


DIAMondback Atherectomy With OCT Visualization for Calcified PAD Lesions (DIAMOCT-PAD Study)
Abstract
Objective. In this study, we aimed to describe the immediate and long-term vascular effects of OAS in patients with peripheral arterial disease (PAD) and moderate to severely calcified lesions. Background. Debulking the calcified atherosclerotic plaque with the orbital atherectomy system (OAS) can potentially enhance vessel compliance and increase the chance of reaching a desirable angioplasty result. Methods. A total of 7 patients were evaluated both at baseline and at 6-month follow-up. Following a diagnostic peripheral angiogram, patients with significant SFA disease had a baseline intravascular optical coherence tomography (IV-OCT) and the lesion was treated with OAS. Repeat IV-OCT was performed after atherectomy and after drug-coated balloon, if used. Patients were also evaluated with angiography and IV-OCT imaging at their 6-month follow-up. Results. The majority of tissue removed was fibrous tissue. During follow-up, luminal volume increased for 4 of the 7 patients from baseline to 6-month follow-up and decreased in 3 patients. On average there was a 6% increase of luminal volume (P<.01 compared with baseline). A recent virtual histology algorithm was used for automatic classification of IV-OCT images unaided by any reader. The algorithm used convolutional neural networks to identify regions as either calcium, fibrous, or lipid plaque, and it agreed with an expert reader 82% of the time. Conclusion. To the best of our knowledge, the current report is the first to describe vascular effects of OAS in medial calcified lesions immediately after and at follow-up using IV-OCT in patients with severe PAD.
J INVASIVE CARDIOL 2022;34(2):E117-E123. Epub 2022 January 20.
Key words: orbital atherectomy, peripheral artery disease, optical coherence tomography, calcification, virtual histology
Introduction
Endovascular therapy is widely used for the treatment of peripheral arterial disease (PAD) and it is rapidly evolving with novel techniques and devices.1 Balloon angioplasty and stenting are frequently used for revascularization; however, their use alone does not remove the atheroma, rather, these procedures redistribute the plaque inside and along the arterial wall at the edges of the stent.2 Consequently, bulky and heavily calcified plaques may not respond well to balloon dilation.3 Moreover, heavily calcified lesions are associated with unfavorable outcomes due to early recoil or flow-limiting dissections.4 Unlike balloon angioplasty, atherectomy modalities allow the removal of calcified atherosclerotic plaque in a more controlled fashion. Therefore, atherectomy may reduce barotrauma to the vessel wall and consequent dissections, while optimizing stent expansion and apposition in patients with PAD and calcified lesions.4 However, Monckeberg medial calcification is a unique type of plaque and how it responds to atherectomy is not known, since the medial calcium is covered by a fibrous tissue coating.
Orbital atherectomy (OA) is a relatively recent atherectomy system, which utilizes an eccentric rotating diamond-coated crown to modify and remove the calcified atherosclerotic plaque with orbital sanding.5 As the softer tissue is deflected away from the crown, the system can preferentially ablate inelastic tissue such as fibrous or calcified plaque.5,6 Debulking the atherosclerotic plaque with OA can potentially enhance vessel compliance, increase the chance of reaching a desirable angioplasty result, and allow better drug delivery to the arterial wall.7-9
Intravascular optical coherence tomography (IV-OCT) is an imaging modality that provides high resolution images and allows tissue characterization.10,11 Detailed endovascular imaging with IV-OCT contributes to the better understanding of the atherosclerotic disease pathophysiology and its response to percutaneous interventions.12 IV-OCT has been utilized in the coronary and the peripheral arterial circulation.12,13 However, although a number of studies have previously investigated the effects of OA in the coronary arteries using IV-OCT,14-18 its effects in the human peripheral circulation have not yet been investigated. Further, using artificial intelligence for the OCT identification of calcium (virtual histology OCT [VH-OCT]) is a new and evolving field that has not has not been previously applied to PAD patients. In this current study, we aimed to describe the immediate and long-term vascular effects of OA at the 6-month follow-up and demonstrate the application of a recent VH-OCT algorithm for calcium, fibrous tissue, and lipid identification.19
