



The Association Between Pressure Ulcer/Injury Development and Short-term Mortality in Critically Ill Patients: A Retrospective Cohort Study





Abstract
Pressure ulcers/injuries (PU/Is) affect the social, mental, and physical well-being of patients; increase treatment costs; prolong hospital stays; increase patient risk for infections; and may independently decrease life expectancy. Purpose: The aim of this retrospective study was to examine the association between PU/I development and mortality in a large cohort of consecutively admitted critically ill patients. Methods: Data from adult patients ( >18 years of age) admitted to an intensive care unit (ICU) between 2010 and 2013 were extracted from the ICU electronic clinical information system. Patients were excluded if they had a PU/I present on admission, no recorded admission modified Jackson/Cubbin (mJ/C) or Sequential Organ Failure Assessment (SOFA) score, or their ICU outcome was undetermined. The mJ/C risk scale (score range 9–48) was used to assess the PU/I risk (the lower the score, the higher the PU/I risk), the SOFA score (score range 0–24; the higher the SOFA score, the sicker the patient, with a higher risk of death) was used to assess the severity of the condition and outcome. ICU outcome was defined as 1) moved from the ICU to a ward/recovering or 2) no response to ICU treatment/deceased. All data were transferred to statistical software for analysis. Logistic regression analysis was used to examine the outcome related to PU/I development, SOFA, and mJ/C scores. Descriptive contingency tables of different scenarios were used to further evaluate relationships among different risk factors related to mortality; the Wald χ2 test was used to assess the statistical significance of the contingency tables. Results: Of the 6582 patients admitted, 6089 were included for analysis. Two hundred, one (201) had a PU/In on admission, 212 had missing mJ/C or SOFA scores, and ICU outcome was undetermined in 80 patients. Patient mean age was 61.1 ± 15.8 (range 18–94) years; 3891 (63.9%) were male, average length of stay (LOS) was 3.6 days, denoted by quartile (Q) (median 1.58 days; Q1: 0.9, Q3: 3.9 days), and 1589 (26.1%) stayed 3 days or more in the ICU. The incidence of PU/I was 6.9% (423 patients), and ICU mortality rate was 9.1% (n=553). The mean LOS of patients with PU/I was 13.35 ± 15.56 days (median 8.95, Q1: 4.88, Q3: 16.2) and 2.84 ± 3.87 days for patients with no PU/I (median: 1.20, Q1: 0.90, Q3: 3.17; P <.0001). Mean LOS was 3.42 ± 5.95 days (median: 1.30, Q1: 0.90, Q3: 3.70) among recovering and 5.00 ± 7.17 days among deceased patients (median 2.56, Q1: 1.26, Q3: 6.40; P <.0001). The proportion of patients with an admission mJ/C score of 29 or less ranged from 48.8% to 51.5%, and the mean SOFA score was 7.0 ± 3.2. PU/I development and SOFA or mJ/C scores were independent predictors of mortality. The probability of a negative outcome was higher in persons with PU/Is compared to persons with no PU/Is. Persons with lower SOFA scores (ie, less severely ill patients) and higher mJ/C scores for each factor separately (ie, at low risk of PU/I development) each factor separately had a lower mortality risk. Conclusion: PU/I development in critically ill patients treated at an ICU is an independent predictor of mortality, even though the PU/I incidence and hospital mortality were relatively low. The ICU admission SOFA and mJ/C score also were independent prognosticators of ICU mortality. Future research could focus on the role of different steps in the cascade of PU/I development, especially to the role of inflammation.
