


External Validation of the JR-CTO Score in Retrograde Chronic Total Occlusion Intervention: From the PROGRESS-CTO Registry
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
In complex chronic total occlusion (CTO) percutaneous coronary interventions (PCI), a retrograde crossing strategy is often necessary. Recently, the Japanese retrograde (JR) CTO score was developed using a simple 4-item tool. This score showed good performance in predicting guidewire crossing failure in patients undergoing primary retrograde CTO PCI. We evaluated the JR-CTO score’s performance in patients treated at 44 centers between 2013 and 2024 as part of the Prospective Global Registry for the Study of CTO Intervention (PROGRESS-CTO). In this independent cohort, although the JR-CTO score showed an association with crossing and technical failure, its predictive ability for both outcomes was modest.
Introduction
Retrograde crossing is often needed in complex chronic total occlusion (CTO) percutaneous coronary interventions (PCI) but has been associated with higher rates of procedural complications as compared with the antegrade approach.1 The Japanese retrograde (JR) CTO score was recently developed by using a simple 4-item tool with a good performance in predicting guidewire crossing failure in patients undergoing primary retrograde CTO PCI.2 We performed an external validation of the JR-CTO score in an independent cohort.
Methods
The Prospective Global Registry for the Study of Chronic Total Occlusion Intervention (PROGRESS-CTO; NCT02061436), is a prospective, observational, multicenter study enrolling CTO PCIs at 44 national and international centers. We analyzed data from 16 028 CTO PCIs performed between 2012 and 2024. The study was approved by the institutional review board of each center and informed consent was waived.
The JR-CTO score was calculated for all primary retrograde cases (ie, when the retrograde strategy was the first crossing strategy performed in the CTO PCI procedure), and patient characteristics were summarized. JR-CTO scores were used to predict guidewire crossing failure, crossing time, and technical failure, defined as successful CTO recanalization with achievement of less than 30% residual stenosis and thrombolysis in myocardial infarction (TIMI)-3 flow.
The Pearson’s chi-square test was used to compare categorical variables. Continuous variables were presented as mean ± SD or as median (interquartile range) and compared using the independent-samples t-test for normally distributed variables and the Mann-Whitney U test for non-parametric variables. We performed univariable logistic regression to assess the association of the JR-CTO score with crossing failure. The discriminative capacity of the score was assessed using the area under the curve (AUC) of the receiver-operating characteristic (ROC) curve. Crossing times were analyzed using box plots according to the JR-CTO score. R Statistical Software, version 4.3.3 (R Foundation for Statistical Computing) was used for statistical analysis and a P-value of less than 0.05 was classified as statistically significant.
Results
Of 1269 primary retrograde CTO PCI cases, successful crossing was achieved in 1011 (81.6%) patients, whereas 228 (18.4%) had crossing failure. Patients with crossing failure had higher rates of prior PCI, moderate to severe calcification, and proximal cap ambiguity, and were less likely to have interventional collaterals.
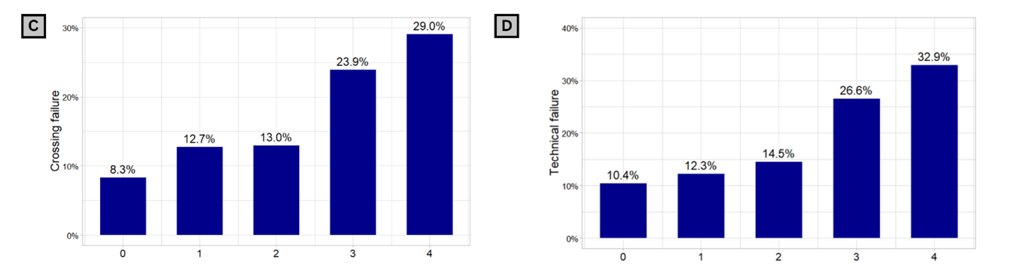
In our cohort, 3.8% of the patients had a JR-CTO score of 0, 16.7% had a JR-CTO score of 1, 34.7% had a JR-CTO score of 2, 32.6% a JR-CTO score of 3, and 12.2% had a JR-CTO score of 4 (Figure 1A). Higher JR-CTO scores were associated with longer crossing times as the JR-CTO score increased (Figure 1B). Crossing failure occurred in 8.3% in patients with a JR-CTO score of 0, 12.7% in patients with a JR-CTO score of 1, 13.0% in patients with a JR-CTO score of 2, 23.9% in patients with a JR-CTO score of 3, and 29.0% in patients with a JR-CTO score of 4 (Figure 1C). The AUC of the JR-CTO prediction model for crossing failure was 0.62 (95% CI, 0.58-0.65) (Figure 1D). Similar results were found when we used the JR-CTO prediction model for technical failure (AUC 0.63; 95% CI, 0.59-0.66; Figure 1E and F).


Discussion
In our study, higher JR-CTO scores were associated with higher crossing and technical failures, as well as with longer crossing time. The capacity of the JR-CTO in predicting crossing failure was modest (AUC 0.63) compared with the study by Tanaka et al (AUC 0.72).2 The incidence of crossing failure in the study from Tanaka et al was lower, probably due to differences in the study populations. Patients from the Japanese CTO-PCI registry had lower JR-CTO scores, with 61.8% of the patients having a JR-CTO score of 0 or 1. In our study, only 20.5% of patients had a JR-CTO score of 0 to 1, whereas most patients had a JR-CTO of 2 or 3 (34.7% and 32.6%, respectively).