Methods
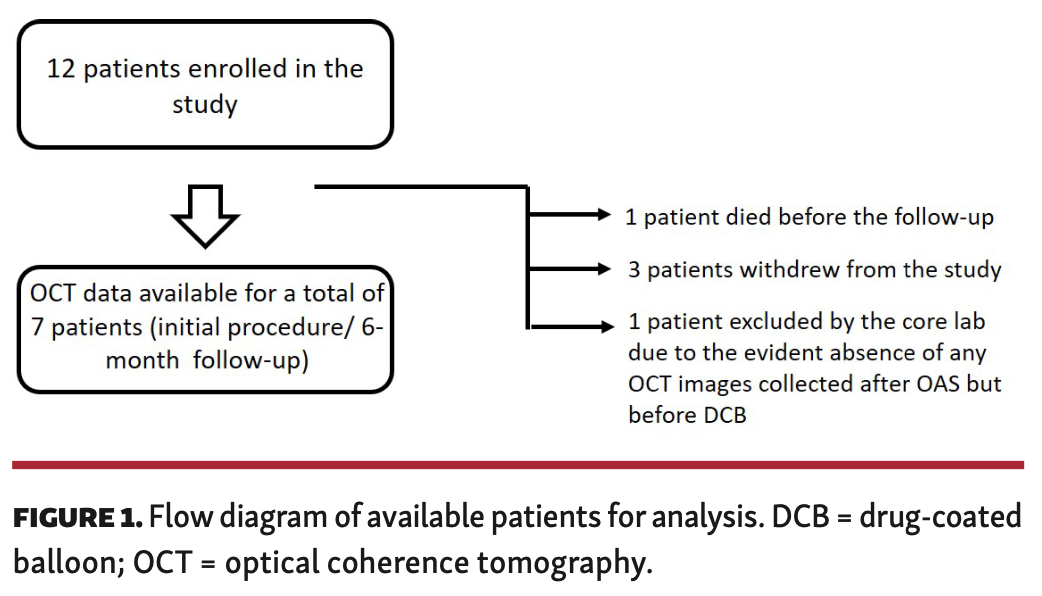
This pilot study was designed as a prospective, nonrandomized, single-arm study using a Diamondback 360 Peripheral Orbital Atherectomy device (Cardiovascular Systems Inc.) in patients with symptomatic PAD with moderate to severely calcified lesions. The study was approved by the institutional review board and a written- consent form was obtained before enrolling the patients in the study. The study was registered on www.clinicaltrials.gov (identification number: 03455374). Patients were evaluated with angiography and IV-OCT imaging both at the initial procedure and 6-month follow-up. The study was terminated after 12 patients due to poor enrollment. A flow diagram of the available patients for analysis can be seen in Figure 1.
Inclusion/exclusion criteria. Inclusion criteria were as follows: (1) Patients with lower-extremity claudication and PAD due to significant superficial femoral artery (SFA) stenosis (50% - ≤99%) that affects the quality of life despite maximum medical therapy and exercise program. (2) Evidence of significant SFA disease involving the most symptomatic limb by noninvasive vascular testing with the use of the following: (ankle-brachial index [ABI]: <.9 [if ABI >1.4, SFA systolic acceleration time should be >140 ms] and/or toe-brachial index: <.6). (3) Computed tomography angiography or magnetic resonance angiography confirming at least a 50% SFA stenosis with moderate-to-severe calcification.
Patients with (1) any planned/scheduled revascularization procedures ≤ 30 days after baseline procedure; (2) prior lower extremity revascularization ≤30 days before baseline procedure; (3) a target in-stent restenosis; (4) infrapopliteal disease involving the last remaining vessel; (5) planned amputation; (6) a creatinine clearance <30 mL/min; (6) known bleeding disorders; (7) known active pathological bleeding; (8) known hypersensitivity to antiplatelets or anticoagulants; (9) known history of intracranial hemorrhage at any time; gastrointestinal bleed in the past 6 months, or major surgery within the past 30 days; (10) known ischemic stroke during the past 3 months; (11) known severe liver disease; or (12) known history of congestive heart failure with left ventricular ejection fraction of <30% were excluded from the study. Patients with concerns about compliance to the medications regimen and/or follow-up (eg, alcohol or drug abuse) and female patients with known pregnancy, breast feeding, or intent to become pregnant during the study period were also excluded from the study.
Interventional procedure. Following a diagnostic peripheral angiography, patients with significant SFA disease (≥ 50%) had baseline IV-OCT imaging of the target vessel and the lesion was treated with proper size crown. Repeat IV-OCT was performed after the atherectomy. Drug-coated balloon (DCB) angioplasty was performed at the discretion of the operator. If a DCB was used, a final IV-OCT imaging was performed to assess lesion expansion and possible dissections.
IV-OCT images were acquired in each subject using commercially available, frequency-domain C7-XR (St. Jude Medical). A 2.7 Fr Dragonfly OCT imaging catheter (St. Jude Medical) was advanced into the distal lumen of the target SFA vessel segment and an automated 20 mm/s, 54 mm diagnostic pullback of the target lesion region was performed, while the blood was cleared with a 40 mL power injection of clearing agent (dextran) at 10 mL/sec via side-arm of sheath. If the target lesion length was >54 mm, we performed multiple, overlapping pullbacks to image the entire target lesion region. The final number of visualized vessel segments in each patient was determined by the investigator as long as the entire target lesion segment was included and at least 5 mm of non-diseased native vessel segment distal and proximal to the target lesion.
