




Ostomy Complications, Risk Factors, and Applied Nursing Care: A Retrospective, Descriptive Study





Abstract
PURPOSE: This study aimed to describe the frequency of colostomy and ileostomy complications and types of nursing interventions as well as to examine patient and ostomy variables associated with early and late complications. METHODS: The records of 572 patients who received ostomy care from a wound ostomy care (WOC) nurse between 2013 and 2017 were abstracted. Patient demographic and ostomy variables, early period (< 30 days after surgery) and late period (> 30 days after surgery) complications, as well as documented nursing interventions were retrieved. Percentages and rates, chi-square statistics, and logistic regression were used to analyze the data. RESULTS: The mean patient age was 59.1 years (standard deviation [SD], 13.86), and the majority of patients were male (302 patients; 52.8%), married (454; 79.4%), and had a temporary (438; 76.6%) end colostomy (253; 44.2%). One (1) or more complications developed in 323 patients (56.5%) in the early period and in 207 patients (36.2%) in the late period. The most common complications in the early period were peristomal irritant contact dermatitis (PICD) (181; 31.6%) and mucocutaneous separation (135; 23.6%). PICD was also the most common complication in the late period (149; 26%). The risk of PICD was significantly higher in patients with a body mass index > 24.9 kg/m2 (odds ratio [OR] = 1.547), who had an ileostomy (OR = 1.654), or a temporary ostomy (OR = 1.728). Variables associated with an increased risk of mucocutaneous separation included obstacles to ostomy care (OR = 2.222), having an end ostomy (OR = 2.171), and ostomy height < 10 mm (OR = 1.964). Complications were treated by the WOC nurse in 67.5% of patients, and the most common intervention was application of skin barrier powder and wipe layers. CONCLUSIONS: The rate of ostomy complications, especially PICD and mucocutaneous separation, in this study was high. Results confirm that patient and ostomy characteristics might significantly affect the risk of complications. The findings support the importance of outpatient follow-up by a WOC nurse. Explorative or randomized controlled studies are needed to identify optimal nursing strategies to decrease complication rates.
Introduction
Approximately 1 million people in the United States have fecal or urinary diversions, and approximately 100,000 people undergo ostomy surgery every year.1 Ostomy creation increases survival rates; however, postoperative complications do occur.2 Ostomy complications can be classified as early or late based on the time of postoperative onset. Early complications have been defined as occurring within 30 days after surgery; the most common early ostomy complications are peristomal irritant dermatitis, mucocutaneous separation, retraction, and necrosis.3–6 Late complications occur after this 30-day postoperative period and may include peristomal hernia, prolapse, stenosis, and granuloma.3,4
Despite recent advancements in ostomy surgery and care, the prevalence of ostomy complications varies between 10% and 70%.3,7–13 In an extensive, prospective study (n = 3970) conducted in the United Kingdom, 1 or more ostomy complications were reported in 1329 patients (34%) within 3 weeks after surgery.12 Persson et al7 followed patients in Sweden who had ostomies for 2 years and determined that 1 or more ostomy complications commonly developed 2 weeks after the patient was discharged. Retrospective studies conducted in Turkey reported that ostomy complications were observed in approximately one-third of patients with ostomy.3,9 Moreover, other studies showed that factors such as age, sex, body mass index (BMI), preoperative stoma site marking, type of ostomy, height of ostomy, emergency or elective procedure, comorbid disease, and surgical technique increase the risk of complications. However, it should be noted that in these results, actual risk factors may vary.3,6,11–14
Complications cause patients to feel anxious and present a challenge to maintain the pouching system, which in turn makes it difficult for them to adjust to the ostomy, prevents them from returning to daily life activities, and reduces their quality of life.15,16 A systematic review of 14 relevant papers demonstrated that ostomy-related problems influence patients’ quality of life negatively.17 Complications can also lead to increased expenses caused by the requirement to frequently change the pouching system and increased use of other ostomy-related products.18,19 A qualitative analysis by Sun et al16 showed that a patient with an ostomy experiences multiple challenges regarding postoperative equipment application and stoma care procedures.