Introduction
Patients with a high Sequential Organ Failure Assessment (SOFA) score on admission to an intensive care unit (ICU) tend to have higher mortality rates than patients with a low SOFA score; in a prospective, multicenter study1 among 1449 patients (mean age 55 ± 15 years, 64% male, with a mean ICU length of stay [LOS] of 5.0 days), the mean SOFA score of all patients was 8.2, but the scores were significantly higher among nonsurvivors than survivors (13.6 ± 4.8 vs 6.7 ± 4.5; P <.001). A systematic review2 on the importance of SOFA has shown that the higher the SOFA score, the higher the mortality rate. A prospective cohort study3 (N = 299) among medical-surgical ICU patients requiring mechanical ventilation for more than 24 hours found the SOFA score may predict the development of pressure ulcers/injuries (PU/Is). The same conclusion was reached in retrospective cohort study⁴ among 4899 consecutively admitted patients treated in a medical-surgical ICU,4 and a systematic review5 on PU/I risk factors also was in accordance, although the role of SOFA as an independent risk factor could not be ascertained. A retrospective study6 conducted across the United States (2008–2012) that included approximately 7 million admissions annually showed PU/I development significantly prolonged hospital stay (from a mean of 4.6 for patients without PU/Is to a mean of 11.1 days for patients with PU/Is) and increased mortality (1.8% vs 9.1%). The same results were observed in a multicenter cohort study7 among 9605 ICU patients where ICU stay and hospital stay (17.5 ± 13.0 vs 4.7 ± 4.6 days and 34.6 ± 24.7 vs 14.5 ± 20 days, respectively; P <.001) were longer for patients with than without a PU/I. Additionally, ICU and hospital mortality rates were higher in the PU/I group (31.2% vs 7.6% and 50.7% vs 13.8%, respectively; P <.001). Mortality risk also is increased for mechanically ventilated ICU patients,7-10 patients in long-term care, and elderly patients11-13 if they developed PU/Is.
The prevalence of PU/Is in ICUs has decreased during the last 25 years from approximately 50% to less than 10%.14-19 This trend is probably due to a combination of factors including increased awareness and knowledge of the pathophysiology of PU/I development and advances in intensive care methods and preventive measures regarding PU/Is, especially the use of specialty mattresses. At the same time, hospital mortality of patients admitted to ICUs has decreased significantly despite an increase in the severity of the illnesses of treated patients.20 Thus, it is interesting to learn whether there is an association between ICU-acquired PU/Is and the immediate outcome of critically ill patients.
The purpose of this retrospective study was to examine the association between PU/I development and mortality in critically ill patients.
Methods
The Turku University Hospital adult medical-surgical ICU has 24 beds and serves a population of 700 000. All surgical and medical intensive care patients in the region except patients with major burns and patients undergoing solid organ transplantation are treated in this tertiary hospital. Bed occupancy was approximately 79% during the study period.
Patients. On admission, patients are classified based on their treatment needs by the treating physician, who determines the main admission diagnosis and other diagnoses and is responsible for the input of pertinent patient data into the ICU electronic clinical documentation and information system (Clinisoft, GE Healthcare, Buckinghamshire, UK). Nurses with special training in using the modified Jackson/Cubbin (mJ/C) scale for PU/I risk assessment and in wound identification and care enter relevant information into the database, including the type and frequency of skin cleansing, skin integrity, PU/I presence, and National Pressure Ulcer Advisory Panel/European Pressure Ulcer Advisory Panel (NPUAP/EPUAP) PU/I classification.21 All laboratory results and medication data also are entered. The data system calculates both the mJ/C and SOFA scores.
Patient data from all ICU admissions between January 2010 and December 2013 (inclusion criterion age >18 years old) were retrospectively collected. Patients with 1 or more PU/Is present on admission were excluded unless they acquired 1 or more PU/Is during their ICU stay. Patients without any information about their SOFA or mJ/C scores and patients whose ICU outcome could not be determined also were excluded.
Study variables. PU/I risk was assessed using the mJ/C risk scale.18,22,23 The first PU/I risk assessment was performed when the patient was admitted to the ICU; subsequent assessments were performed daily. If the mJ/C score was 29 points or less,18,23 PU/I risk was considered high or extremely high and patients were placed on an appropriate protective mattress if one had not already been provided. Otherwise, PU/I prevention care followed the NPUAP-EPUAP guidelines,21 and repositioning therapy was intensified as much as possible with consideration for the condition of the patient. SOFA scores24 were collected on admission and daily thereafter. Information on age, gender, LOS (noted in quartiles [Q]), and ICU transfer or discharge were extracted from the database.
mJ/C scale. The mJ/C scale consists of 12 main categories of specific patient variables, each graded from 1 (high risk) to 4 (low risk). These categories include age, weight/tissue viability, past medical history, general skin condition, mental condition, mobility, hemodynamics, respiration, oxygen requirements, nutrition, incontinence, and hygiene. Three (3) subcategories (transport to examinations or treatments, use of blood products, and hypothermia) can lead to the deduction of 1 point. Thus, the minimum score is 9 and the maximum score is 48, with a lower score indicating a higher risk for PU/I development.