All images were de-identified and digitally stored. Processing was performed at the OCT core laboratory located at the University of Texas Health–San Antonio with a unique software for quantitative OCT image analysis using both attenuation coefficient and texture analysis for the identification of calcium. VH-OCT accuracy was determined as the % agreement between the VH-OCT algorithm and the expert OCT reader when identifying tissue as either calcium or non-calcified plaque.
Pre- and postatherectomy OCT luminal gain and removal of the calcium from the vessel wall was the primary imaging endpoint. Secondary endpoints for the initial procedure included change in calcified plaque volume, change in total plaque volume, number, and percentage of frames with new dissections, percentage of cross-sectional images with new injury to the adventitia, or external elastic lamina. Luminal area loss, change in calcified and total plaque volume, and percentage of cross-sectional images with persistent dissections were compared between the post-atherectomy and 6-month OCT pullbacks.
VH-OCT for calcium detection.19 Internal review board approval was obtained from University of Texas Health Science Center in San Antonio from which in vivo data was collected. Ex vivo human coronary arteries were collected from donors in San Antonio whose hearts were not suitable for transplantation. Coronary arteries were first dissected from the heart and then attached to a custom fixture that allowed perfusion with saline while imaging with IV-OCT. IV-OCT imaging was performed using an assortment of Dragonfly OPTIS and Dragonfly Duo imaging catheters. The arteries were then sent for histological processing at the Texas Heart Institute, where they were stained with H&E every 400 µm and Movat’s pentachrome every 2 mm. An expert IV-OCT reader worked with a cardiovascular pathologist to coregister the histology and IV-OCT images. The expert IV-OCT reader then manually segmented images into congruent, color-coded class maps based on tissue type. Classmap generated masks were dilated to help ensure that edges would be identified. The in vivo classmaps were likewise generated by an expert IV-OCT reader. Due to their clinical importance, calcium, fibrous tissue, and lipids were selected for CNN identification.
Inclusion of ex vivo IV-OCT data sets provide an advantage of accurate characterization via histology, coupled with the downside of possible registration errors and microstructural changes due to autolysis. In vivo IV-OCT data lack histological accuracy but train the CNN with more realistic data recorded from live coronary arteries. For these reasons, both CNNs were trained and tested on both ex vivo and in vivo IV-OCT data sources. The final dataset was composed of 38 ex vivo and 6 in vivo IV-OCT pullbacks. From the set of ex vivo frames coregistered with histology, 410 frames were randomly selected, and 87 in vivo frames with classmaps were selected. IV-OCT data were further split into training and testing datasets.
Ex vivo and in vivo IV-OCT pullbacks were recorded using St. Jude Ilumien systems giving 16-bit tiff images that represent linear intensity data after the OCT signal processing. The pullbacks varied slightly in width and height proportions, but all were first resized to 256 × 512 pixels. The data were then padded on the left and the right, each by 32 A-scans from opposing sides of the frame to prevent the CNN from having issues with boundary A-scans. These data were normalized by dividing by 2 16−1, producing B-scans α1 • In in the range of 0 to 1. The attenuation data do not take into account the optical properties of the system, thus representing a relative measure of attenuation rather than an absolute measure. The algorithm for generating attenuation data has the side effect of producing increased values at extreme depths, often overwhelming the native signal where tissue is present. Two methods were employed to accommodate this effect: padding the bottom of the image and creating a third B-scan that merges the intensity and attenuation images. The IV-OCT images were padded on the bottom by taking the bottom-most 128 pixels and performing a mirroring and appending operation. Next the attenuation data are computed, producing B-scan α2 • Ia, also in the range of 0 to 1. Constants α1 = 2 and α2 = 1 are used to scale B-scan contributions to the network and were determined experimentally. A third B-scan was computed:
[Ina = (α1 • In) 2 + (α2 • Ia)2] square root
The 3 B-scans merged along the channel dimension served as inputs into the CNN. The network training was terminated when the moving average of the error stopped improving over 10 runs.
Software, hardware, and CNN. The CNN employed here was a U-Net constructed using Deep Learning for Java, an open source, scalable, mature deep learning framework that can run either on a CPU or Nvidia GPU. The U-Net follows the work done by Ronneberger et al,20 though each layer was scaled down by a factor of 8. This scaling was permissible since the goal was to detect calcium only —so reducing number of neurons was deemed acceptable. The CNNs were trained with an Adam algorithm with a learning rate of 2 × 10−4 with a cross entropy loss function.21 Due to the larger image size of 320×640, a smaller batch size of 8 was used. The computer used was an Alienware Aurora R7 with 16 GB of RAM and dual Nvidia GTX 1080 GPUs, each with 8 GB of RAM.
