



The Effect of a Wound Care Solution Containing Polyhexanide and Betaine on Bacterial Counts: Results of an in vitro Study
Abstract
Polyhexanide and betaine topical solution is used in the management of infected wounds as a cleaning agent. An in vitro study was conducted to examine the antimicrobial effects of a solution containing 0.1% of the antimicrobial agent polyhexanide and 0.1% of the surfactant betaine.
Three batches of each product were tested, and culture results of 13 micro-organisms were evaluated after 7, 14, and 28 days using USP <51> methodology. Growth reduction was identical at each day following exposure to the solution in all micro-organisms except Aspergillus brasiliensis. A range of 5.3-log to 5.8-log reduction was seen for the following micro-organisms: Staphylococcus epidermidis, Pseudomonas aeruginosa, Serratia marcescens, Candida albicans, S. aureus, vancomycin-resistant Enterococcus faecalis, Proteus mirabilis, Escherichia coli, methicillin-resistant S. aureus, Acinetobacter baumannii, Enterobacter cloacae, and E. faecalis. For A. brasiliensis, reductions were 2.1-log, 2.3-log and 2.8-log at 7, 14, and 28 days, respectively. The results of this study indicate a 4+ log inhibition of activity in 12 of 13 micro-organisms exposed to the solution. Research to elucidate the potential clinical effects of these observations is needed.
Potential Conflicts of Interest: Mr. Minnich, Dr. Wilkins, and Dr. Unverdorben disclose they are employees, received a consulting fee or honorarium, and/or received payment for writing or reviewing the manuscript from B Braun Medical Inc, Allentown, PA.
Introduction
Wound healing potential is determined by a variety of factors, including underlying disease, susceptibility to infection, and the patient’s overall health.1 Chronic wounds develop when the normal wound healing process is delayed,2 have been estimated to affect >1% of the general population, and generate healthcare costs of up to $15,000 for each episode of care.3,4 Contamination by large numbers (>105 bacterial cells/g of tissue5,6) of bacteria from the skin and the surrounding environment can create a pro-inflammatory environment7 that enhances the risk of infection. Thus, it is possible that a reduction in bacterial bioburden by creating conditions in the wound that favor tissue viability and are unfavorable to micro-organism growth may reduce the impairment of and delay in wound healing.
Although the use of topical antimicrobial agents is considered by some authors8 to be essential in wound care, their use remains controversial even though wound infection is associated with increased morbidity and mortality9 and higher bioburden is associated with infection and delayed healing.5,6 In order to be considered antimicrobially effective, a topical wound care product must demonstrate a significant reduction of microbial growth across a wide range of clinically relevant micro-organisms, including anaerobic and aerobic bacteria, antibiotic-resistant bacteria, mold, and yeasts. Some authors10 consider a 3-log reduction of micro-organisms in time-kill in vitro studies as significant.
In animal studies and clinical practice,11-14 use of a solution containing 0.1% of the antimicrobial polyhexanide and 0.1% of the surfactant betaine has been associated with evidence suggestive of improved wound healing. Polyhexanide is a polymeric biguanide with antimicrobial activities first described in 1956.15 Its antimicrobial activity is based on the adsorption of the drug to phosphatidylglycerol and other negatively charged phospholipids of the cellular membrane, causing changes in the physical properties and disorganization of the cellular membrane.16,17 The negative charge of the outer surface of the cellular membrane is a universal characteristic of bacteria, allowing the drug to act on both Gram-positive and Gram-negative bacteria.18 Other binding sites of the drug include lipopolysaccharides, teichoic acids, and proteoglycans.18 These nonspecific mechanisms of action translate into biocidal effects against other organisms such as yeast and fungi without damage to cells involved in mammalian healing.18
Undecylenamidopropyl betaine is a mild surfactant developed for use in personal care products. It is a derivative of undecylenic acid, a natural fungicide; it is not easily metabolized by micro-organisms and is able to act as an antimicrobial agent.19 Undecylenamidopropyl betaine has been shown in vitro to have the potential to decrease fibroblast cytotoxicity up to 50% and enhance bactericidal effectiveness against Pseudomonas aeruginosa when compared to polyhexanide alone.20 Prontosan® Wound Solution (B Braun Medical Inc., Allentown, PA) contains polyhexanide and undecylenamidopropyl betaine with sodium hydroxide to control pH. The product is sterile following aseptic manufacturing and remains sterile until the product is first opened.  The purpose of this in vitro study was to investigate the antimicrobial effectiveness of polyhexanide 0.1% and betaine 0.1% solution.