SOFA. The SOFA scale includes 6 organ failure assessment categories: liver (serum bilirubin concentration), coagulation (platelet count), renal dysfunction (creatinine concentration), cardiovascular system (mean arterial pressure or need for vasopressors), presence of respiratory disorder (PaO2/FiO2) and nervous system status (Glasgow Coma Score [GCS]). The GCS assesses ocular, motor, and verbal responsiveness. Each category is scored from 0 (low risk) to 4 (high risk), so the SOFA score ranges from 0 to 24. Missing values in a single SOFA subgroup were given a value of zero (ie, normal), a situation mainly relevant to bilirubin concentration, which is not routinely collected on the day of admission. The SOFA score system has been validated; the higher the score, the more severe the patient’s condition and the higher the mortality.2
Outcome. The primary endpoint was the ICU outcome, which was defined as: 1) moved from ICU to a ward, recovering, 2) no response to ICU treatment/deceased, or 3) transferred elsewhere from the ICU and outcome could not be determined. The patients in group 3 were excluded from analysis. The overall hospital mortality rate of these ICU patients was collected from the database.
The primary variable of interest was PU/I development during the ICU stay and the overall ICU outcome, and the secondary variables were the SOFA and mJ/C scores, assessed separately or together.
Data collection. All data were retrospectively extracted by the database administrator of the ICU from the clinical documentation and information system. All patient, nurse, and physician identifiers were removed at this stage from the data sets. The data sets were transferred by the statistician to SAS 9.4 (SAS Institute Inc, Cary, North Carolina).
Data analysis. For data analysis, no distinction was made regarding those who developed 1 PU/I or several PU/Is during their ICU stay (ie, all were classified as having developed a PU/I during their ICU stay). LOS values were calculated from exact times. Deceased/transfers were recorded as such.
For initial assessment, the data were analyzed by first day mJ/C scores (<29 or >0) or SOFA scores (<6, 6–12, and ≥12), PU/I status (developed or not during ICU stay), and ICU outcome (alive or deceased). The χ2 test was used to compare categorical data in the different groups (see Table 1 and Table 2). Thereafter, the probability of the short-term outcome was determined using a logistic regression model25,26 that utilized the categorical values of both the mJ/C and the SOFA scores. For logistic regression, the response variable was binary and the relationship between response and explanatory variables was determined using the logit link function:
{kind=link}
logit(π)=log(π/(1-π))= β0+β1x1+ ...+βkxk
where π is the probability of a positive outcome, x1,x2,…,xk are the values of the explanatory variables, and β0,β1,…,xk are the estimates of the predictability values of the different explanatory odds ratios (OR) used to summarize the results of the logistic regression modeling. The OR is closely connected to logistic regression, and it can be used to evaluate the effect of a single risk factor while other risk factors are fixed. The OR was used to examine the primary hypothesis H1, which denotes that PU/I(s) acquired during an ICU stay increase the risk of a negative, short-term outcome of ICU patients.
The primary hypothesis was evaluated using a logistic regression model with the following explanatory variables: admission SOFA score (groups <6, 6–11, ≥12), admission mJ/C score (≤29, ≥30), PU/I status (ICU acquired PU/Is, no PU/Is), and interactions between 1) SOFA score and PU status, between 2) SOFA score and mJ/C score, and between 3) PU/I status and mJ/C score.
logit(π)=log(π/(1-π))= β0+β1 *SOFAscore+
β2*mJ/Cscore+β3*PUstatus+β4*SOFAscore
*mJ/Cscore+β5*SOFAscore*PUstatus+β6
*mJ/Cscore*PUstatus
Logistic regression also was used to examine the correlation between mJ/C or SOFA scores and the negative short-term outcome of ICU patients.
In addition to the logistic regression model, descriptive contingency tables of different scenarios were used to further evaluate the relationships among different risk factors related to a negative outcome. The Wald χ2 test was used to assess the statistical significance of the contingency tables. A negative outcome was defined as no response to treatment or deceased.
Ethical approval. The study was approved by the Ethics Committee of Hospital District of Southwest Finland (T25/2011, 14.06.2011 §172).