Statistical analysis. All parameters were expressed as mean ± standard deviation or percentages. Wilcoxon signed-rank test was used to analyze the luminal change over time. The sample size was chosen without a power calculation because the study was designed as a pilot study. Data were analyzed using SPSS, version 21 (SPSS).
Results
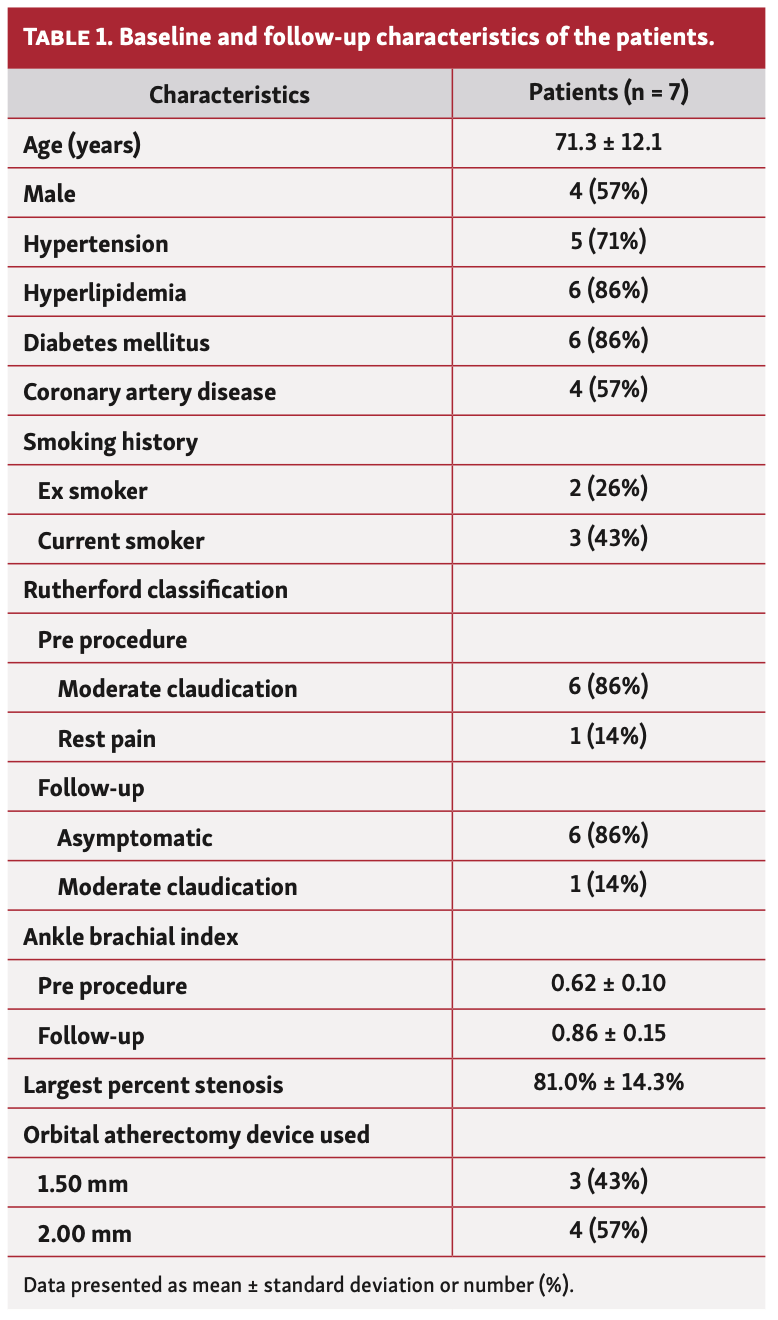
A total of 7 patients were included in the study. Mean age of the study participants was 71.3 ± 12.1 and 4 (57%) patients were male. Five (71%) patients had hypertension, 6 (86%) had hyperlipidemia, 6 (86%) had diabetes mellitus, and 4 (57%) had a history of coronary artery disease. Most patients (86%) had Rutherford class 3 claudication, while 1 patient presented with rest pain. Baseline characteristics of the patients can be found in Table 1. All interventions were performed in the SFA.