The purpose of this in vitro study was to investigate the antimicrobial effectiveness of polyhexanide 0.1% and betaine 0.1% solution.
Materials and Methods
The study was conducted according to the internationally recognized United States Pharmacopeia (USP) <51> Antimicrobial Effectiveness Test recommendations21 and included micro-organisms commonly found in the wound bed: Staphylococcus aureus, ATCC No. 6538; P. aeruginosa, ATCC No. 9027; Escherichia coli, ATCC No. 8739; Candida albicans, ATCC No. 10231; Aspergillus brasiliensis (formerly A. niger), ATCC No. 16404; methicillin-resistant S. aureus (MRSA), ATCC No. 33591; vancomycin-resistant Enterococcus faecalis (VRE), ATCC No. 51575; Serratia marcescens, ATCC No. 13880; Acinetobacter baumannii, ATCC No. 15149; Proteus mirabilis, ATCC No. 12453; S. epidermidis, ATCC No. 12228; E. faecalis, ATCC No. 14508; and Enterobacter cloacae, ATCC No. 13047 (all micro-organisms provided by ATCC, Manassas, VA). The organisms tested in this study were identified starting with the USP <51> required organisms and expanded to include others commonly found in wounds.
Challenge organisms S. aureus, P. aeruginosa, E. coli, MRSA, VRE, S. marcescens, A. baumannii, P. mirabilis, S. epidermidis, E. faecalis, and E. cloacae were aseptically transferred onto fresh trypticase soy agar slants (TSA; Remel, Lenexa KS) and incubated for 18 to 24 hours at 32.5 (± 2.5)° C. Subsequent to incubation, the bacteria were harvested using sterile TS saline (EMD, Inc, Gibbstown, NJ) with a sterile cotton swab to dislodge the organisms from the agar surface. Challenge organism C. albicans was aseptically transferred onto fresh slants of Sabouraud dextrose agar (SDA; Remel, Lenexa, KS) and incubated for 44 to 52 hours at 22.5 ± 2.5° C (mean ± STDEV). Challenge organism A. brasiliensis was aseptically transferred onto fresh SDA slants and incubated for 6 to 10 days at 22.5 ± 2.5° C (mean ± STDEV). Subsequent to incubation, C. albicans and A. brasiliensis both were harvested using sterile TS saline with a sterile cotton swab to dislodge the organisms from the agar surface. The A. brasiliensis suspension was filtered through sterile gauze to remove hyphal fragments. The resulting suspensions of each challenge organism were washed. A separate suspension of each organism was prepared for each lot of solution (lot numbers 9241M01, 9241M02, and 8411M18) tested. All challenge organisms were spectrophotometrically adjusted in sterile TS saline to a concentration of approximately 1.0 x 107 to 1.0 x 108 colony forming units (cfu/mL).
For each challenge organism and batch of polyhexanide 0.1% and betaine 0.1% solution to be tested, one 20-mL sample of the solution and one 20-mL sample of TS saline for the inoculum control was aseptically dispensed into appropriate sample containers. For each challenge organism and one batch of polyhexanide 0.1% and betaine 0.1% solution to be tested, the product was diluted 1:10 using Dey-Engley neutralizing broth (DEB; Becton Dickinson, Franklin Lakes, NJ). Recovery medium control testing was performed on two lots of the polyhexanide 0.1% and betaine 0.1% solution (Batch Identification: 9241M01, 9241M02, and 8411M18). A control sample was prepared with trypticase soy broth (TSB; Remel, Lenexa, KS). Both tubes were inoculated with sufficient inoculum to result in 10 cfu to 100 cfu of challenge organisms per plate. Inoculated tubes were incubated for 10 minutes to allow for neutralization at ambient temperature. Appropriate aliquots from each tube were plated in triplicate on TSA for the bacteria and SDA for the fungi.
