



A Clinical Minute: Improving Outcomes and Quality of Life for Patients With Chronic Venous Ulcers
Chronic venous ulcers (CVU) are considered the most common leg ulcers in the ambulatory elderly population in developed countries.1 Associated pain, exudate, and odor have a major impact on a person’s quality of life (QoL). Most of these ulcers are colonized; many are critically colonized or infected during the episode of illness. If total healing is unattainable, which frequently is the case, most patients choose to preserve their QoL, concluding symptom relief is more important than healing.2
Decreasing critical colonization and infection can promote QoL with improvement in pain, exudate amount, itching, and odor. Some patients report pain with antimicrobial agents such as silver-containing dressings, necessitating a change in (and subsequently lengthening of) the treatment plan.3 Long healing times and high recurrence rates worsen the overall impact of having a CVU. Aerosolization of bacteria during dressing changes can lead to further contamination and foster the cycle of issues impacting QoL. In their study of the bacteria in the environment and on surfaces during chronic wound dressing changes, Slekovec et al4 determined bacteria in air samples are more prevalent than on surfaces; the majority of the bacteria were Staphylococcus aureus and Pseudomonas aeruginosa. As such, utilization of a product that can provide a barrier to bacterial penetration and inhibit growth within wound dressings can thwart opportunistic infections from spreading and may improve overall QoL.
In an effort to minimize the spread of bacteria, clinicians can use a dressing that functions as a spot-on barrier by killing the bacteria within the dressing substrate. BIOGUARD® Barrier Dressings (Derma Sciences, Inc, Princeton, NJ) provide a barrier to bacterial penetration and result in >5-log (99.999%) kill of a broad spectrum of microbes, including antibiotic-resistant organisms. PolyDADMAC is an advanced cationic biocide polymer, bound to the dressing substrate, which kills the bacteria within the dressing, potentially preventing the ability of the bacteria to become airborne and cross-contaminate. Additionally, the use of BIOGUARD® non-adherent dressings applied to the CVU, followed by wrapping the affected leg with a BIOGUARD® rolled gauze or conforming bandage, can reduce the risk of bacterial contamination and therefore improve overall QoL.
Case 1. A 68-year-old man had a history of recurrent CVUs for more than 15 years during which he had skin grafts and numerous topical treatments. On admission to the author’s facility, he had a CVU measuring 5.9 cm x 3.1 cm x 0.2 cm. He initially was provided BIOGUARD® non-adherent dressing on March 16, 2015, and his leg was wrapped with BIOGUARD® wrap followed by a 2-layer compression wrap. His wound progressed well over 11 weeks; on June 1, 2015, it measured 3.2 cm x 2.7 cm x 0.1 cm (see Figures 1a,b,c). 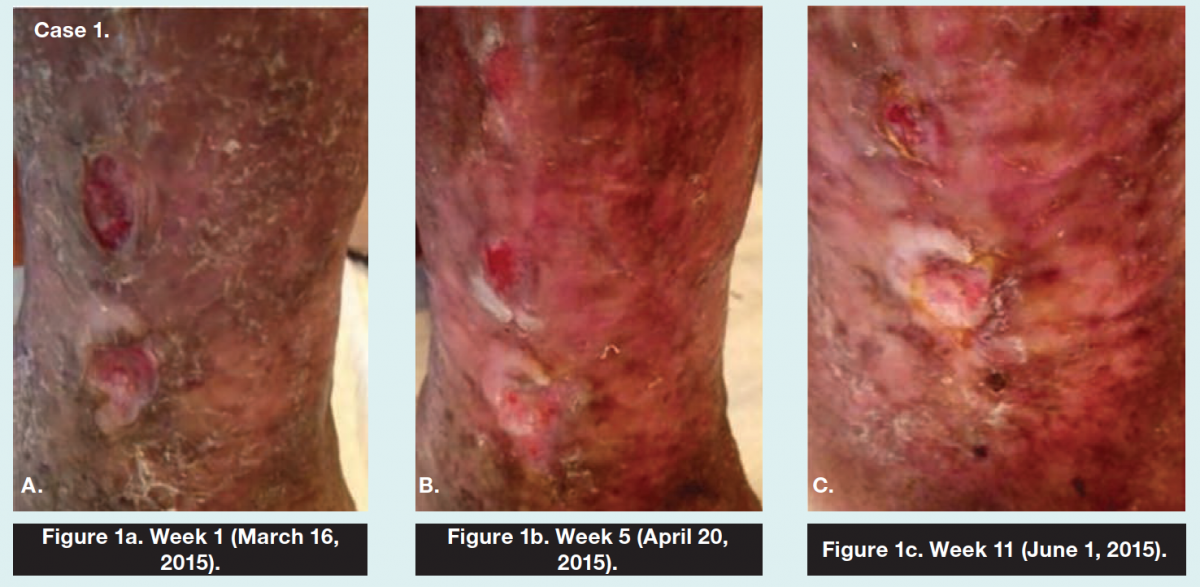
Case 2. A 52-year-old man had a history of deep vein thrombosis and a subsequent CVU formation measuring 2.5 cm x 3.8 cm x 0.1 cm on admission. His previous treatment included generic silver sulfadiazine cream and oral antibiotics for an infection. BIOGUARD® and compression were initiated on April 27, 2015. On June 1, 2015, wound size decreased to 0.5 cm x 0.5 cm x 0.1 cm (see Figures 2a,b,c). 