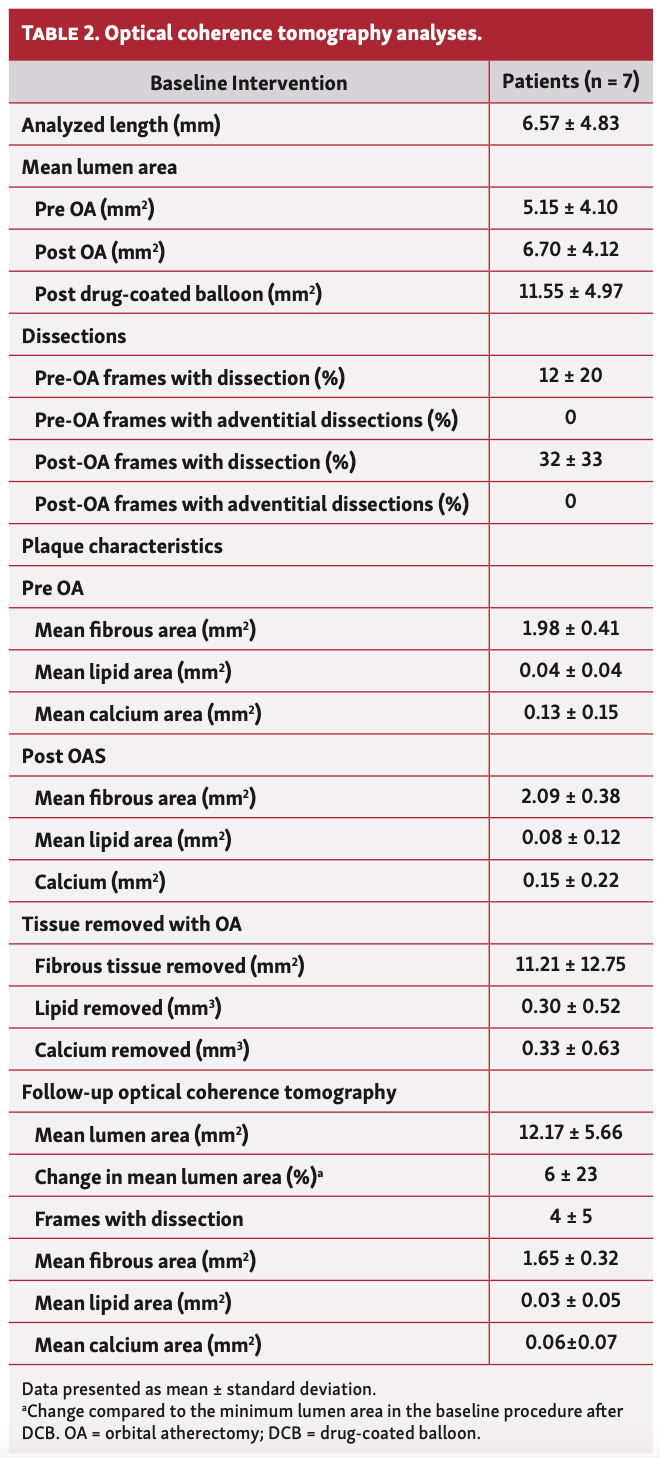
Atherosclerotic plaque and fibrous tissue were successfully removed by the orbital atherectomy in all but 1 patient (Figure 2). Luminal volume increased for 4 of the 7 patients in the region of interest from baseline (after DCB) to follow-up and decreased in 3 patients (Figure 3). On average there was a 6% increase of luminal volume (P<.01, compared with baseline).
When the plaque characteristics were evaluated, most of the tissue removed from these patients was fibrous tissue (mean fibrous tissue removed 11.21 ± 12.75 mm3, mean lipid removed 0.30 ± 0.52 mm3, mean calcium removed 0.33± 0.63 mm3).
After OA, dissections were observed in a mean of 48% of the frames; however, at follow-up most of these dissections were healed and were present in 34% of the frames. None of the dissections were penetrating into the adventitia after OA.
A VH algorithm developed by our group for automatic classification of OCT images unaided by any reader was utilized. The algorithm used convolutional neural networks to identify regions as either calcium o, fibrous or lipid, and it agreed with the expert reader 82% of the time (Figure 4 and Table 2).
Discussion
To the best of our knowledge, the current study is the first to describe imaging outcomes immediately after orbital atherectomy and at follow-up using IV and VH-OCT in PAD patients with moderate to severely calcified lesions. Another unique aspect of the study is the use of a VH algorithm for plaque characterization of OCT. The main findings of the study are as follows: (1) The mean luminal volume increased on average by 6% in the follow-up. When the patients were evaluated individually, luminal area increased in 4 of the 7 patients, while decreasing in 3 patients in the region of interest from baseline to the follow-up. (2) New dissections were initially observed after orbital atherectomy, but most improved during follow-up and none penetrated into the adventitia; (3) Most of the tissue removed by atherectomy was fibrous; (4) The VH algorithm was trained to identify pixels as calcium, fibrous or lipid, and it agreed with the expert reader 82% of the time.