The key element to managing an ostomy complication is to prevent it. Wound, ostomy, and continence (WOC) nurses contribute significantly to the care of patients by preventing complications.4,20 Preoperative stoma site marking by a WOC nurse reduces the complication rate, and preoperative counseling facilitates the postoperative adjustment to ostomy for the patient.4 In addition, postoperative education and follow-up are essential to provide optimal outcomes. Ideally, the patient should be able to manage all aspects of ostomy care independently prior to hospital discharge.20,21 Skills taught by WOC nurses promote self-care and make adapting to new circumstances easier for patients. A case–control study (n = 50) by Danielsen and Rosenberg22 reported that patients with an ostomy who attended a postoperative ostomy education program improved their health-related quality of life compared with those patients who do not attend the program. Thus, WOC nurses are important in providing postoperative education to these patients. In addition, care by a WOC nurse can help patients maintain the seal of a pouching system for a predictable period without leakage, thus protecting the peristomal skin.20,21,23 When complications develop, management by a WOC nurse is essential for the patient’s recovery, which then increases the health-related quality of life.12 Harris and Shannon24 determined that WOC nurses are important leaders in patient care and reduce patients’ health care costs.
The identification and management of ostomy complications are an international priority. Despite the reported incidence of ostomy complications, evidence-based guidance for the treatment and care of these complications is very limited.25 This retrospective, cohort study aimed to determine the frequency of ostomy complications, their associated factors, and the applied nursing care. The study questions were as follows: 1) What are the early and late period complication rates and the factors affecting these complications? 2) What does nursing care for patients with ostomy complications entail?
Methods
This retrospective, cohort study was conducted in the stoma therapy unit of Dokuz Eylül University Hospital, Turkey, between July 2018 and November 2018. Data were extracted from the hospital’s patient records (2013–2017) created during hospitalization and outpatient follow-up. The paper-based patient records were completed by 3 nurses who were WOC nursing certified. WOC nurse visits, assessments, and interventions were recorded.
A total of 1004 hospital patient records were retrieved and screened. Inclusion criteria were patients who had undergone surgery to create an ileostomy or a colostomy, who had completed follow-up appointments after discharge, and whose records were complete. The records of 572 ostomy patients met these criteria.
Sample size. The sample size was determined using the G-Power 3.0.10 statistical power analysis software. For the post power analysis, results of the logistic regression analyses were used to calculate the power. A total power of 99% was revealed.
Study variables and assessment. All variables taken into account in this study were selected based on the literature3,6,7,9,11,14,25 and patient records at the authors’ institution. The study variables were abstracted and recorded on 2 specially designed forms developed for this study by the researchers. The first form, The Demographic and Ostomy-Related Characteristics Forms, included age, sex, marital status, employment status, preoperative neoadjuvant therapy, educational level, comorbid disease (hypertension, heart diseases, diabetes mellitus, rheumatism, chronic respiratory disease), BMI, elective or emergency surgery, preoperative education, preoperative stoma site marking, reason for ostomy, type of ostomy (end/loop colostomy, end/loop ileostomy), ostomy location, permanent or temporary ostomy, ostomy configuration (height and shape), ostomy moisture (moist or dry), and obstacles to ostomy care and education (ie, visual impairment, age-related poor dexterity, cognitive impairment, hearing loss, tremor due to Parkinson disease, dementia, immobility, hemiplegia/plegia, and joint disorder caused by rheumatoid arthritis). Obstacles to ostomy care and education had been assessed by the WOC nurse during the first encounter and follow-up of the patient. BMI at the time of postoperative hospitalization was documented. The stoma site was marked preoperatively according to the recommendations from the Wound Ostomy Continence Nurses Society26 and was recorded on the patient form by the WOC nurses. The height of the ostomy was measured at the time of postoperative hospitalization; height was described as the distance between the ostomy lumen (top of the stoma) and the skin.
