


Active Leptospermum Honey and Negative Pressure Wound Therapy for Nonhealing Postsurgical Wounds
The use of negative pressure wound therapy (NPWT, V.A.C. Therapy®, KCI, San Antonio, TX) has grown rapidly over recent years. The modality creates a healing-friendly environment by promoting the growth of granulation tissue and removing exudate and infectious material. While the evidence base supporting this treatment grows, certain issues specific to NPWT require attention. According to the manufacturer’s specifications and in order to maximize the benefits of NPWT, all devitalized tissue (including eschar and hardened slough) should be removed as thoroughly as possible before NPWT application. This may require sharp or surgical debridement. If the patient is not a candidate for sharp debridement, an alternative debridement approach (ie, autolytic, enzymatic, or mechanical) must be implemented.1 Also, once NPWT is initiated, malodor upon dressing removal must be addressed. Malodor with occlusion has been well documented2-6 and may be related to bacteria7 and/or alterations in the skin, including altered epidermal lipids, DNA synthesis, epidermal cell turnover, pH, epidermal morphology, sweat glands, and stresses to the Langerhans cells.8 The combination of an occlusive dressing, necrotic tissue, and decreased dressing change frequency increases the potential for malodor. An odor filter, a standard piece of equipment on the various NPWT systems, is designed to control odor within the exudate receptacle but not at the wound site.
The following case report describes the use of active Leptospermum honey (ALH) paste (MEDIHONEY®, Derma Sciences, Inc., Princeton, NJ) in combination with NPWT to determine if this approach would help resolve debridement and odor concerns and provide a synergistic therapeutic effect. The components and properties of ALH, a medical grade honey, help prepare the wound bed: high osmolarity helps draw fluid from the wound and underlying tissue, aiding in debridement of slough and devitalized tissue,9,10 and physiochemical and antimicrobial characteristics11-13 have been reported to reduce or eliminate malodor14 via several mechanisms. First, bacteria preferentially metabolize glucose in the honey instead of the amino acids present in tissue and serum, resulting in the formation of lactic acid (as opposed to ammonia, sulfur, and amines). Second, the antimicrobial action of honey reduces the presence of bacteria — and subsequently their associated ability to cause odor — in the wound bed.13 This particular type of honey, unlike all other honeys, does not lose its antimicrobial activity in the presence of wound fluid.11,12
Case Report
Thirty-two-year-old Mr. Q had undergone extensive abdominal surgery and a hernia repair with mesh that was left open to heal by secondary intention. The mesh had become infected, requiring subsequent re-exploration of the abdomen and removal of the infected mesh. Mr. Q was discharged to home receiving NPWT to bridge the abdominal wall margins and prepare the wound bed for surgical closure.
After several weeks of NPWT at home, exudate and malodor increased and healing stalled. Mr. Q was referred to the wound care clinic for evaluation. A large amount of necrotic slough tissue was noted in the base of the wound (see Figure 1), along with a large amount of foul-smelling exudate. Sharp debridement was performed. To facilitate continued autolytic debridement, ALH was initiated with the NPWT dressings. A thin layer (the thickness of a dime) of ALH paste was applied to the surface of the wound before the NPWT foam dressing was applied. The dressing was changed three times per week.
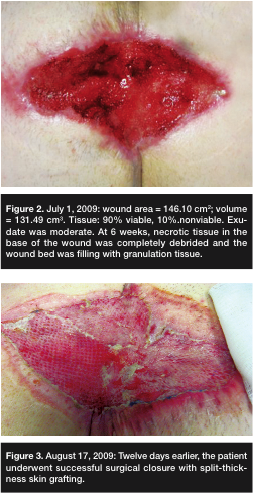
Over 10 weeks, the wound remained slough- and malodor-free, exudate decreased, and healthy granulation tissue was filling the wound; no infection was noted (see Figure 2). Once the wound was 100% filled with granulation tissue, a split-thickness skin graft was used to achieve complete closure (see Figure 3).
 The use of ALH paste used in combination with NPWT dressings was associated with rapid reduction in slough, malodor, and exudate. Granulation tissue formation improved. These outcomes enabled the application of a split-thickness skin graft for complete closure with no evidence of subsequent infection.
The use of ALH paste used in combination with NPWT dressings was associated with rapid reduction in slough, malodor, and exudate. Granulation tissue formation improved. These outcomes enabled the application of a split-thickness skin graft for complete closure with no evidence of subsequent infection.
Making Progress With Stalled Wounds is made possible through the support Derma Sciences, Inc., Princeton, NJ. The opinions and statements of the clinicians contained herein are specific to the respective authors and are not necessarily those of Derma Sciences, Inc., OWM, or HMP Communications.
This article was not subject to the Ostomy Wound Management peer-review process.
1. Andros G, Armstrong DG, Attinger CE et al. Consensus statement on negative pressure wound therapy (V.A.C. Therapy) for the management of diabetic foot wounds. Ostomy Wound Manage. 2006;52(6 suppl):1–32.
2. Hinman CD, Maibach HI. Effect of air exposure and occlusion on experimental human skin wounds. Nature. 1963;200:377–378.
3. Valenta AL. Using the vacuum dressing alternative for difficult wounds. Am J Nurs. 1994;94(4):44–45.
4. Aly R, Shirley C, Cunico B, Maibach HI. Effect of prolonged occlusion on the microbial flora, pH, carbon dioxide and transepidermal water loss on human skin. J Invest Dermatol. 1978;71(6):378–381.
5. Marples RR, Kligman AM, Growth of bacteria under adhesive tapes. Arch Dermatol. 1969;99(1):107–110.
6. Kumar P. Limited access dressing. Wounds. 2008;20(2):49–59.
7. Finegold SM. Pathogenic anaerobes. Arch Intern Med. 1982;142(11):1988–1992.
8. Zhai H, Maibach HI. Effect of occulsion and semi-occlusion on experimental skin wound healing: a reevaluation. Wounds. 2007;19(10):270–276.
9. Gethin G, Cowman S. Manuka honey vs. hydrogel — a prospective, open label, multicentre, randomised controlled trial to compare desloughing efficacy and healing outcomes in venous ulcers. J Clini Nurs. 2008;18(3):466–474.
10. White RJ, Molan P. A summary of published clinical research on honey in wound management. In: Cooper R, Molan P (eds). A Modern Wound Management Product. Aberdeen, UK: UK Publishers; 2005:130–142.
11. Cooper RA, Jenkins L. A comparison between medical grade honey and table honeys in relation to antimicrobial efficacy. Wounds. 2009;21(2):29–36.
12. Cooper RA, Jenkins L, Rowlands R. The influence of catalase on the antibacterial activity of honey. Poster presented at the Symposium on Advanced Wound Care. San Diego, CA. April 2008.
13. Blair SE, Cokcetin NN, Harry EJ, Carter DA, et al. The unusual antibacterial activity of medical-grade Leptospermum honey: antibacterial spectrum, resistance, and transcriptome analysis. Eur J Clin Microbiol Infect Dis. 2009;28:1199–1208.
14. Moore S. Squamous cell carcinoma of the head and neck: using active Leptospermum honey for wound management and odor control. Poster presented at the South Central Region Wound, Ostomy, Continence Nursing Conference. Edmond, OK. September 2008.