For more information on BIOGUARD® Barrier Dressings visit www.dermasciences.com.
References
1. Margolis DJ, Bilker W, Santanna J, Baumgarten M. Venous leg ulcer: incidence and prevalence in the elderly. J Am Acad Dermatol. 2002;46(3):381–386.
2. Mudge E, Holloway S, Simmonds W, Price P. Leg ulcers. Living with venous leg ulceration: issues concerning adherence. Br J Nurs. 2006;15(21):1166–1171.
3. Coutts P, Sibbald RG. The effect of a silver-containing Hydrofiber dressing on superficial wound bed and bacterial balance of chronic wounds. Int Wound J. 2005;2(4):348–356.
4. Slekovec C, Faivre B, Humbert P, Bertrand X, Hocquet D, Pazart L, Talon D. Chronic wound care leads to the bacterial contamination of the environment. Ann Dermatol Venereol. 2012;139(12):798–802.
A Clinical Minute is made possible through the support of Derma Sciences, Inc, Princeton, NJ. The opinions and statements provided in A Clinical Minute are specific to the respective authors and not necessarily those of OWM or HMP Communications.
This article was not subject to the Ostomy Wound Management peer-review process.
Chronic venous ulcers (CVU) are considered the most common leg ulcers in the ambulatory elderly population in developed countries.1 Associated pain, exudate, and odor have a major impact on a person’s quality of life (QoL). Most of these ulcers are colonized; many are critically colonized or infected during the episode of illness. If total healing is unattainable, which frequently is the case, most patients choose to preserve their QoL, concluding symptom relief is more important than healing.2
Decreasing critical colonization and infection can promote QoL with improvement in pain, exudate amount, itching, and odor. Some patients report pain with antimicrobial agents such as silver-containing dressings, necessitating a change in (and subsequently lengthening of) the treatment plan.3 Long healing times and high recurrence rates worsen the overall impact of having a CVU. Aerosolization of bacteria during dressing changes can lead to further contamination and foster the cycle of issues impacting QoL. In their study of the bacteria in the environment and on surfaces during chronic wound dressing changes, Slekovec et al4 determined bacteria in air samples are more prevalent than on surfaces; the majority of the bacteria were Staphylococcus aureus and Pseudomonas aeruginosa. As such, utilization of a product that can provide a barrier to bacterial penetration and inhibit growth within wound dressings can thwart opportunistic infections from spreading and may improve overall QoL.
In an effort to minimize the spread of bacteria, clinicians can use a dressing that functions as a spot-on barrier by killing the bacteria within the dressing substrate. BIOGUARD® Barrier Dressings (Derma Sciences, Inc, Princeton, NJ) provide a barrier to bacterial penetration and result in >5-log (99.999%) kill of a broad spectrum of microbes, including antibiotic-resistant organisms. PolyDADMAC is an advanced cationic biocide polymer, bound to the dressing substrate, which kills the bacteria within the dressing, potentially preventing the ability of the bacteria to become airborne and cross-contaminate. Additionally, the use of BIOGUARD® non-adherent dressings applied to the CVU, followed by wrapping the affected leg with a BIOGUARD® rolled gauze or conforming bandage, can reduce the risk of bacterial contamination and therefore improve overall QoL.
Case 1. A 68-year-old man had a history of recurrent CVUs for more than 15 years during which he had skin grafts and numerous topical treatments. On admission to the author’s facility, he had a CVU measuring 5.9 cm x 3.1 cm x 0.2 cm. He initially was provided BIOGUARD® non-adherent dressing on March 16, 2015, and his leg was wrapped with BIOGUARD® wrap followed by a 2-layer compression wrap. His wound progressed well over 11 weeks; on June 1, 2015, it measured 3.2 cm x 2.7 cm x 0.1 cm (see Figures 1a,b,c).
Case 2. A 52-year-old man had a history of deep vein thrombosis and a subsequent CVU formation measuring 2.5 cm x 3.8 cm x 0.1 cm on admission. His previous treatment included generic silver sulfadiazine cream and oral antibiotics for an infection. BIOGUARD® and compression were initiated on April 27, 2015. On June 1, 2015, wound size decreased to 0.5 cm x 0.5 cm x 0.1 cm (see Figures 2a,b,c).
For more information on BIOGUARD® Barrier Dressings visit www.dermasciences.com.
A Clinical Minute is made possible through the support of Derma Sciences, Inc, Princeton, NJ. The opinions and statements provided in A Clinical Minute are specific to the respective authors and not necessarily those of OWM or HMP Communications.This article was not subject to the Ostomy Wound Management peer-review process.
References
1. Margolis DJ, Bilker W, Santanna J, Baumgarten M. Venous leg ulcer: incidence and prevalence in the elderly. J Am Acad Dermatol. 2002;46(3):381–386.
2. Mudge E, Holloway S, Simmonds W, Price P. Leg ulcers. Living with venous leg ulceration: issues concerning adherence. Br J Nurs. 2006;15(21):1166–1171.
3. Coutts P, Sibbald RG. The effect of a silver-containing Hydrofiber dressing on superficial wound bed and bacterial balance of chronic wounds. Int Wound J. 2005;2(4):348–356.
4. Slekovec C, Faivre B, Humbert P, Bertrand X, Hocquet D, Pazart L, Talon D. Chronic wound care leads to the bacterial contamination of the environment. Ann Dermatol Venereol. 2012;139(12):798–802.

{kind=link}
{kind=link}