All test and inoculum control samples were prepared with an appropriate inoculum suspension to achieve a final concentration of 1.0 x 105 to 1.0 x 106 cfu/mL. Immediately after inoculation, a 1-mL aliquot from each inoculum control, for each challenge organism, was aseptically transferred to a 9-mL DEB blank and allowed to neutralize for 10 minutes at ambient temperature. Subsequent to neutralization, all inoculum control samples were serially diluted using additional DEB blanks and appropriate dilutions plated in triplicate on either TSA for the bacteria or SDA for the fungi. At 7, 14, and 28 days after inoculation, a 1.0-mL aliquot from each lot of the polyhexanide 0.1% and betaine 0.1% solution, for each challenge organism, was aseptically transferred to a 9-mL DEB blank, and the inoculation and neutralization processes were repeated. Dilutions were plated in triplicate. All bacterial plates were incubated for 3 to 5 days at 32.5 ± 2.5° C (mean ± STDEV). Yeast plates were incubated for 3 to 5 days at 22.5 ± 2.5° C (mean ± STDEV), and mold plates for 3 to 7 days at 22.5 ± 2.5° C (mean ± STDEV).
Plate counts were determined and log reduction calculated as described in the USP<51> standard. The growth reduction in comparison to the starting value was determined according to USP<51>. The USP<51> standard requires not less than a 2-log reduction from the initial count at 14 days, and no increase from the 14 day count at 28 days for bacteria, and no increase from the initial calculated count at 14 and 28 days for yeast and molds.
There was no control material, but the neutralization scheme was validated with the recovery medium control. This assay validates the ability of the test system to recover the challenge organisms in the presence of the test articles. 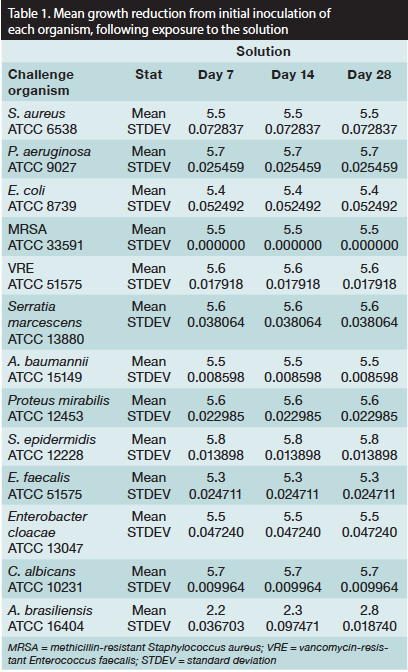
Results
The mean growth reduction from the initial value was identical at 7, 14, and 28 days following exposure to each of the three batches of the polyhexanide 0.1% and betaine 0.1% solution in all micro-organisms except A. brasiliensis. The mean log reductions seen in each micro-organism, except A. brasiliensis, were above 5-log, as well as the accepted USP <51> standard of 2-log (see Table 1). In A. brasiliensis, the mean reductions were 2.3-log, 2.8-log, and 2.8-log at 7, 14, and 28 days, respectively.
Discussion
According to the USP <51> guidelines, in vitro microbial reductions of at least 2-log or greater demonstrate inhibition of micro-organism activity. A wide range of micro-organisms was selected for this study, including aerobic and anaerobic bacteria, antibiotic-resistant bacteria, mold, and yeast, providing a quantitative demonstration of antimicrobial activity. The specific micro-organisms tested conform to the USP <51> guidelines. With the exception of A. brasiliensis, each of the micro-organisms tested had a growth reduction >5-log in the presence of the study products. Although A. brasiliensis also showed a growth reduction, use of the solution formulation met the 2-log USP standard. Per results of in vitro and in vivo study,22,23 the Aspergillus species are quite resistant to antibiotics; azoles (specifically voriconazole) and amphotericin B are the agents of choice in combating Aspergillus infections. This study of a combination containing 0.1% polyhexanide and 0.1% betaine solution found in vitro 5-log reductions in antimicrobial activity in 12 of the 13 micro-organisms tested. The solution met USP guidelines for in vitro antimicrobial activity at 14 and 28 days.
