



Epidermolysis Bullosa: When a Challenge Starts at Birth
Epidermolysis bullosa (EB) is a family of mechanobullous genetic disorders characterized by fragility of the skin in response to mechanical trauma. EB is caused by mutations in at least 14 genes that encode proteins of the basement membrane zone. If proteins are absent, adhesion between epidermis and dermal is diminished. The last classification was revised in 2014 and names 4 major categories defined by the level of cleavage at the dermal/epidermal junction (EB simplex [EBS], junctional EB [JEB], dystrophic EB [DEB], and Kindler syndrome) and many subcategories.1,2
Minimal, everyday friction causes blisters and erosions in EB. The extent and distribution depend on the subtype. Systemic complications, such as failure to thrive as well as laryngeal and esophageal strictures, can complicate the clinical course.
Dermal/epidermal junction EB simplex subtypes are inherited as both autosomal dominant (AD) and autosomal recessive (AR) conditions. EBS is a disorder of abnormally coded keratin proteins 5 and 14, necessary for keratin stability within basal epidermal cells. Dysfunction leads to mechanical weakness, breakdown, and blistering, even with minimal friction. EBS is divided into basal and suprabasal subtypes, 17 in total.1
Junctional EB has autosomal recessive inheritance and a defect at the lamina lucida level of the basement membrane. The mutation in JEB arises from components of hemidesmosomes, filaments providing integrity and anchorage across the basement membrane zone. Three (3) subtypes are known. The first subtype, generalized severe JEB, can be difficult to control; systemic complications such as respiratory failure due to laryngeal blisters, failure to thrive, and chronic sepsis lead to poor prognosis and survival past 2 years. Generalized intermediate JEB, the second subtype, has better survival rates, but many patients develop squamous cell carcinoma by a young age. The third subtype is JEB with pyloric stenosis present with feeding intolerance at a very young age, due to pyloric atresia. A defect in the integrin part of hemidesmosomes explains this variant, as integrin is important in gastrointestinal and genitourinary epithelium.1-3
Dystrophic EB has both AD and AR inheritance. A defect in protein collagen 7 is responsible for the separation at the sub-lamina densa part of the basement membrane zone. There are more than 15 subtypes, depending on the relative amount of collagen 7.1-3 This disease affects mucous membranes and leads to difficulty with feeding and bowel elimination as well as significant scarring with healing.
Kindler syndrome is an AR disorder caused by mutation in fermitin homolog 1 gene, leading to cleavage at various levels in the basement membrane zone. Clinical complications of periodontitis, malabsorption, diarrhea, and urethral strictures are common.1-3
NEONATAL PRESENTATION
Neonates with EB present with blisters (often on the extremities), areas of trauma, or areas of friction. Localized skin absence is variable. Granulation tissue can be exuberant, erosions can bleed, and blisters can develop with variable frequency. Most blisters in EBS and JEB will heal without scars, but with variable pigmentation. Special attention to oral erosions is warranted.
EBS can be worsened by hot and humid conditions because sweat exacerbates friction and promotes blistering. Although uncommon, airway, gastrointestinal, and genitourinary tract involvement may complicate initial presentation. Evaluation of blisters and erosions is at the helm of care for these children. Secondary concerns include temperature stability, electrolyte and fluid balance, feeding tolerance, sepsis prevention, and immediate access management.
Management. It is recommended that infants with EB be cared for in the neonatal intensive care unit by caregivers experienced in treating this disease. EB requires a multidisciplinary approach, often including a neonatologist, dermatologist, subspecialist such as gastroenterology, palliative care specialist, nurses, physical therapists experienced in care of such patients, and social work to support the family. The goals of care are the following: 1) accurate diagnosis of EB type; 2) existing wound healing and minimization of new blisters and erosions; 3) fluids, electrolytes, and temperature balance; 4) infection prevention; 5) pain control; 6) optimal nutrition; and 7) family support.
Diagnosis. DNA mutation analysis is very accurate, but many recommend this test to be directed toward a particular gene. The subtype can be diagnosed by immunofluorescence microscopy or transmission electron microscopy, and DNA mutation analysis can be used to confirm the diagnosis. It is the author’s practice to start with non–skin-invasive diagnosis (blood DNA mutation analysis), especially in preterm babies and proceed to biopsy only, if necessary, later in care. Transmission electron microscopy was considered a gold standard in the past, but immunofluorescence microscopy is now more widespread due to its availability, faster turnaround time, and an expanded panel of antibodies to proteins. If a blister is to be biopsied, it is important to induce a new blister because existing blisters may have reepithelialization evidence, leading to false diagnosis. Prenatal diagnosis is available with chorionic villus samples or amniocentesis to families with known mutations.