Results
Of the 6582 patients whose data were retrospectively collected from the database (ie, all consecutively admitted patients), 212 patients had 1 or several PU/Is present-on-admission; of those, 11 also developed a PU/I after admission. Additionally, 212 were excluded because information about their SOFA or mJ/C scores was lacking, and 80 were excluded because their ICU outcome could not be determined, leaving 6089 patients included in the analysis. Patient mean age was 61.1 ± 15.8 (range 18–94) years; 3891 (63.9%) were male, average LOS was 3.6 days (median 1.58 days; Q1: 0.9, Q3: 3.9 days), and 1589 (26.1%) of the patients stayed 3 days or more in the ICU. During their ICU stay, 423 patients developed 1 or more PU/I (6.9% incidence), and 553 died (9.1% mortality rate) (see Table 1). The overall hospital mortality of these ICU patients was 11.1%. The mean LOS of patients who developed a PU/I was 13.35 ± 15.56 days (median 8.95, Q1: 4.88, Q3: 16.2) versus 2.84 ± 3.87 days for non-PU/I patients (median: 1.20, Q1: 0.90, Q3: 3.17; P <.0001, Mann Whitney Wilcoxon test for comparison of 2 non-gaussian samples). Mean LOS was 3.42 ± 5.95 days (median: 1.30, Q1: 0.90, Q3: 3.70) among patients who recovered and 5.00 ± 7.17 days among deceased patients (median 2.56, Q1: 1.26, Q3: 6.40; P <.0001, Mann Whitney Wilcoxon). The proportion of patients with a mJ/C score of 29 or less during the study period ranged from 48.8% to 51.5%. The mean patient SOFA score was 7.0 ± 3.2. Outcome could not be determined for 80 patients in the study (76 without PU/Is and 4 who developed a PU/I during the ICU stay).
The ICU mortality rate was significantly higher among patients who developed PU/Is during their ICU stay (73/423; 17.3%) than among those who did not develop PU/Is (480/5686; 8.4%; P <.0001) (see Table 1 and Table 2).
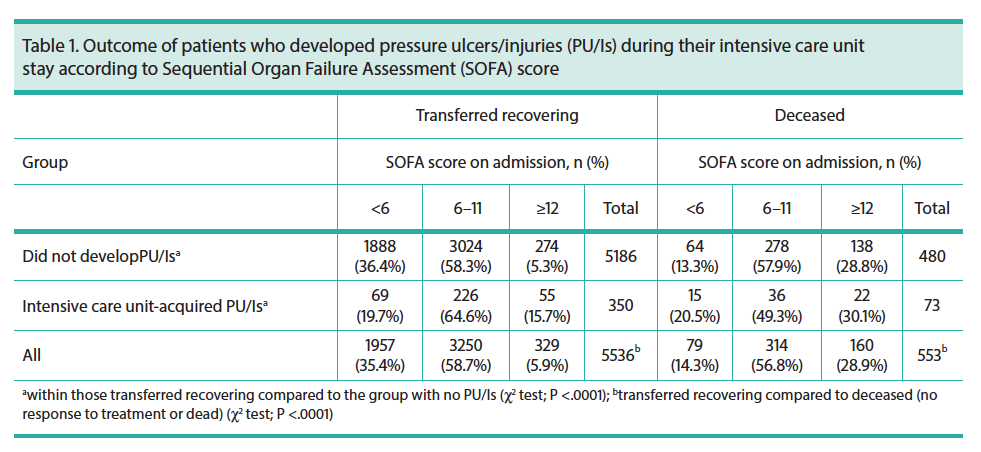
Significantly more of the deceased patients in the 2 groups, regardless of whether they developed (22/73; 30.1%) or did not develop PU/Is (138/480; 28.8%), had higher admission SOFA scores than those in the corresponding groups of patients who recovered (274/5186 [5.3%] and 55/350 [15.7%], respectively; P <.0001) (see Table 1).
Among the patients who recovered, persons with ICU-acquired PU/Is had significantly higher admission SOFA scores (>12; 55/350 [15.7%]) than persons who did not develop PU/Is (274/5186 [5.3%]) while in the ICU (P <.0001) (see Table 1).
Significantly more patients who died (436/553 [78.8%]) had admission mJ/C scores less than 30 (ie, were at higher risk for PU/Is) than those who recovered (2937/5536 [53.1%]; P <.0001) (see Table 2). Among the patients who recovered, significantly more patients with ICU-acquired PU/Is had low mJ/C scores on admission (219/350 [62.6%]) than persons with no PU/Is (2718/5186 [52.4%]; P = .0003).