The second form, the Complication Diagnosis and Nursing Care Evaluation Form, consisted of items to evaluate early period ostomy complications, which were defined as those that occurred within 30 days of surgery, and late period ostomy complications, which were defined as those that developed > 30 days after surgery. Ostomy complications were evaluated using the definitions developed by Beitz and Colwell.25 This taxonomy generated a strong level of content validation (content validity index, 0.96–0.97) among a group of expert WOC nurse raters. Ostomy complications utilized in this study included peristomal irritant contact dermatitis (PICD) (damage resulting from skin exposure to fecal or urinary drainage or chemical preparations), mucocutaneous separation (the detachment of stomal tissue from the surrounding peristomal skin), peristomal suture granuloma (excessive tissue occurring at skin/stoma base in areas of retained or reactive suture material), stomal retraction (the disappearance of normal stomal protrusion in line with or below skin level), stomal necrosis (death of stomal tissue resulting from impaired blood flow), peristomal hernia (a defect in abdominal fascia that allows the intestine to bulge into the peristomal area), stomal prolapse (the telescoping of the intestine through the stoma), stomal fistula (an abnormal communication between the stoma and surrounding tissue), stomal stenosis (impairment of effluent drainage due to narrowing or contracting of the stoma tissue at skin or fascial level), and maceration (skin softening and breakdown caused by prolonged exposure to moisture; affected skin was soft, pale, and wrinkled).
Nursing interventions to treat the complications, ostomy education/teaching frequency, and postdischarge patient follow-up frequency in the stoma therapy or general surgery department were also abstracted. The actual duration of patient ostomy education was not recorded and varied according to the needs of the patient. The abstracted nursing interventions were grouped by the researcher.
Data abstraction and analysis. Study variables were abstracted and recorded using a paper-and-pencil instrument by the researcher. Completing the forms took approximately 20 to 25 minutes. Data collection procedures were conceived to protect participant confidentiality. All data were checked carefully, immediately after collection, to avoid any inaccurate information. Data were entered directly into the SPSS 24.0 version software. Descriptive statistics were used to summarize the demographic and ostomy characteristics of the patients. Student t-test and chi-square test were performed to assess the relationship between demographics and complications. Logistic regression was used to assess whether any independent variables predicted the development of complications. The demographic variables included in the model were determined based on the literature3,8,10,12,13 by considering univariate analyses. The assumption that independent and dependent variables were linearly related to the logit was checked and met.
Ethical considerations. Written permission to conduct the study was obtained from Dokuz Eylül University Hospital and the Dokuz Eylül Non-Invasive Studies Ethics Committee (Date: 2018/26-07, Decision no: 2018/19-36).
Results
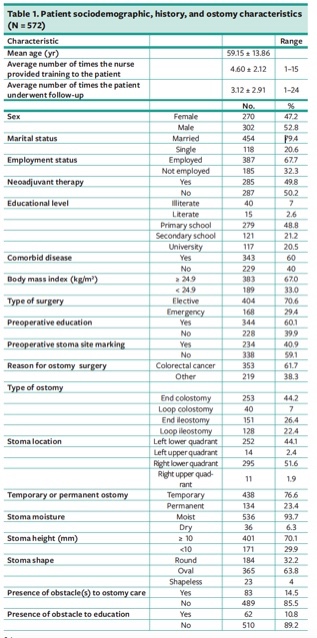
Of the total sample (572 patients), 302 (52.8%) were male, and 454 (79.4%) were married. Mean patient age was 59.15 ± 13.86 years and approximately half (279; 48.8%) were primary school graduates. Most (383; 67%) had a BMI ≥ 24.9 kg/m2. The majority of patients (404; 70.6%) had elective surgery, and 344 (60.1%) received preoperative education. Colorectal cancer (353; 61.7%) was the predominant diagnosis. The type of ostomy included end colostomy (253; 44.2%), loop colostomy (40; 7%), end ileostomy (151; 26.4%), and loop ileostomy (128; 22.4%). A little less than half (234; 40.9%) had their stoma site marked preoperatively; 438 (76.6%) had a temporary ostomy, 295 (51.6%) had an ostomy in the right lower quadrant, and 171 (29.9%) had an ostomy height of < 10 mm. Most patients (489; 85.5%) did not have any obstacles during ostomy care. The average number of times the nurse provided training to the patient and the average number of times the patient underwent follow-up were 4.60 ± 2.12 and 3.12 ± 2.91, respectively. Other patient demographic and ostomy characteristics are presented in Table 1.
{kind=link}
In the early period, 1 or more complications developed in 323 patients (56.5%). The most common complication was PICD (181; 31.6%), which occurred mainly within the second or third week after ostomy creation. The second most common complication was mucocutaneous separation (135; 23.6%), which occurred mainly in the first or second week after ostomy creation. Other less common complications were peristomal suture granuloma (29; 5.1%), stomal retraction (19; 3.3%), stomal necrosis (15; 2.6%), bleeding (15; 2.6%), maceration (8; 1.4%), and stomal fistula (10; 1.7%) (Table 2).