Daily care. A term neonate should be kept in an open crib, avoiding an enclosed isolette with extra humidity or temperature; preterm neonates should be weaned from humidity as transepidermal water loss stabilizes. Careful balance of temperature and humidity is important as blisters are more common in a humidified and heated environment, which may be necessary in preterm neonates or those with electrolytes derangements.
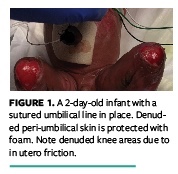
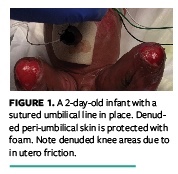
If intravenous nutrition and medications are necessary, placing an umbilical line initially may minimize skin punctures. Careful suturing of the line may allow minimal if any adhesive use (Figure 1). Further care may necessitate a prolonged central line; careful attention to securement dressings is necessary. The authors use a clear acrylate dressing, covered by a stretchable net. Use of silicon dressing remover is paramount in central line dressing change.
Nutrition, including maximum protein and daily vitamins, should be optimized. Careful introduction of oral feeding is observed, looking for signs of obstruction, gastroesophageal reflux, pain, or intolerance. Breast milk is the gold standard for neonates due to its anti-inflammatory and digestion-promoting effects. If extra calories are necessary, milk fortifiers can be given. Soft bottle nipples are recommended to minimize friction and blisters. If nasogastric tubes are placed, gentle handling and minimal friction should be ensured as internal mucosa can be injured. Feeding coordination can be challenging as solids are introduced. Feeding therapy and, if necessary, a gastrostomy tube may improve oral intake and provide adequate calories. Adequate weight gain and an effective feeding regimen are prerequisites to discharge, as well as close follow-up with a dermatology clinic. The author’s institution tries to arrange for home nurse visits as families are often overwhelmed initially.
Enrollment in an early intervention program is helpful, as motor skill development can be delayed due to pain, skin lesions, and anatomical deformity of lower and upper extremities. Many families have a difficult time taking care of ongoing wounds and feeding challenges. Referrals to a rehabilitation facility capable of EB-appropriate care are not unusual. The author knows of an excellent facility where a parent can stay with the child, or visit as often as possible, and learn the care slowly.
Skin care. The infant should be placed on a soft surface. The author uses soft, thin foam (Mepilex Lite; Mölnlycke) to pad the back areas and minimize friction. Bathing is delayed to minimize skin blistering; if an area is particularly oozy and thick exudate is observed, gentle irrigation can be done with warmed normal saline or hypochlorous acid solution. As babies get older, a once- or twice-a-week bath may help to soften areas of sloughed skin layers. The bath basin should be lined with blankets, and the patient held with a blanket against the skin to minimize friction. Neonates can be colonized with Staphylococcus aureus. Dilute bleach bath can help with decolonization.2-5
Dressings are applied and changed on an as-needed basis, and can be done every other day or so to minimize pain and unintentional injury. Diaper or tubular dressing edges can induce friction and blistering. This can be minimized by padding with foam, hydrofiber, or any other soft material.2-5
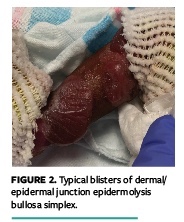
Blisters (Figure 2) and raw areas (Figure 1 and Figure 3) are often covered by nonadherent dressings such as petroleum jelly-impregnated gauze, atraumatic silicon contact layer, or a foam. These are often covered with an additional layer of petrolatum. For new and deep erosions, topical mupirocin can be applied (Figure 3). Lipido-colloidal layer (Urgotul; Urgo) is another dressing often used for these patients (Figure 4). Antimicrobial dialkylcarbamoyl chloride (DACC)–covered dressing with hydrogel (Cutimed Sorbact; BSN Medical) is another excellent option, especially if there is concern about infection (Figure 5).3,4 Polymeric membrane (PolyMem; Ferris) is very helpful, especially in wounds with exudate and around the digits. Stretchable silicon strips, petrolatum-impregnated strips, or hydrofiber can be used around the digits as well, minimizing the onset of webbing or mitten deformity from continuous trauma.3,4 Secondary dressings, such as foams, may be necessary for exudate absorption and padding; if not, soft rolled gauze, stretchable netting, or self-adhesive compression dressings can be used as retention dressings, eliminating adhesive tape.2-4 If tape is necessary, one that is silicon based, such as Mepitac (Mölnlycke), is recommended. Powder, such as cornstarch, is recommended by some to enhance blister drying and decrease friction. It should not be applied in areas of significant moisture, however, because it may turn to paste.