PAD has emerged as a global health problem, affecting more than 200 million people worldwide.22 An “endovascular first” approach has been embraced for the majority of patients requiring revascularization.23 Despite the advances in device technology and increased operator experience, heavily calcified lesions remain challenging and limit both procedural and long-term success. The use of atherectomy modalities to debulk the calcified atherosclerotic plaques prior to angioplasty can improve procedural and long-term outcomes by improving vessel compliance, rate of dissections, drug delivery and consequently the need for bail-out stenting.4,9,24 Avoiding stents or the “leaving no metal behind” approach may also improve long-term outcomes.4 Plaque characterization using intravascular imaging can further refine this strategy.
The primary aim of OA is to modify the lesion compliance rather than the luminal gain with maximum debulking.25,26 During the rotation of the crown, the softer healthy tissue is deflected away from the crown, and the system can preferentially ablate inelastic plaque.5,6 In the TRUTH study, the VH-IVUS revealed that OA modified the calcified component of the plaque burden, which may change the lesion compliance allowing for low pressure adjunctive balloon angioplasty.26 However, in our study, most of the removed tissue was fibrous. This is probably related to the deep location of the calcifications. It is also important to note that, there may be pulsatile forces that indirectly cause fragmentation of deeper calcification in the arterial wall.5 In the study of Yamamoto et al, the differential plaque modification was imperfect with OA in coronary arteries and there was evidence of noncalcified plaque modification.16 These authors suggested that noncalcified plaques may be prone to the effects of guidewire bias, forcing the crown to remove fibrous and elastic tissue. There are also concerns that the non-calcified tissue ablation can lead to vascular perforations; nevertheless, there were no perforations in our study.16
During the percutaneous interventions, barotrauma and mechanical stretch may lead to dissections in the vessel wall.27 In a previous study, Fujihara et al reported 84% of the SFA cases had varying degrees of dissections after balloon angioplasty, 42% being severe.28 Over the long-term, those dissections can result in unfavorable outcomes.27,28 Atherectomy per se can cause dissections. In fact, Kini et al using IV-OCT after atherectomy showed tissue modification with deep dissections in approximately a third of the treated lesions after rotational atherectomy and OA in coronary arteries. Moreover, post-OA dissections were significantly deeper in these lesions.14 On the contrary in peripheral interventions, atherectomy can reduce the rate of significant dissections and therefore, the need for bailout stenting.8,29 In our study, despite the higher number of image frames by OCT after OA, none of the dissections were flow limiting and there were no adventitial dissections. It is important to note that IV-OCT provides an approximate 10-fold higher resolution than IVUS (10–15 µm compared to 100–150 µm) and it may describe microperforations which would not be recognized by angiography and IVUS, without its use. The clinical importance of those micro-perforations to the primary patency of the vessel after percutaneous interventions remains to be determined. Moreover, fewer dissections were present at 6 months follow-up with IV-OCT, which indicates that most of them heal without adverse consequences.
Various automated plaque-classification approaches have been developed to make IV-OCT image interpretation more reliable and rapid. However, these approaches are limited by a lack of comparison to histology, are not developed using clinically standard IV-OCT devices, require a user to select regions of interest, and lack sensitivity for differentiating lipidic from calcific plaque.30-33 The aim of our work was to develop a fully automated and histology-validated plaque classification artificial intelligence that can segment IV-OCT images into 3 vascular components: fibrous, lipid, and calcium. We will demonstrate that neural networks trained on attenuation, structural, and textural features with histology as ground truth can accurately segment IV-OCT images and classify them into appropriate plaque morphologies compared to an expert OCT reader and apply the use of VH-OCT to the peripheral circulation for the first time.
Study limitations. There are certain limitations of the current study. First, the sample size was small, which also limits the statistical analyses. However, this study was designed as a pilot study. Further, having access to IV-OCT imaging in these patients at 6 months mitigates this concern. The lack of a comparison group that did not have rotational atherectomy or alternative peripheral devices is another limitation. The presence of a single expert OCT reader to compare the results of the VH-OCT is another limitation. However, the single reader (TH) ran the OCT core lab for 8 years, and has significant experience. Finally, it should be noted that due to the limited penetration depth of IV-OCT, deeper tissue might have become visible and identifiable both to the expert reader and the VH-OCT algorithm after atherectomy had removed superficial tissue.
Conclusion
In this study, we described imaging outcomes immediately after orbital atherectomy and at follow-up using IV- and VH-OCT in PAD patients with moderate to severely calcified lesions.
