wounds: Pressure Ulceration versus Incontinence-associated Dermatitis versus Intertriginous Dermatitis
All wound clinicians know that accurate determination of etiology (and implementation of measures to address etiology) is the critical first step in effective management of any wound; attention to glycemic control, perfusion, nutrition, and evidence-based topical therapy are unlikely to result in wound healing if the cycle of injury is not interrupted. When dealing with trunk wounds, the clinician must accurately differentiate between wounds that are pressure-related and those caused by some combination of moisture and friction (incontinence-associated dermatitis [IAD] and intertriginous dermatitis [ITD]).1 Guidelines for differential assessment are the focus of this column. Several factors have led to our current state of confusion regarding differential assessment and terminology related to trunk wounds. One is the historical tendency to label all trunk wounds pressure ulcers. This has been reinforced by our current pressure ulcer staging system, which includes partial-thickness wounds; Stage II pressure ulcers are defined as “partial-thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum-filled or serosanguinous-filled blister.”2 The inclusion of partial-thickness wounds in the staging system is understandable, because the system originally was designed simply to reflect the anatomic depth of the ulcer as opposed to reflecting the stages (process) of pressure ulcer development. In the last two iterations of the National Pressure Ulcer Advisory Panel (NPUAP) staging system2,3 the following caveat was added to the definition/description of Stage II ulcers: “This category should not be used to describe skin tears, tape burns, incontinence-associated dermatitis, maceration, or excoriation.” However, the inclusion of partial-thickness wounds in the pressure ulcer staging system continues to reinforce the belief that pressure ulcers can be “superficial” wounds.
The importance and impact of the staging system was underscored in a consensus session held at the Wound Ostomy Continence Nurses (WOCN) Society conference; the intent was to develop consensus statements related to differential assessment of moisture wounds versus pressure wounds. Many participants stated they were uncomfortable supporting any statement that appeared to contradict the staging system currently in place.4 This issue also has been addressed by the Shifting the Original Paradigm Expert (SOPE) Panel,5 which concluded, “Current numerical pressure ulcer classification systems (staging, grading, or categories) are problematic and misleading because they imply that pressure ulcers progress through defined stages (from I to IV)”; and “The current concept of the Stage/Grade II pressure ulcer is a misconception because these superficial skin injuries (outside in) are primarily due to moisture and friction.”
Another factor contributing to the confusion is the fact that patients at risk for pressure ulcers are also frequently at risk for IAD and ITD. For example, patients who are bedbound, immobile, incontinent, and diaphoretic are at risk for all three types of skin damage.
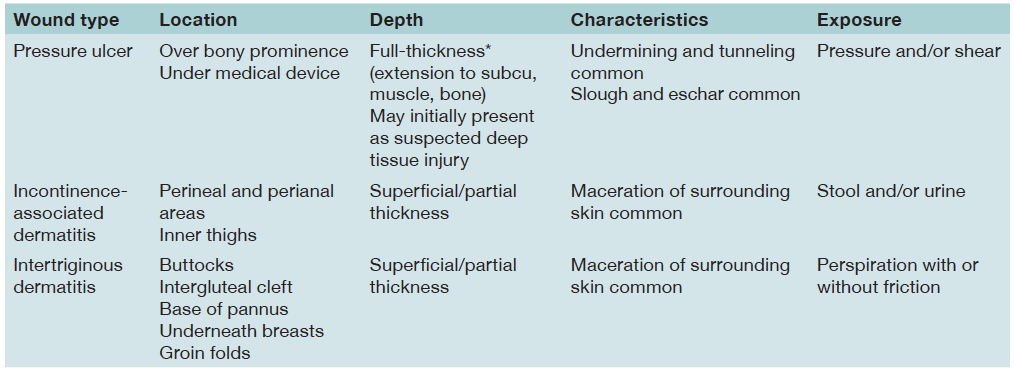 What does this mean for the clinician? What guidelines exist to help the clinician accurately differentiate moisture lesions from pressure-related wounds? A comparison of the pathology and clinical presentation of the various conditions provides major clues and substantive guidance. These guidelines are summarized in Table 1.
What does this mean for the clinician? What guidelines exist to help the clinician accurately differentiate moisture lesions from pressure-related wounds? A comparison of the pathology and clinical presentation of the various conditions provides major clues and substantive guidance. These guidelines are summarized in Table 1.