One or more complications developed in the late period in 207 (36.2%) patients. The most common late complication was PICD (149; 26%), which occurred mainly in the second month after ostomy creation. Other complications were peristomal hernia (54; 9.4%), peristomal suture granuloma (24; 4.2%), stomal prolapse (24; 4.2%), fistula (16; 2.8%), stenosis (7; 1.2%), and retraction (6; 1%) (Table 3).
PICD developed most often in patients with loop ileostomy in the early period (P = .001), whereas the complication incidence rate in the late period was not affected by the type of ostomy (P = .608). Mucocutaneous separation developed less frequently in patients with loop ostomy compared to those with end ostomy, and the difference was statistically significant (P = .000). Peristomal hernia was determined to develop most commonly in patients with end colostomy, and the difference was statistically significant (P = .007) (Table 4).
Multiple logistic regression analyses of the factors associated with a higher incidence of PICD, mucocutaneous separation, and peristomal hernias are summarized in Table 5. The incidence of PICD was significantly higher among patients with a BMI > 24.9 kg/m2 (odds ratio [OR] = 1.547; 95% confidence interval [CI] = 1.074–2.227), temporary ostomy (OR = 1.728; 95% CI = 1.127–2.648), and ileostomy (OR = 1.654; 95% CI = 1.157–2.365). The odds of mucocutaneous separation were greater in patients with obstacles to ostomy care (OR = 2.222; 95% CI = 1.294–3.816), end ostomy (OR = 2.171; 95% CI = 1.280–3.683), and ostomy height < 10 mm (OR = 1.964; 95% CI = 1.261–3.060). The OR of peristomal hernia development was significantly higher in patients aged > 65 years (OR = 2.104; 95% CI = 1.168–3.791) and in those with a left quadrant ostomy (OR = 2.640; 95% CI = 1.355–5.143).
Of the total sample (572 patients), 386 (67.5%) received care for complications from a WOC nurse. Among the 181 patients with PICD, skin barrier powder and wipe layers/sprays were applied in 173 patients (95.6%) and absorbent materials were applied in 43 patients (23.8%). New ostomy products (such as convex flange, change of flange or paste, more flexible products, elastic barrier strips, and adhesive remover wiper/spray) were recommended to 83 patients (45.9%) who had PICD, while the use of an ostomy belt was recommended to only 22 patients (12.2%). Skin barrier powder was applied to 126 patients (93.3%) with mucocutaneous separation (n = 135), whereas the separation areas of 78 patients (57.8%) were filled with hydrofiber; it was recommended to 44 patients (32.6%) to use new ostomy products. Skin barrier powder was applied to 43 patients (81.1%) with peristomal suture granuloma, and silver nitrate was applied to 38 patients (71.7%). Hernia belt use was recommended to all patients with peristomal hernia. Cold compress application was recommended to all patients with prolapse. A majority of participants (20; 80%) who experienced retraction were advised to replace the product with convex flange (Table 6).
Discussion
The high rate of ostomy complications is a challenge.11,15 The current study found that 56.5% of patients had at least 1 complication in the early period, whereas 36.2% of patients had at least 1 complication > 30 days after surgery, which is similar to results of previously published retrospective8 and prospective7,10,11,27 studies conducted in other parts of the world. Compared to the retrospective studies conducted in Turkey, while the complication incidence rate in the late period was similar to the rate determined by Baykara et al,9 the complication rate in this study during the early period was higher than the rate reported by Koc et al.3 However, a clear and direct comparison cannot be made as a result of the many different definitions of ostomy-related complications used in the literature. The results of studies conducted on ostomy complications may vary due to differences in inclusion criteria and methodology, the definitions of the complications not being expressed clearly, and differences in surgical techniques.
In this study, the most common complication in both the early and late periods was PICD, which was observed most often in patients with an ileostomy. These results are similar to the literature.7,9,10,12,14,15 Other important results are that PICD most commonly developed in the second or third week in the early period and that the rate of PICD decreased over time. Similarly, a prospective study (n = 180) conducted by Persson et al7 determined that peristomal skin problems developed most commonly in patients with ileostomy 2 weeks after surgery. The decrease in the frequency of PICD may be explained by the ostomy reaching its actual size after edema decreases, the correct cutting of the flange, patients adapting to ostomy care, and the closure of the temporary ostomy. Considering the results of this study and those in the literature, patient follow-up after discharge is important.