The in vitro log reduction induced by the combination of 0.1% polyhexanide and 0.1% of betaine in this study may help explain, at least in part, observed in vivo study results. In a randomized controlled porcine study,24 superficial wounds cleansed with polyhexanide healed in an average of 22.9 days compared to 24.1 days for wounds in the control group (P <0.05). In a case series of 10 patients with chronic wounds of varying etiology (including seven chronic leg wounds) previously cleansed with saline, polyhexanide/betaine cleansing was reported to improve patient-reported quality of life and reduce wound odor, exudate, pain, and wound size assessed by serial wound photography.25 In a retrospective case-controlled study13 of 112 patients with chronic leg ulcers, outcomes of wounds cleansed with polyhexanide/betaine were compared to those cleansed with saline or Ringer’s solution; 89% of wounds in the saline/solution and 79% in the polyhexanide/betaine group healed within 6 months. In wounds that healed, the mean time to healing was shorter in the polyhexanide/betaine group (3.3 months) than in the control group (4.4 months) (P <0.0001). In a single blind, randomized, controlled study26 of 40 patients with chronic leg ulcers, the use of polyhexanide/betaine was compared with saline cleaning for a period of 4 weeks. No differences in wound size reduction were observed, but patients in the polyhexanide/betaine group reported significantly less wound pain and had significantly lower wound pH values (P <0.05), a factor associated with improved wound healing in chronic venous ulcers.
Limitations
This study did not have a control group to evaluate the antibacterial effects of just the excipients. However, the solution contains only small amounts of sodium hydroxide to adjust pH.
Although the method did not include testing in the presence of serum or wound exudate that might interfere with antimicrobial activity in the clinical environment, the recommended use of the solution as an aid to cleaning wounds would reduce the presence of wound debris in vivo and thus minimize any impact of this potential issue in translating the results into clinical practice.
An in vitro study permits the generation and testing of mechanistic hypotheses, but these results cannot be transferred to clinical practice without supporting clinical research. The micro-organisms studied, although from common species seen in wounds, are not fully representative of the type of bacteria seen in clinical practice. However, the antimicrobial activity seen against these species is at least suggestive of a mechanism underlying the positive data reported when polyhexanide/betaine is used clinically.17,29-31
Conclusion
The results of this study demonstrate a significant (5-log and higher) reduction in bacterial load in vitro in 12 of 13 micro-organisms commonly present in chronic wounds. As with all in vitro studies, the results observed may not translate into a clinical benefit nor be representative of the wide range of situations seen in clinical practice. However, this study provides objective data of the product’s in vitro antimicrobial activity, adding to the increasing body of evidence suggesting the clinical effectiveness of 0.1% polyhexanide/0.1% betaine for wound cleaning. Further large well-designed clinical studies are required to confirm the in vitro and data from small studies that suggest the product has value in the management of chronic wounds.
Mr. Minnich is the Knowledge and Process Manager, Medical Scientific Affairs; Ms. Stolarick is the Corporate Vice President, Regulatory Affairs; and Prof. Unverdorben is the Chief Medical Officer and Senior Vice President, Medical Scientific Affairs, B Braun Medical Inc, Allentown, PA. Dr. Wilkins is an independent healthcare consultant. Mr. Chilson is a microbiologist, Moog Medical Devices Group, Rush, NY. Dr. Pritt is the Director, Biological Test Center, Irvine, CA. Please address correspondence to: Kevin E. Minnich, MBA, B Braun Medical Inc, 901 Marcon Boulevard, Allentown, PA 18109; email: kevin.minnich@bbraun.com.
1. Lazarus GS, Cooper DM, Knighton DR, Margolis DJ, Pecoraro RE, Rodeheaver G, et al. Definitions and guidelines for assessment of wounds and evaluation of healing. Arch Dermatol. 1994;130(4):489–493.
2. Franz MG, Robson MC, Steed DL, Barbul A, Brem, H, Cooper DM, et al. Guidelines to aid healing of acute wounds by decreasing impediments to healing. Wound Repair Regen. 2008;16:723–748.
3. Edwards R, Harding KG. Bacteria and wound healing. Curr Opin Infect Dis. 2004;17:91–96.
4. Gottrup F, Apelqvist J, European Wound Management Association Patient Outcome Group, Price P. Outcomes in controlled and comparative studies on non-healing wounds: recommendations to improve the quality of evidence in wound management. J Wound Care. 2010;19:237–268.