Pressure ulcers are ischemic ulcers caused by compression of the soft tissue and perfusing vessels; compression and blood vessel deformation cause a significant reduction in blood flow to all tissue layers between the bone and the skin. Current studies5-7 indicate the muscle tissue layer is the layer most vulnerable to diminished blood flow; thus, evidence strongly supports a “bottom-up” progression of pressure-related damage in which damage begins at the muscle layer and progresses toward the surface. Based on the fact that pressure ulcers result from ischemic damage beginning in the deep tissue layers, and Stage II ulcers represent loss of the epidermis with preservation of the deep dermis, subcutaneous tissue, and muscle, it seems unlikely that Stage II ulcers are ever caused by pressure. Thus, true pressure ulcers are typically characterized by full-thickness lesions in which tissue necrosis (ie, the presence of slough and/or eschar) is frequently evident, and they occur in areas where tissue is compressed between the bone and the skin surface or between deep tissues and a medical device.5
IAD is defined as an inflammatory response of the skin to prolonged or repetitive contact with urine, stool, or both. Early stages of IAD are characterized by erythema and tenderness, which may progress to patchy or extensive denudation; denudation may occur as a result of skin exposure to the enzymes in liquid stool or as a result of frictional forces applied to overhydrated macerated skin.8 IAD is a type of “top-down” injury; the pathology involves inflammation of the skin layers themselves, as opposed to ischemic damage involving the deeper tissue layers. IAD generally presents as erythema and denudation in areas exposed to stool and urine (perineal and perianal areas, inner thighs, and buttocks).8,9
ITD involves inflammation and denudation of the skin between opposing skin folds; the pathologic processes include maceration as a result of trapped moisture and friction caused by the opposing skin folds.8,9 ITD presents as a linear break in the skin (fissure), which may occur spontaneously in overhydrated skin or as a result of minor trauma (such as separating the buttocks to provide hygienic care). ITD is another type of “top-down” injury in that the pathology involves the skin layers themselves and not the deeper tissue. ITD is most likely to occur in the intergluteal cleft, underneath the breasts, underneath a pannus, or in groin folds, but can occur at the base of any fold where there is trapped moisture.9
Summary
Differential assessment of trunk wounds is a critical element of their effective management. In reviewing the pathology and typical presentation for pressure necrosis, IAD, and ITD, four factors provide guidance in differential assessment: location, depth, characteristics, and exposure. Pressure ulcers are full-thickness lesions located over bony prominences or under medical devices. IAD and ITD are superficial lesions that occur in areas exposed to urine and/or stool (IAD) or trapped perspiration (ITD). Undermining and tunneling are common features of pressure ulcers, but never occur with IAD or ITD. Similarly, pressure ulcers frequently present with tissue necrosis, whereas ITD and IAD are commonly associated with maceration of the surrounding skin.
Dr. Doughty is Director of the Emory University WOC Nursing Education Center, Atlanta, GA. The National Association For Continence is a national, private, nonprofit organization dedicated to improving the quality of life of people with incontinence. The NAFC’s purpose is to be the leading source for public education and advocacy about the causes, prevention, diagnosis, treatments, and management alternatives for incontinence.
This article was not subject to the Ostomy Wound Management peer-review process.
1. Mahoney M, Rozenboom B, Doughty D, Smith H. Issues related to accurate classification of buttocks wounds. J WOCN. 2011;38(6):635–642.
2. National Pressure Ulcer Advisory Panel; European Pressure Ulcer Advisory Panel. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guidelines. 2009. Washington, DC: NPUAP. Available at: www.npuap.org.
3. National Pressure Ulcer Advisory Panel. Pressure Ulcer Staging System. 2007. Washington, DC: NPUAP. Available at: www.npuap.org.
4. WOCN Society. Differential Assessment of Buttocks Lesions Consensus session at the WOCN Annual Conference. New Orleans, LA. June 2011.
5. Sibbald RG, Krasner D, Woo K, SOPE Panel. Pressure ulcer staging revisited: superficial skin changes and deep pressure ulcer framework. Adv Skin Wound Care. 2011;24(12):571–582.
6. Aoi N, Yoshimura K, Kadono T, Nakagami G, Iizuka S, Higashino T, et al. Ultrasound assessment of deep tissue injury in pressure ulcers: possible prediction of pressure ulcer progression. Plast Reconstr Surg. 2009;124(2):540–550.
7. Quintavalle P, Lyder C, Mertz P, Phillips-Jones C, Dyson M. Use of high-resolution, high-frequency diagnostic ultrasound to investigate the pathogenesis of pressure ulcer development. Adv Skin Wound Care. 2006;19(9):498–505.
8. Gray M, Beeckman D, Bliss D, Fader M, Logan S. Incontinence-associated dermatitis: review and update. J WOCN. 2012;39(1):61–74.
9. Black J, Gray M, Bliss D, Kennedy-Evans K, Logan S, et al. Moisture-associated skin damage. Part 2: Incontinence-associated dermatitis and intertriginous dermatitis: a consensus. J WOCN. 2011;38(4):359–370.