Affiliations and Disclosures
From the 1UTHSCSA, San Antonio, Texas; 2UT Houston, MD Anderson Cancer Center, Houston, Texas; 3Department of Cardiology, Pamukkale University Hospitals, Denizli, Turkey; 4UT Austin, School of Biomedical Engineering, Austin, Texas; 5Arkansas Heart Hospital, Little Rock, Arkansas; and 6HCA Northside Hospital, St. Petersburg, Florida.
Funding: This study was an investigator initiated study funded by CSI.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Manuscript accepted May 10, 2021.
The authors report patient consent for images used herein.
Address for correspondence: Mehmet Cilingiroglu, MD, Professor of Medicine and Biomedical Engineering, UTHSCSA, 11800 Carmel Creek Road, San Diego, CA 92130. Email: cilingiroglumehmet@gmail.com
Related Articles
- Histopathologic Characterization of Chronic Total Occlusions by Directional Atherectomy: The HIPACT Study
- Intravascular Ultrasound Insights Into Perforation After Coronary Atherectomy
- Accidental Stent Withdrawal Through an Entrapped Rotational Atherectomy Burr
- Peripheral Arterial Vessel Prepping with Intravascular Ultrasound and Atherectomy: An Interventionalist’s Perspective
References
1. Al-Omran M, Tu JV, Johnston KW, Mamdani MM, Kucey DS. Use of interventional procedures for peripheral arterial occlusive disease in Ontario between 1991 and 1998: a population-based study. J Vasc Surg. 2003;38(2):289-295.
2. Katsanos K, Spiliopoulos S, Reppas L, Karnabatidis D. Debulking atherectomy in the peripheral arteries: is there a role and what is the evidence? Cardiovasc Intervent Radiol. 2017;40(7):964-977.
3. Pietzsch JB, Geisler BP, Ikeno F. Cost-effectiveness of orbital atherectomy compared to rotational atherectomy in treating patients with severely calcified coronary artery lesions in Japan. Cardiovasc Interv Ther. 2018;33(4):328-336.
4. Korosoglou G, Giusca S, Andrassy M, Lichtenberg M. The role of atherectomy in peripheral artery disease: current evidence and future perspectives. Vasc Endovasc Rev. 2019;2(1):12-18.
5. Shlofmitz E, Martinsen BJ, Lee M, et al. Orbital atherectomy for the treatment of severely calcified coronary lesions: evidence, technique, and best practices. Expert Rev Med Devices. 2017;14(11):867-879.
6. Saab F, Martinsen BJ, Wrede D, Behrens A, Adams GL, Mustapha J. Orbital atherectomy for calcified femoropopliteal lesions: a current review. J Cardiovasc Surg (Torino). 2019;60(2):212-220.
7. Zheng Y, Belmont B, Shih AJ. Experimental investigation of the abrasive crown dynamics in orbital atherectomy. Med Eng Phys. 2016;38(7):639-647.
8. Shammas NW, Lam R, Mustapha J, et al. Comparison of orbital atherectomy plus balloon angioplasty vs. balloon angioplasty alone in patients with critical limb ischemia: results of the CALCIUM 360 randomized pilot trial. J Endovasc Ther. 2012;19(4):480-488.
9. Tzafriri AR, Garcia-Polite F, Zani B, et al. Calcified plaque modification alters local drug delivery in the treatment of peripheral atherosclerosis. J Control Release. 2017;264:203-210. Epub 2017 Sep 1.
10. Cilingiroglu M, Oh JH, Sugunan B, et al. Detection of vulnerable plaque in a murine model of atherosclerosis with optical coherence tomography. Catheter Cardiovasc Interv. 2006;67(6):915-923.
11. Tearney GJ, Regar E, Akasaka T, et al. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: a report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J Am Coll Cardiol. 2012;59(12):1058-1072.
12. Marmagkiolis K, Lendel V, Leesar MA, Feldman MD, Cilingiroglu M. Use of optical coherence tomography during superficial femoral artery interventions. J Invasive Cardiol. 2014;26(5):220-223.
13. Marmagkiolis K, Lendel V, Cawich I, Leesar M, Feldman MD, Cilingiroglu M. Optical coherence tomography to guide below-the-knee endovascular interventions. Int J Cardiol. 2014;176(3):1336-1338.
14. Kini AS, Vengrenyuk Y, Pena J, et al. Optical coherence tomography assessment of the mechanistic effects of rotational and orbital atherectomy in severely calcified coronary lesions. Catheter Cardiovasc Interv. 2015;86(6):1024-1032.
15. Sotomi Y, Cavalcante R, Shlofmitz RA, et al. Quantification by optical coherence tomography imaging of the ablation volume obtained with the orbital atherectomy system in calcified coronary lesions. EuroIntervention. 2016;12(9):1126-1134.