5. Nagoba BS, Wadher BJ, Rao AK, Kore GD, Gomashe AV, Ingle AB. A simple and effective approach for the treatment of chronic wound infections caused by multiple antibiotic resistant Escherichia coli. J Hosp Infect. 2006;69:177–180.
6. Robson MC. Wound infection — a failure of wound healing caused by an imbalance of bacteria. Surg Clin N Am. 1997;77:637–650.
7. Warriner R, Burrell R. Infection and chronic wound: a focus on silver. Adv Skin Wound Care. 2005:18:2–12.
8. Vandenbulcke K, Horvat LIL, De Mil M, Slegers G, Beel H. Evaluation of the antibacterial activity and toxicity of two new hydrogels: a pilot study. Int J Lower Extremity Wounds. 2006;5(2):109–114.
9. Chu CC, Williams DF. Effects of physical configuration and chemical suture of suture materials on bacterial adhesion: a possible link to wound infection. Am J Surg. 1984;147:197–204.
10. Baron EJ, Peterson LR, Finegold SM. Laboratory methods for detection of antibacterial resistance. In: Diagnostic Microbiology, 11th ed. London, UK: Mosby;2002:229–250.
11. Schmit-Neuerburg KP, Bettag C, Schlickewei W, Fabry W, Hanke J, Renzing-Kohler K, et al. [Effectiveness of an improved antiseptic in treatment of contaminated soft tissue wounds]. Chirurg. 2001;72:61–71.
12. Valenzuela AR, Perucho NS. [The effectiveness of a 0.1% polyhexanide gel]. Rev Enferm. 2008;31:7–12.
13. Andriessen A, Eberlein T. Assessment of a wound cleansing solution in the treatment of problem wounds. WOUNDS. 2008;20:171–175.
14. Kaehn K, Eberlein T. In-vitro test for comparing the efficacy of wound rinsing solutions. Br J Nurs. 2009;18(11):S4–S10.
15. Rose F, Swain G. Bisguanides having antibacterial activity. J Chem Soc. 1956;850:4422–4425.
16. Davies A, Bentley M, Field BS. Comparison of the action of vantocil, cetrimide and chlorhexidine on Escherichia coli and its spheroplasts and the protoplasts of Gram-positive bacteria. J Appl Bacteriol. 1968;31:448–461.
17. Ikeda T, Tazuke S, Bamford C, Ledwith A. Spectroscopic studies on the interaction of polymeric in-chain biguanide biocide with phospholipic membranes as probed by 8-anilinonaphthalene-1-sulphonate. Bull Chem Soc Jpn. 1985;58:705–709.
18. Kaehn K. Polihexanide: a safe and highly effective biocide. Skin Pharmacol Physiol. 2010;23(suppl):7–16.
19. Domsch A. Chemistry and application of undecylenic acid and derivatives thereof for cosmetics. SÖFW-Journal. 1994;120:322–329.
20. Müller G, Koburger T, Jethon FUW, Kramer A. Comparison of the bactericidal efficacy and in vitro cytotoxicity of Lavasept® and Prontosan®. GMS Krankenhaushygiene Interdisziplinär. 2007;2(2):1-11.
21. United States Pharmacopeia, National Formulary (USP 32- NF 27) <51> Antimicrobial Effectiveness Testing. The United States Pharmacopeial Convention. 2009(1):67-69.
22. Lass-Florl C, Perkhofer S. in vitro susceptibility-testing in Aspergillus species. Mycoses. 2008;51:437–446.
23. Brahm H, Segal BH. Aspergillosis. New Engl J Med. 2009;360(18):1870–1884.
24. Kramer A, Roth B, Müller G, Rudolph P, Klöcker N. Influence of the antiseptic agents polyhexanide and octenidine on FL cells and on healing of experimental superficial aseptic wounds in piglets. A double-blind, randomised, stratified, controlled, parallel-group study. Skin Pharmacol Physiol. 2004;17(3):141–146.
25. Horrocks A. Prontosan wound irrigation and gel: management of chronic wounds. Br J Nurs. 2006–2007;15(22):1222–1228.
26. Romanelli M, Dini V, Barbanera S, Bertone MS. Evaluation of the efficacy and tolerability of a solution containing propyl betaine and polyhexanide for wound irrigation. Skin Pharmacol Physiol. 2010;23(suppl):41–44.