In this study, mucocutaneous separation was the second most common complication. It occurred in 23.6% of patients and most commonly within the first 2 weeks postoperatively. This finding is similar to results of a retrospective study conducted in Turkey9 and prospective studies conducted in other parts of the world.10,12 A prospective study conducted by Cottam et al12 found that mucocutaneous separation occurred in 24% of patients within 3 weeks after ostomy surgery. Lindholm et al10 conducted a prospective study in patients with ostomy who underwent emergency surgery and reported that mucocutaneous separation developed within the first 2 weeks after ostomy creation. Other prospective7 and retrospective8 studies have found lower rates of mucocutaneous separation. Thus, considering other studies in the literature, mucocutaneous separation varies between 3.7% and 24%.3,8,9,12
In the current study, the rate of peristomal suture granuloma in the early (5.1%) and late (4.2%) period was low and similar to that reported in the literature.7,8 In this study, granuloma developed more commonly between the first and second month after surgery. A prospective study of patients (n = 180) who underwent elective ostomy surgery reported that granuloma occurred between the third and sixth month,7 whereas results of a prospective study among patients (n = 144) who underwent emergency surgery showed that granuloma developed in 12th month postoperatively.10 The occurrence of granuloma in the early period could be the result of poor ostomy care skills and the incorrect cutting of the flange. Because granuloma causes bleeding and pain, it may increase anxiety in patients, making it difficult for them to change the pouch system.10
The rate of retraction in the early (3.3%) and late (1%) periods in this study was found to be similar to previously published prospective11 and retrospective3 studies. However, other retrospective8 and prospective6,12 studies have shown retraction rates of 7.4% to 40.1%. Shellito28 determined that retraction is usually caused by previous stomal necrosis or tension on the bowel when ostomy creation was performed.
In this study, the rate of peristomal hernias was 9.4%, which was lower than the rates reported by Arumugam et al27 and Robertson et al.29 Arumugam et al27 reported that among 97 patients, parastomal hernia developed in 12 patients. Robertson et al29 reported that the proportion of patients who had parastomal hernias increased with time (from 0 to 40% in the colostomy and 0 to 22% in the ileostomy groups). However, in Sung et al’s retrospective work (N = 1170),8 the rate (5.8%) was lower than in this study. In this study, peristomal hernias occurred more commonly in patients with end ostomy. This result is in agreement with a study conducted by Persson et al.7
Several variables affect the development rate of peristomal hernias, including age, ostomy creation outside of the rectus abdominis muscle, suboptimal operative techniques, and the fascia tissue being excessively damaged.8,26,28,30 Based on an advanced analysis, the current study determined that age > than 65 years and left quadrant ostomy affected the development of hernia. Peristomal hernias present multiple challenges for patients including cosmetic issues, local discomfort, pain, the sensation of a mass in the abdomen, and flange application problems.8,10
In the present study, having a BMI > 24.9 kg/m2, an ileostomy, or a temporary ostomy increased the rate of PICD. The literature relevant to PICD reports that the output of more liquid stool may damage skin integrity on various levels.14,15,31,32 Other research, similar to this study, showed that obesity was related to a higher frequency of peristomal complications.8,12,27 Based on the literature and the results of this study, it can be concluded that weight control may be an important factor in preventing PICD in patients with an ostomy.
End ostomy, obstacles to ostomy care, and ostomy height < 10 mm influenced the likelihood of mucocutaneous separation in this study. The result that end ostomy increases the risk of the development of mucocutaneous separation was in accordance with the results of previous studies.9,10,12 Similarly, Lindholm et al10 reported that mucocutaneous separation developed more commonly in patients with an end colostomy. Cottam et al12 concluded that the likelihood of stoma complications can be predicted based on ostomy height.12 Parmar et al6 reported that the ostomy was more “problematic” in patients with short ostomy length. In that study,6 a problematic stoma was “one which needs one or more accessories to keep the patient clean and dry for a minimal period of 24 h[ours].”