Among patients without PU/Is who died, significantly more had a low (≤29) mJ/C score (382/480; 79.6%) than whose without PU/Is and who recovered (2718/5186 [52.4%]; P <.0001) (see Table 2).
Regardless of the mJ/C score, ICU-acquired PU/Is were more common in persons who died (73/553 [13.2%]) than who recovered (350/5536 [6.3%; P <.0001) (see Table 2).
Regression analysis. SOFA (P <.0001), mJ/C scores (P = .0002) on admission, and PU/I development (P <.0001) were significantly related with overall ICU outcome (see Table 3). The relationship between SOFA score on admission and PU/I development was also statistically significant (P <.0001), whereas the relationship between SOFA and mJ/C scores on admission (P = .0554) and the relationship between PU/I development and mJ/C score on admission (P = .1673) were not statistically relevant (see Table 3).
Using ORs to evaluate the primary hypothesis found that acquiring a PU/I during ICU stay significantly increased the risk of a negative outcome (no response to treatment or death) in the low SOFA score groups (<6 and 6–11) (see Table 4). Among patients with a SOFA score less than 6, the probability of a negative outcome was 4.74 times higher if the mJ/C score was less than or equal to 29 and 7.43 times higher if the mJ/C score was 30 or more if a PU/I emerged compared to the situation in which no PU/Is developed. In persons with SOFA scores between 6 and 11, the corresponding risk increase was 1.55-fold when the mJ/C score was 29 or less and 2.42-fold when the mJ/C score was 30 or more. In persons with SOFA scores 12 or more, ICU-acquired PU/Is did not increase the risk of a negative outcome (see Table 4).
Logistic regression showed a low mJ/C score to predict a negative overall outcome for patients during their stay at the ICU. When the combined effect of the mJ/C score by PU/I development and SOFA score was evaluated using ORs (see Table 5), having a higher mJ/C score reduced the risk of a negative patient outcome. This was especially true for patients who, at the same time, had low SOFA scores; in the group of patients with a SOFA score less than 6, the probability of a negative outcome was only 0.26 times in the non-PU/I group and 0.41 times in PU/I group if the mJ/C score on admission was high (ie, 30 or more) compared to patients with a low mJ/C score on admission (29 or less). In the group of patients with PU/I and a SOFA score between 6 and 11, the probability of a negative outcome was 0.50 times lower if the mJ/C score at admission was high (30 or more) compared to patients with low mJ/C on admission score (29 or less). The remaining comparisons failed to show statistically significant differences between persons with high or low mJ/C scores (see Table 5).
Discussion
The main finding of the present study was that PU/I development was an independent prognostic factor for mortality for patients admitted to the ICU and that both the SOFA and mJ/C scores obtained at ICU admission were independent prognostic factors for mortality.
Previous studies1,2 have demonstrated that patients with high SOFA scores on ICU admission have higher mortality rates during their ICU stay than patients with low SOFA scores and that having a PU/I versus not having a PU/I and persons who die versus those who recover have longer LOS, respectively.6,7 The current results are in concordance with these findings.
A database cohort study27 also has shown PU/Is increase the mortality risk of elderly patients and patients in long-term care (N =19 981; mean age 71.2 years). PU/I-associated mortality may reflect various systemic factors, such as diseases, geriatric conditions, and the frailty of an older population.12,13,27 A population-based study11 in the US where PU/Is were reported as a cause of death (N = 114 380) showed septic infections occur in approximately 40% of patients with PU/I-associated deaths and that nearly 80% of PU/I-associated deaths occurred in persons 75 years old or more. Incapacitating chronic and neurodegenerative conditions contribute to the spectrum of illnesses.
A multicenter cohort study7 in Brazil among 9605 ICU patients found that both the LOS and mortality of patients with PU/I, some of whom needed mechanical ventilation, were higher than of patients without PU/I. Furthermore, PU/Is increased long-term and hospital mortality in populations of critically ill, mechanically ventilated patients.8-10 In those studies, the PU/I incidence was 23.1% (27/117; mean age 65 years),8 19.5% (110/563; mean age 63 years),9 and 9.0% (30/332, mean age 63 years),10 and the corresponding overall hospital mortality was 29.0%, 48.7%, and 53.3%, respectively. In the current study, the corresponding rates were 6.9% and 11.1%. Mortality was related to the severity of the underlying diseases and the patients’ medical condition.