16. Yamamoto MH, Maehara A, Kim SS, et al. Effect of orbital atherectomy in calcified coronary artery lesions as assessed by optical coherence tomography. Catheter Cardiovasc Interv. 2019;93(7):1211-1218.
17. Okamoto N, Ueda H, Bhatheja S, et al. Procedural and one-year outcomes of patients treated with orbital and rotational atherectomy with mechanistic insights from optical coherence tomography. EuroIntervention. 2019;14(17):1760-1767.
18. Yamamoto MH, Maehara A, Karimi Galougahi K, et al. Mechanisms of orbital versus rotational atherectomy plaque modification in severely calcified lesions assessed by optical coherence tomography. JACC Cardiovasc Interv. 2017;10(24):2584-2586.
19. Baruah V, Zahedivash A, Hoyt T, et al. Automated coronary plaque characterization with Intravascular optical coherence tomography and smart-algorithm approach: virtual histology OCT. JACC Cardiovasc Imaging. 2020;13(8):1848-1850.
20. Ronneberger O, Fischer P, Brox T. 2015. U-Net: convolutional networks for biomedical image segmentation. In: Navab N, Hornegger J, Wells W, Frangi A (eds). Medical Image Computing and Computer-Assisted Intervention – MICCAI 2015. MICCAI 2015. Lecture Notes in Computer Science, vol 9351. Springer. 2015:234-241.
21. Kingma DP, Ba J. Adam: a method for stochastic optimization. arXiv:14126980 [cs.LG]. Updated January 30, 2017. Accessed January 11, 2022. https://arxiv.org/abs/1412.6980
22. Song P, Rudan D, Zhu Y, et al. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: an updated systematic review and analysis. Lancet Glob Health. 2019;7(8):e1020-e1030.
23. Olin JW, White CJ, Armstrong EJ, Kadian-Dodov D, Hiatt WR. Peripheral artery disease: evolving role of exercise, medical therapy, and endovascular options. J Am Coll Cardiol. 2016;67(11):1338-1357.
24. Tellez A, Dattilo R, Mustapha JA, et al. Biological effect of orbital atherectomy and adjunctive paclitaxel-coated balloon therapy on vascular healing and drug retention: early experimental insights into the familial hypercholesterolaemic swine model of femoral artery stenosis. EuroIntervention. 2014;10(8):1002-1008.
25. Das T, Mustapha J, Indes J, Vorhies R, Beasley R, Doshi N, Adams GL. Technique optimization of orbital atherectomy in calcified peripheral lesions of the lower extremities: the CONFIRM series, a prospective multicenter registry. Catheter Cardiovasc Interv. 2014;83(1):115-122.
26. Babaev A, Zavlunova S, Attubato MJ, Martinsen BJ, Mintz GS, Maehara A. Orbital atherectomy plaque modification assessment of the femoropopliteal artery via intravascular ultrasound (TRUTH study). Vasc Endovascular Surg. 2015;49(7):188-194.
27. Gray WA, Cardenas JA, Brodmann M, et al. Treating post-angioplasty dissection in the femoropopliteal arteries using the Tack Endovascular System: 12-month results from the TOBA II Study. JACC Cardiovasc Interv. 2019;12(23):2375-2384.
28. Fujihara M, Takahara M, Sasaki S, et al. Angiographic dissection patterns and patency outcomes after balloon angioplasty for superficial femoral artery disease. J Endovasc Ther. 2017;24(3):367-375.
29. Kim T-H, Katsetos M, Dahal K, Azrin M, Lee J. Use of rotational atherectomy for reducing significant dissection in treating de novo femoropopliteal steno-occlusive disease after balloon angioplasty. J Geriatr Cardiol. 2018;15(4):254-260.
30. Athanasiou LS, Bourantas CV, Rigas G, et al. Methodology for fully automated segmentation and plaque characterization in intracoronary optical coherence tomography images. J Biomed Opt. 2014;19(2):026009.
31. Rico-Jimenez JJ, Campos-Delgado DU, Villiger M, Otsuka K, Bouma BE, Jo JA. Automatic classification of atherosclerotic plaques imaged with intravascular OCT. Biomed Opt Express. 2016;7(10):4069-4085.
32. Ughi GJ, Adriaenssens T, Sinnaeve P, Desmet W, D’hooge J. Automated tissue characterization of in vivo atherosclerotic plaques by intravascular optical coherence tomography images. Biomed Opt Express. 2013;4(7):1014-1030.
33. He S, Zheng J, Maehara A, et al. Convolutional neural network based automatic plaque characterization for intracoronary optical coherence tomography images. In: Angelini ED, Angelini ED, Landman BA (eds). Medical Imaging 2018: Image Processing. Vol. 10574. Progress in Biomedical Optics and Imaging – Proceedings of SPIE.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