In the current study, 67.5% of patients received care for the complications they encountered and were taught how to prevent future complications. The application of powder and barrier sprays to areas with rashes and the use of ostomy equipment are suggested in managing patients with PICD.23,32–35 In this study, powder and barrier sprays were used in 95.6% of patients with PICD. Colwell et al34 stated that WOC nurses most commonly use powder and barrier wipe layers (81.4%) for patients with PICD. A cross-sectional descriptive study was conducted by Beitz and Colwell25 with WOC nurses (n = 281) to evaluate which optimal interventions WOC nurses used the most for complications. They found that nurses used powder and barrier sprays more commonly for patients with peristomal irritant dermatitis after determining the etiology of the complication by evaluating the peristomal skin. In the same study, WOC nurses stated that they applied silver nitrate to remove excess tissue. Silver nitrate was also applied to the majority of patients with peristomal suture granuloma (71.7%) in the current study.
Optimal management of mucocutaneous separation, including filling the site with absorbent materials, paste, or powder depending on its extent, is very important to prevent additional complications until the area has healed.20 In this study, powder and barrier sprays were used on 93.3% of patients with mucocutaneous separation, whereas absorbent materials were used on 57.8%.
Patients with a peristomal hernia are advised to avoid heavy lifting and wear supportive clothing/hernia belts. Surgery is performed only if the bowel is obstructed.20,25,35,36 In this, and previous studies, patients with peristomal hernias were advised to use hernia belts and flexible products.25,33 In cases in which prolapse, observed in the late period, decreases patients’ quality of life or when the ostomy is under too much tension, surgical treatment is advised. In other cases, interventions such as applying a cool compress to the ostomy to reduce ostomy size and choosing an appropriate pouch system were found to be similar to those previously reported.25,33
Previous studies have recommended the use of convex flanges and belts to patients with retraction.7,20,34 Colwell et al34 stated that 46.8% of WOC and enterostomal therapy nurses reported that 26% to 50% of their patients required convexity. In the current study, new products were also recommended.
All patients with an ostomy deserve to be cared for by health professionals who possess sufficient knowledge to assess and recommend optimal ostomy care strategies and help prevent complications.23 Nursing interventions in this study were congruent with those described in the literature.
Limitations
The first limitation of this study is related to the nature of descriptive and retrospective studies. It covered only a certain period, did not include patients with incomplete records, and relied on the accuracy of existing documentation. Also, patient follow-up data were limited in some cases. As a result, the actual complication rates may be lower or higher than reported.
Conclusion
This was a retrospective, cohort study to evaluate the frequency of ostomy complications and their associated factors, as well as to describe applied nursing care in a group of patients with ostomy. PICD and mucocutaneous separation were the most common complications in the early period, whereas PICD and peristomal hernias were the most commonly documented late period complications. Ostomy type was found to be the most important variable in the development of complications. Ileostomy, BMI > 24.9 kg/m2, and temporary ostomy increased the risk of the development of PICD. End ostomy, obstacles to ostomy care, and an ostomy height < 10 mm were risk factors for the development of mucocutaneous separation; age older than 65 years and left quadrant ostomy increased the risk of peristomal hernia development. Application of skin barrier powder and wipe layers to the affected skin was the most common treatment for PICD. These findings support the importance of patient follow-up in the early and late period by a WOC nurse. Explorative or randomized controlled studies are needed to identify possible nursing strategies to decrease the frequency of stoma complications.
Affiliations
Ms. Ayik is a research assistant, Dokuz Eylül University, Izmir, Turkey, and a PhD candidate at Dokuz Eylül University Graduate School of Health Sciences, Izmir, Turkey; Dr. Özden is an associate professor, Dokuz Eylül University, Izmir, Turkey; and Ms. Cenan is an enterostomal therapy nurse, Dokuz Eylül University Research and Application Hospital, Izmir, Turkey. Address all correspondence to: Cahide Ayik, Nursing Faculty, Dokuz Eylül University, Balcova, Izmir, Turkey; fax: +90 232 412 47 89; tel: +90 232 412 6967; email: cahideayk@gmail.com
References
1. United Ostomy Associations of America. Welcome to UOAA. https://www.ostomy.org/our-mission-history/. Published 2015. Accessed June 3, 2018.