Retrograde CTO PCI should be performed if the anticipated benefits outweigh the risks. Retrograde CTO PCI has increased risk of complications as compared with the antegrade approach but is also associated with higher success rates, especially in more complex CTOs.3 The use of scores such as the JR-CTO score could help with patient and physician decision-making; for example, if the anticipated likelihood of success is low and the risk high, retrograde CTO PCI may be best avoided, except in highly symptomatic patients.4-6 Predicting the likelihood of antegrade wiring success could be very useful in such patients and could be facilitated by the use of machine learning algorithms.7
Limitations
Our study has limitations. The PROGRESS-CTO is an observational registry with all inherent limitations and includes different patients than those in the JR-CTO score derivation cohort. There was no independent adjudication of clinical events or core laboratory analysis of the study’s angiograms. The procedural data and baseline characteristics needed to calculate the JR-CTO score were available for 843 (66.4%) patients, and those with missing data were excluded from the validation analysis. The PROGRESS-CTO includes experienced operators in CTO PCI, hence, the results may not apply to less experienced operators and centers.
Conclusions
In conclusion, while there is an association between crossing failure and JR-CTO score, its predictive ability for both crossing and technical failures was modest, suggesting a need for new such tools.
Affiliations and Disclosures
Pedro E. P. Carvalho, MD; Athanasios Rempakos, MD; Deniz Mutlu, MD;Michaella Alexandrou, MD; Dimitrios Strepkos, MD; Bavana V. Rangan, BDS, MPH; Olga C. Mastrodemos, BA; Ahmed Al-Ogaili, MD; M. Nicholas Burke, MD; Yader Sandoval, MD; Emmanouil S. Brilakis, MD, PhD
From theMinneapolis Heart Institute and Minneapolis Heart Institute Foundation, Abbott Northwestern Hospital, Minneapolis, Minnesota, USA.
Disclosures: Dr Sandoval serves on advisory boards for Abbott Diagnostics, Roche Diagnostics, Philips, GE, and Zoll; is a speaker for Roche Diagnostics and Philips; holds patent 20210401347; and is an associate editor for JACC Advances. Dr Brilakis receives consulting/speaker honoraria from Abbott Vascular, the American Heart Association (associate editor, Circulation), Biotronik, Boston Scientific, Cardiovascular Innovations Foundation (Board of Directors), CSI, Elsevier, GE Healthcare, IMDS, Medtronic, and Teleflex; receives research support from Boston Scientific, GE Healthcare; is the owner of Hippocrates LLC; and is a shareholder in MHI Ventures, Cleerly Health, and Stallion Medical. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Center for Complex Coronary Interventions, Minneapolis Heart Institute, Center for Coronary Artery Disease at the Minneapolis Heart Institute Foundation, 920 E 28th Street #300, Minneapolis, MN 55407, USA. Email: esbrilakis@gmail.com; X: esbrilakis
References
- Allana SS, Kostantinis S, Rempakos A, et al. The retrograde approach to chronic total occlusion percutaneous coronary interventions: technical analysis and procedural outcomes. JACC Cardiovasc Interv. 2023;16(22):2748-2762. doi:10.1016/j.jcin.2023.08.031
- Tanaka H, Tsuchikane E, Kishi K, et al. Retrograde coronary chronic total occlusion intervention (JR-CTO) score: from the Japanese CTO-PCI expert registry. JACC Cardiovasc Interv. 2024;17(11):1374-1384. doi:10.1016/j.jcin.2024.03.023
- Tajti P, Karmpaliotis D, Alaswad K, et al. The hybrid approach to chronic total occlusion percutaneous coronary intervention: update from the PROGRESS CTO registry. JACC Cardiovasc Interv. 2018;11(14):1325-1335. doi:10.1016/j.jcin.2018.02.036
- Simsek B, Rempakos A, Kostantinis S, et al. A systematic review of periprocedural risk prediction scores in chronic total occlusion percutaneous coronary intervention. Am J Cardiol. 2023;193:118-125. doi:10.1016/j.amjcard.2023.01.044
- Rempakos A, Simsek B, Kostantinis S, et al. Assessment of the ERCTO Score for predicting success in retrograde chronic total occlusion percutaneous coronary interventions in the PROGRESS-CTO registry. J Invasive Cardiol. 2023;35(6):E294-E296. doi:10.25270/jic/23.00036
- Mutlu D, Rempakos A, Alexandrou M, et al. Validation of the J-Channel Score for retrograde channel crossing in the PROGRESS-CTO registry. J Invasive Cardiol. 2024;36(5). doi:10.25270/jic/24.00006
- Rempakos A, Alexandrou M, Mutlu D, et al. Predicting successful chronic total occlusion crossing with primary antegrade wiring using machine learning. JACC Cardiovasc Interv. 2024;17(14):1707-1716. doi:10.1016/j.jcin.2024.04.043