The current study found mortality was related to PU/I development, although the incidence of PU/I and hospital mortality was much lower than in the previously mentioned studies where PU/Is occurred in patients with a wide range of primary admission diagnoses and, as such, mortality probably was not the direct result of related illnesses.19
PU/Is have a multifactorial origin; there are numerous risk factors.5,10,28-30 Previously, neither severity of illness nor mortality risk scales, such as the mJ/C or SOFA, have been conclusively associated with the development of PU/Is in ICU patients,3,5,31 although retrospective cohort studies4,32 recently have indicated that both mJ/C and SOFA scales can be used to predict PU/I development. In this study, the SOFA and mJ/C scores determined on admission and that cover a number of PU/I risk indicators were shown to be clearly associated with the development of PU/Is during the ICU stay (see Table 1 and Table 2). It is of note that both scores predicted ICU patient mortality, regardless of whether the patient acquired a PU/I during the ICU stay.
The association of SOFA and mJ/C scores or PU/I status and mJ/C score on admission were not statistically significant (see Table 3, Table 4, and Table 5), which may indicate overlap of some of the variables that predict mortality within the SOFA and mJ/C scales. Nevertheless, a significant relationship was noted between SOFA and PU/I development, predicting mortality. High SOFA scores are associated with a risk of organ dysfunction/failure; high SOFA scores are also related to the intensity and balance between opposite inflammatory responses.33
Although it is possible that PU/Is, as such, are causally related to mortality, PU/I development may function as an early indicator of pending mortality. Oxidative stress and inflammatory reactions involving several biochemical mediators have been shown to play an important role in the pathophysiology of PU/I development and could well explain how and why PU/Is are related to mortality.28,34-37
Coslovsky et al38 presented an advanced model for predicting an adverse outcome of patients during their ICU stay. Among the 7680 patients included in the model, advanced age, prolonged capillary refill time, low blood pressure, mechanical ventilation, low oxygen saturation index, low GCS value, and Acute Physiology And Chronic Health Evaluation II diagnostic category were identified as factors for adverse outcomes. Even if the goal of the current study did not include development of a prognostic model, subscores of the SOFA and mJ/C scales reflected similar components.38 The current results may indicate that outcome is related to a combined effect of the characteristics considered in both ICU admission SOFA and the mJ/C, because both scores address the risk of PU/I development4,18,22 and mortality.
Limitations
This is a retrospective analysis, which carries a risk of unintentional bias due to variation of documentation over time. Among the patients studied, 212 lacked SOFA or mJ/C score data and were excluded from the analysis; this may have affected the statistical significance of the results. The authors used a default value of zero (ie, normal) for individuals missing SOFA subclass values (mainly bilirubin), and this also might have influenced the results. However, this is 1 of the largest consecutive adult cohorts of ICU patients ever studied, so the probability of bias inherent to retrospective studies is minimized. Nevertheless, the number of patients with PU/Is (including all stages) was rather limited, and it was not possible to analyze the association between outcome and PU/I stage or subcategories of either the SOFA or the mJ/C scale (for example, skin or specific organ failure or medications). In addition, the study timeline was 4 years, a duration of time during which care practices may have changed.
Also, some patients may have died soon after transfer from the ICU to the ward, but the effect of this cannot have been very pronounced because the difference between ICU and overall hospital mortality was small.
Conclusion
A retrospective, observational, consecutive cohort study involving data from 6089 critically ill adult patients analyzed the relationships among ICU mortality and PU/I development, PU/I risk score, and disease severity. PU/I development was found to be an independent predictor of no response to treatment or death of critically ill patients. Both the SOFA score and the mJ/C score, assessed when the patient was admitted to the ICU, independently predicted PU/I development and mortality.
PU/Is are apparently more deleterious than generally considered and their effect on mortality is apparently related to the pathophysiological process of PU/I development. The outcome (ie, PU/I development) from the pathophysiological cascade28, 37 — pressure, deformation, inflammation, and hypoxia — may be an early indicator of pending mortality. Future research could focus on the role of different steps in the cascade, especially the role of inflammation. Consequently, these indicators of a negative prognosis should prompt early interventions to prevent the development of PU/Is that may add to the forthcoming risk of mortality of intensive care patients. Further research to determine whether acting upon the risk factors identified in this study is warranted.
Acknowledgments
The study was supported by grants from the Service Division, Perioperative Services, Intensive Care Medicine and Pain Management (State research funding, grant 13693) of the Turku University Hospital Foundation. The language of the article was reviewed by Robert Paul, MD, PhD, certified translator.