2. Nichols T, Goldstine J, Inglese G. A multinational evaluation assessing the relationship between peristomal skin health and health utility. Br J Nurs. 2019;28(5):S14–S19. doi:10.12968/bjon.2019.28.5.S14
3. Koc U, Karaman K, Gomceli I, et al. A retrospective analysis of factors affecting early stoma complications. Ostomy Wound Manag. 2017;63(1):28–32.
4. Hsu MY, Lin JP, Hsu HH, Lai HL, Wu YL. Preoperative stoma site marking decreases stoma and peristomal complications: a meta-analysis. J Wound Ostomy Continence Nurs. 2020;47(3):249–256. doi:10.1097/WON.0000000000000634
5. Ratliff CR. Early peristomal skin complications reported by WOC nurses. J Wound Ostomy Continence Nurs. 2010;37(5):505–510. doi:10.1097/WON.0b013e3181edac57
6. Parmar KL, Zammit M, Smith A, Kenyon D, Lees NP. A prospective audit of early stoma complications in colorectal cancer treatment throughout the Greater Manchester and Cheshire colorectal cancer network. Colorectal Dis. 2011;13(8):935–938. doi:10.1111/j.1463-1318.2010.02325.x
7. Persson E, Berndtsson I, Carlsson E, Hallén AM, Lindholm E. Stoma-related complications and stoma size - a 2-year follow up. Colorectal Dis. 2010;12(10):971–976. doi:10.1111/j.1463-1318.2009.01941.x
8. Sung YH, Kwon I, Jo S, Park S. Factors affecting ostomy-related complications in Korea. J Wound Ostomy Continence Nurs. 2010;37(2):166–172. doi:10.1097/WON.0b013e3181cf7b76
9. Baykara ZG, Demir SG, Karadag A, et al. A multicenter, retrospective study to evaluate the effect of preoperative stoma site marking on stomal and peristomal complications. Ostomy Wound Manag. 2014;60(5):16–26.
10. Lindholm E, Persson E, Carlsson E, Hallén AM, Fingren J, Berndtsson I. Ostomy-related complications after emergent abdominal surgery. J Wound Ostomy Continence Nurs. 2013;40(6):603–610. doi:10.1097/won.0b013e3182a9a7d9
11. Salvadalena GD. The incidence of stoma and peristomal complications during the first 3 months after ostomy creation. J Wound Ostomy Continence Nurs. 2013;40(4):400–406. doi:10.1097/WON.0b013e318295a12b
12. Cottam J, Richards K, Hasted A, Blackman A. Results of a nationwide prospective audit of stoma complications within 3 weeks of surgery. Colorectal Dis. 2007;9(9):834–838. doi:10.1111/j.1463-1318.2007.01213.x
13. Carlsson E, Fingren J, Hallén AM, Petersén C, Lindholm E. The prevalence of ostomy-related complications 1 year after ostomy surgery: a prospective, descriptive, clinical study. Ostomy Wound Manag. 2016;62(10):34–48.
14. Nybæk H, Bang Knudsen D, Nørgaard Laursen T, Karlsmark T, Jemec GB. Skin problems in ostomy patients: a case-control study of risk factors. Acta Derm Venereol. 2009;89(1):64–67. doi:10.2340/00015555-0536
15. Pittman J, Rawl SM, Schmidt CM, et al. Demographic and clinical factors related to ostomy complications and quality of life in Veterans with an ostomy. J Wound Ostomy Continence Nurs. 2008;35(5):493–503. doi:10.1097/01.won.0000335961.68113.cb
16. Sun V, Bojorquez O, Grant M, Wendel CS, Weinstein R, Krouse RS. Cancer survivors’ challenges with ostomy appliances and self-management: a qualitative analysis. Support Care Cancer. 2020;28(4):1551–1554. doi:10.1007/s00520-019-05156-7
17. Vonk-Klaassen SM, de Vocht HM, den Ouden MEM, Eddes EH, Schuurmans MJ. Ostomy-related problems and their impact on quality of life of colorectal cancer ostomates : a systematic review. Qual Life Res. 2016;25(1):125–133. doi:10.1007/s11136-015-1050-3
18. Neil N, Inglese G, Manson A, Townshend A. A cost-utility model of care for peristomal skin complications. J Wound Ostomy Continence Nurs. 2016;43(1):62–68. doi:10.1097/WON.0000000000000194