Generally, EB-related wounds treatment should be approached with the same sense as any wound: suppression of inflammation and promotion of tissue growth, prevention and treatment of infection, moisture balance, and edge (or intact skin) protection. Topical antimicrobial products safe for neonates should be used. Medical grade honey, DACC-coated dressings, and silver- or methylene blue/gentian violet–impregnated foams can be applied to colonized or infected wounds.3,5,6 Gentle hypochlorous acid6 and surfactant-based gel can be used to enhance cleansing and exudate removal while providing some antimicrobial protection. Hydrolyzed collagen gel or powder can be very helpful in deep erosions. Amniotic membrane–based products can enhance healing and minimize scarring.
Dressing application can be very painful; pain medication, oral dextrose drops, a pacifier, gentle swaddling, and a “one limb at a time” approach can help minimize discomfort. If cloths are used, soft material with seams to the outside are recommended. Parents need to become proficient in the daily care prior to discharge. Organizations such as debra of America (https://www.debra.org) can be excellent sources of information and support for families.
CASE STUDY
The images included in this article are of a neonate, born preterm at 31 weeks’ gestation, with unexpected skin findings (Figure 3). A gene study came back positive for mutation in keratin 14, consistent with EBS. Premature status and initial electrolyte derangements required the use of a humidified and heated isolette, which likely contributed to the slow healing of the existing blisters and the development of new ones. The patient required an umbilical line, followed by a percutaneous central catheter, which was challenging to place and secure. Patient discomfort and pain during dressing changes were not adequately covered with anti-inflammatory agents; stronger opioids were required, which was challenging because the respiratory drive was mildly affected at times.
The patient had feeding intolerance and aspirations, eventually leading to pneumonia, complete respiratory failure, pulmonary hypertension, and prolonged antibiotic use due to sepsis. Bloody stools from fissures and erosions were noted, and necrotizing enterocolitis developed. Securing an endotracheal tube and monitoring devices was essential yet caused many areas of denuded skin, despite meticulous use of dressing releaser, nonadhesive outer layers, and gentle care.
The critical state of the patient and the need for strong pain medications for hands-on care or dressing changes were challenges throughout treatment. Gabapentin (a medication successful with neuropathic pain/pruritus in older patients) was a useful adjunct to pain medications, allowing less opioid dependency. Palliative care, pain service, child life, social work, and many medical providers played integral roles in providing care. The patient was eventually transferred to a rehabilitation facility secondary to feeding difficulties, dependency on pain medications for hands-on care, and need for extensive family education.
Dr. Boyar is director of Neonatal Wound Services, Cohen Children’s Medical Center of New York, New Hyde Park, and assistant professor of Pediatrics, Zucker School of Medicine, Hofstra/Northwell, Hempstead, NY. All photos provided are with the consent of the patients’ parents. This article was not subject to the Wound Management & Prevention peer-review process.
1. Fine J-D, Eady RAJ, Bauer EA, et al. The classification of inherited epidermolysis bullosa (EB): report of the Third International Consensus Meeting on Diagnosis and Classification of EB. J Am Acad Dermatol. 2008:58(6):931–950. doi:10.1016/j.jaad.2008.02.004
2. Denyer J, Pillay E. Best practice guidelines for skin and wound care in epidermolysis bullosa. International Consensus. DEBRA, 2012.
3. Bruckner A, O’regan G. Inherited and acquired blistering diseases. In: Eichenfield L, Frieden I, Mathes E, Zaenglein A. Neonatal and Infant Dermatology. 3rd ed. Elsevier; 2015.
4. Lara-Corrales I, Arbuckle A, Zarinehbaf S, Pope E. Principles of wound care in patients with epidermolysis bullosa. Pediatr Dermatol. 2010;27(3):229–237. doi:10.1111/j.1525-1470.2010.01086.x
5. Bruckner-Tuderman L. Newer treatment modalities in epidermolysis bullosa. Indian Dermatol Online J. 2019;10(3):244¬–250. doi:10.4103/idoj.IDOJ_287_18
6. Elsass F. Adjunctive debridement with hypochlorous acid leads to a healing trajectory of complex wounds in children. Ostomy Wound Management. 2016;62(4):8–10.
7. Goldschneider KR, Good J, Harrop E, et al. Pain care for patients with epidermolysis bullosa: best care practice guidelines. BMC Med. 2014;12(178). doi:10.1186/s12916-014-0178-2

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}