Affiliations
Ms. Ahtiala is an authorized wound care nurse, Service Division, Perioperative Services, Intensive Care Medicine and Pain Management, Turku University Hospital, Turku, Finland. Mr. Kivimäki is a statistician, StatFinn Ltd, Turku, Finland. Dr. Laitio is a senior consultant in intensive care medicine, Service Division, Perioperative Services, Intensive Care Medicine and Pain Management, Turku University Hospital. Dr. Soppi is a senior consultant in internal medicine, Eira Hospital, Helsinki, Finland. Please address correspondence to: Maarit Ahtiala, RN, Service Division, Perioperative Services, Intensive Care Medicine and Pain Management, Turku University Hospital, POB 52, FI-20521 Turku, Finland; email: maarit.ahtiala@tyks.fi.
References
1. Moreno R, Vincent JL, Matos R, et al. The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Working Group on Sepsis related Problems of the ESICM. Intensive Care Med. 1999;25(7):686–696.
2. Minne L, Abu-Hanna A, de Jonge E. Evaluation of SOFA-based models for predicting mortality in the ICU: a systematic review. Crit Care. 2008;12(6):1–13.
3. Manzano F, Navarro MJ, Roldán D, et al; Granada UPP Group. Pressure ulcer incidence and risk factors in ventilated intensive care patients. J Crit Care. 2010;25(3):469–476.
4. Ahtiala M, Soppi E, Saari T. Sequential Organ Failure Assessment (SOFA) to predict pressure ulcer risk in intensive care patients – a retrospective cohort study. Ostomy Wound Manage. 2018;64(10):32–38.
5. Cox J. Pressure injury risk factors in adult critical care patients: a review of the literature. Ostomy Wound Manage. 2017;63(11):30–43.
6. Bauer K, Rock K, Nazzal M, Jones O, Qu W. Pressure ulcers in the United States’ inpatient population from 2008 to 2012: results of a retrospective nationwide study. Ostomy Wound Manage. 2016;62(11):30–38.
7. Ranzani OT, Simpson ES, Japiassú AM, Noritomi DT; Amil Critical Care Group. The challenge of predicting pressure ulcers in critically ill patients. A multicenter cohort study. Ann Am Thorac Soc. 2016;13(10):1775–1783.
8. Aboussouan LS, Lattin CD, Kline JL. Determinants of long-term mortality after prolonged mechanical ventilation. Lung. 2008;186(5):299–306.
9. Manzano F, Pérez-Pérez AM, Martínez-Ruiz S, et al. Hospital-acquired pressure ulcers and risk of hospital mortality in intensive care patients on mechanical ventilation. J Eval Clin Pract. 2014;20(4):362–368.
10. Becker D, Tozo TC, Batista SS, Mattos AL, et al. Pressure ulcers in ICU patients: Incidence and clinical and epidemiological features: a multicenter study in southern Brazil. Intens Crit Care Nurs. 2017;42(10):55–61.
11. Redelings MD, Lee NE, Sorvillo F. Pressure ulcers: more lethal than we thought? Adv Skin Wound Care. 2005;18(7):367–372.
12. Jaul E, Calderon-Margalit R. Systemic factors and mortality in elderly patients with pressure ulcers. Int Wound J. 2015;12(3):254–259.
13. Jaul E, Rosenzweig JP. A retrospective study of the impact of pressure ulcers on survival in elderly persons with chronic diseases. Ostomy Wound Manage. 2017;63(5):26–32.
14. Inman KJ, Sibbald WJ, Rutledge FS, Clark BJ. Clinical utility and cost effectiveness of an air suspension bed in the prevention of pressure ulcers. JAMA. 1993;269(9):1139–1143.
15. Takala J, Varmavuo S, Soppi E. Prevention of pressure sores in acute respiratory failure: a randomized, controlled trial. Clin Intens Care. 1996;7(5):228–235.
16. Bours GJ, De Laat E, Halfens RJ, Lubbers M. Prevalence, risk factors and prevention of pressure ulcers in Dutch intensive care units. Results of a cross-sectional survey. Intensive Care Med. 2001;27(10):1599–1605.
17. VanGilder C, Amlung S, Harrison P, Meyer S. Results of the 2008 – 2009 International Pressure Ulcer Prevalence™ Survey and a 3-year, acute care, unit-specific analysis. Ostomy Wound Manage. 2009;55(11):39–45.