19. Nagano M, Ogata Y, Ikeda M, Tsukada K, Tokunaga K, Iida S. Peristomal moisture-associated skin damage and independence in pouching system changes in persons with new fecal ostomies. J Wound Ostomy Continence Nurs. 2019;46(2):137–142. doi:10.1097/WON.0000000000000491
20. Goldberg M, Colwell J, Burns S, et al. WOCN Society Clinical Guideline: management of the adult patient with a fecal or urinary ostomy —An executive summary. J Wound Ostomy Continence Nurs. 2018;45(1):50–58. doi:10.1097/WON.0000000000000396
21. Prinz A, Colwell JC, Cross HH, Mantel J, Perkins J, Walker CA. Discharge planning for a patient with a new ostomy: best practice for clinicians. J Wound Ostomy Continence Nurs. 2015;42(1):79–82. doi:10.1097/WON.0000000000000094
22. Danielsen AK, Rosenberg J. Health related quality of life may increase when patients with a stoma attend patient education a case-control study. PLoS One. 2014;9(3):e90354. doi:10.1371/journal.pone.0090354
23. Stelton S, Zulkowski K, Ayello EA. Practice implications for peristomal skin assessment and care from the 2014 world council of enterostomal therapists international ostomy guideline. Adv Skin Wound Care. 2015;28(6):275–284. doi:10.1097/01.ASW.0000465374.42350.0f
24. Harris C, Shannon R. An innovative enterostomal therapy nurse model of community wound care delivery: a retrospective cost-effectiveness analysis. J Wound Ostomy Continence Nurs. 2008;35(2):169–183. doi:10.1097/01.WON.0000313639.37247.c0
25. Beitz JM, Colwell JC. Stomal and peristomal complications: Prioritizing management approaches in adults. J Wound Ostomy Continence Nurs. 2014;41(5):445–454. doi:10.1097/WON.0000000000000052
26. Salvadalena G, Hendren S, McKenna L, et al. WOCN Society and ASCRS Position statement on preoperative stoma site marking for patients undergoing colostomy or ileostomy surgery. J Wound Ostomy Continence Nurs. 2015;42(3):249–252. doi:10.1097/WON.0000000000000119
27. Arumugam PJ, Bevan L, Macdonald L, et al. A prospective audit of stomas-analysis of risk factors and complications and their management. Colorectal Dis. 2003;5(1):49–52. doi:10.1046/j.1463-1318.2003.00403.x
28. Shellito PC. Complications of abdominal stoma surgery. Dis Colon Rectum. 1998;41(12):1562–1572. doi:10.1007/BF02237308
29. Robertson I, Leung E, Hughes D, et al. Prospective analysis of stoma-related complications. Colorectal Dis. 2005;7(3):279–285. doi:10.1111/j.1463-1318.2005.00785.x
30. Antoniou SA, Agresta F, Garcia Alamino JM, et al. European Hernia Society guidelines on prevention and treatment of parastomal hernias. Hernia. 2018;22(1):183–198. doi:10.1007/s10029-017-1697-5
31. Woo KY, Sibbald RG, Ayello EA, Coutts PM, Garde DE. Peristomal skin complications and management. Adv Skin Wound Care. 2009;22(11):533–534. doi:10.1097/01.asw.0000305498.23391.22
32. Burch J. Stoma care: an update on current guidelines for community nurses. Br J Community Nurs. 2017;22(4):162–166. doi:10.12968/bjcn.2017.22.4.162
33. Beitz JM, Colwell JC. Management approaches to stomal and peristomal complications: a narrative descriptive study. J Wound Ostomy Continence Nurs. 2016;43(3):263–268. doi:10.1097/WON.0000000000000215
34. Colwell JC, McNichol L, Boarin J. North America wound, ostomy, and continence and enterostomal therapy nurses current ostomy care practice related to peristomal skin issues. J Wound Ostomy Continence Nurs. 2017;44 (3):257–261. doi:10.1097/WON.0000000000000324
35. O’Flynn SK. Peristomal skin damage: assessment, prevention and treatment. Br J Nurs. 2019;28(5):S6–S12. doi:10.12968/bjon.2019.28.5.S6
36. Stelton S. CE: Stoma and peristomal skin care: a clinical review. Am J Nurs. 2019;119(6):38–45. doi:10.1097/01.NAJ.0000559781.86311.64