18. Ahtiala M, Soppi E, Wiksten A, Koskela H, Grönlund JA. Occurrence of pressure ulcers and their risk factors in mixed medical-surgical ICU – a cohort study. J Intens Care Soc. 2014;15(4):2–4.
19. Ahtiala M, Kivimäki R, Soppi E. Characteristics of intensive care unit (ICU) patients with pressure ulcers present on admission, acquired in ICU or no ulceration: a retrospective cohort study. Wounds Int. 2018;9(1):11≠17.
20. Zimmerman JE, Kramer AA, Knaus WA. Changes in hospital mortality for United States intensive care unit admissions from 1988 to 2012. Crit Care. 2013;17(2):R81–R89.
21. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel. Pressure Ulcer. Prevention & Treatment: Clinical Practice Guideline. Washington, DC: National Pressure Ulcer Advisory Panel;2009.
22. Ahtiala M, Soppi E, Kivimäki R. Critical evaluation of the Jackson/Cubbin pressure ulcer risk scale — a secondary analysis of a retrospective cohort study population of intensive care patients. Ostomy Wound Manage. 2016;62(2):24–33.
23. Jackson C. The revised Jackson/Cubbin pressure area risk calculator. Intensive Crit Care Nurs. 1999;15(3):169–175.
24. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22(7):707–710.
25. Cox DR. The regression analysis of binary sequences (with discussion). J Royal Stat Soc B. 1958;20(2):215–242.
26. Nelder J, Wedderburn R. Generalized linear models. J Royal Stat Soc A. 1972;135(3):370–384.
27. Berlowitz DR, Brandeis GH, Anderson J, Du W, Brand H. Effect of pressure ulcers on the survival of long-term care residents. J Gerontol A Biol Sci Med Sci. 1997;52(A 2):MI06–M110.
28. European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers/Injuries. Clinical Practice Guideline. The International Guideline. Emily Haesler (Ed.). EPUAP/NPIAP/PPPIA;2019.
29. García-Fernández FP, Soldevilla Agreda JJ, Verdú J, Pancorbo-Hidalgo PL. A new theoretical model for the development of pressure ulcers and other dependence-related lesions. J Nurs Scholarsh. 2014;46(1):28–38.
30. Bly D, Schallom M, Sona C, Klinkenberg D. A model of pressure, oxygenation, and perfusion risk factors for pressure ulcers in the intensive care unit. Am J Crit Care. 2016;25(2):156–164.
31. García-Fernández FP, Pancorbo-Hidalgo PL, Soldevilla Argeda JJ, Rodriguez Torres MC. Risk assessment scales for pressure ulcers in intensive care units: a systematic review with meta-analysis. EWMA J. 2013;13(2):7–13.
32. Ahtiala M, Soppi E, Tallgren M. Specific risk factors for pressure ulcer development in adult intensive care patients – a retrospective cohort study. EWMA J. 2018;19(1):35J–42.
33. Sauaia A, Moore FA, Moore EE. Postinjury inflammation and organ dysfunction. Crit Care Clin. 2017;33(1):167–191.
34. Taylor R, James T. The role of oxidative stress in the development and persistence of pressure ulcers. In: Bader DL, Bouten CV, Colin D, Oomens CW (eds). Pressure Ulcer Research. Current and Future Perspectives. Berlin, Germany: Springer-Verlag Berlin Heidelberg: Springer;2005:205–232.
35. Latifa K, Sondess S, Hajer G, et al. Evaluation of physiological risk factors, oxidant-antioxidant imbalance, proteolytic and genetic variations of matrix metalloproteinase-9 in patients with pressure ulcer. Sci Rep. 2016;6(7):1–11.
36. Santos EM, Farias LC, Santos SHS, de Paula AMB, Oliveira E Silva CS, Guimarães ALS. Molecular finds of pressure ulcer: a bioinformatics approach in pressure ulcer. J Tissue Viability. 2017;26(2):119–124.
37. Gefen A. The future of pressure ulcer prevention is here: detecting and targeting inflammation early. EWMA J. 2018;19(2):7–13.
38. Coslovsky M, Takala J, Exadaktylos AK, Martinolli L, Merz TM. A clinical prediction model to identify patients at high risk of death in the emergency department. Intens Care Med. 2015;41(6):1029–1036.
