

In Vivo Virtual Histology Intravascular Ultrasound Comparison of Neointimal Hyperplasia Within Drug-Eluting- Versus Bare Metal Stents
ABSTRACT: Background. The process of in-stent neointimal hyperplasia (NIH) between drug-eluting stents (DES) and bare metal stents (BMS) might be different. We compared in vivo composition of in-stent NIH between DES and BMS using virtual histology-intravascular ultrasound (VH-IVUS). Methods and Results. Volumetric VH-IVUS was used to compare in-stent NIH between 23 DES and 15 BMS in 30 patients who underwent coronary angiography because of angina. The inner and outer VH-IVUS contours were drawn in a way to avoid the stent strut artifacts. Cross-sectional analysis was done at every VH-IVUS frame within the stent, thereby allowing volumetric measurement of stent, lumen, and NIH and its components. Baseline characteristics and IVUS measurements were similar between DES and BMS groups. The duration of follow-up was similar between DES (median 38 months [interquartile range, 7–59]) vs. BMS (median 40 months [interquartile range, 7–99]), (p=0.26). % necrotic core (NC) volume was significantly higher in DES than BMS: 19.5 [16.3, 25.6] vs. 12.1 [8.2, 18.5] (p=0.006). %NC volume significantly increased with time in BMS (p=0.007), but not in DES (p=0.24) so that at any given time point, %NC in DES was greater than in BMS. After adjustment for baseline differences, only DES (p=0.003) and stent age (p=0.043) were independent predictors of %NC volume. VH-IVUS in-stent thin-cap fibroatheromas were detected only in the DES group: 34.8% vs. 0%, p=0.013. Conclusion. In vivo composition of in-stent NIH between DES and BMS was different, suggesting that the process of in-stent NIH in DES and BMS is diverse.
J INVASIVE CARDIOL 2011;23:262–268
Key words: in-stent restenosis, stent thrombosis, VH-IVUS
_____________________________________________
Drug-eluting stents (DES), as compared to bare metal stents, reduce restenosis by inhibiting neointimal hyperplasia (NIH).1,2 Stent thrombosis, however, has emerged as a major concern.3,4 The phenomenon of very late stent thrombosis is more frequent in DES than in bare metal stents (BMS),5 although the mechanisms remain unclear. NIH after BMS implantation consists of vascular smooth muscle cells and an extracelluar matrix, including proteoglycans, hyaluronan, and collagen I and III;6 but little is known about the histological composition of NIH within DES. In an angioscopic study, Higo et al7 reported that newly formed neointima within DES contains yellow atherosclerotic plaque in 30% of lesions. Yellow plaque formation is also present in the vessel wall underneath the struts of DES. It is plausible that differences in plaque composition within DES compared to BMS may contribute to the more frequent late thrombotic events seen with DES.5 Virtual histology-intravascular ultrasound (VH-IVUS) was developed to improve on the limited ability of conventional grayscale IVUS to assess plaque composition, although VH-IVUS has not been validated in a study of NIH. Nevertheless, in the present study we used VH-IVUS to assess differences in the composition of NIH within DES compared with BMS.
Methods
Patients. From June to December 2009, we identified 107 patients who underwent coronary angiography with VH-IVUS coronary assessment at Washington Hospital Center. The indication of VH-IVUS was left at the discretion of the operators. Among them, 46 patients had VH-IVUS assessment of a previously implanted stent (either BMS or DES). All patients had stable angina pectoris. Sixteen of 46 patients were excluded because of manual IVUS catheter pullback, pre-dilation before VH-IVUS, in-stent restenosis secondary to stent underexpansion, or in-stent restenosis in a vein graft. Overlapped stents were treated as 1 long stent resulting in a total study population of 38 stents in 30 patients ― 23 DES and 15 BMS; 2 patients treated with both DES and BMS in different lesions were included in both groups. All stents had been implanted in de novo native coronary lesions between 1997 and August 2009. Five patients who underwent percutaneous coronary intervention prior to January 2003 were treated with BMS because DES have only been available since April 2003 in the United States. After April, 2003, 17 patients were treated with DES, 6 patients were treated with BMS, and 2 patients were treated with both stent types. Post-stent implantation aspirin 325 mg/day was prescribed lifelong; and clopidogrel 75 mg/day or ticlopidine 200 mg/day was prescribed for ≥ 12 months in the DES group and ≥ 1 month in the BMS group.
Patient hospital records were reviewed to obtain information on clinical demographic data and medical history. Systemic hypertension included ≥ 1 of the following: antihypertensive medication use, systolic blood pressure ≥ 140 mmHg, or diastolic blood pressure ≥ 90 mmHg. Dyslipidemia included ≥ 1 of the following: treatment with medication, total cholesterol ≥ 220 mg/dL, low-density lipoprotein cholesterol ≥ 140 mg/dL, high-density lipoprotein cholesterol < 40 mg/dL, or triglycerides ≥ 150 mg/dL. Diabetes mellitus included ≥ 1 of the following: oral agent or insulin treatment or hemoglobin A1c > 6.5%. This study was performed with the approval of the institutional review board. All patients gave written informed consent before the procedures.
VH-IVUS. After coronary angiography, VH-IVUS examinations were performed after intracoronary artery administration of 200 µg nitroglycerin with a commercially available VH-IVUS system (Volcano Therapeutics, Inc., Rancho Cordova, California) that uses spectral analysis of radiofrequency ultrasound signals to enable assessment of plaque composition with established accuracy.8,9 Image acquisition used automated transducer pullback at 1.0 mm/s performed from a point at least 10 mm distal to the stent to the aorto-ostial junction. Quantitative IVUS measurements and VH-IVUS analysis were performed using the Volcano VH-IVUS machine (Version 3.1) by individuals blinded to stent type and age (time from implantation to VH-IVUS analysis). Cross-sectional analysis was done at every VH-IVUS frame within the stent, thereby allowing volumetric measurement of stent, lumen, and NIH and its components. The grayscale IVUS analyses were performed according to the American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies.10
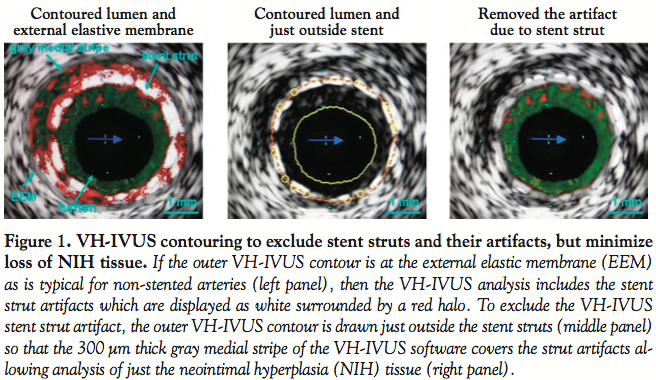 We have previously reported that on VH-IVUS most stent struts (80%) appeared white (misclassified as “calcium”) surrounded by red (misclassified as “necrotic core”); 2% appeared just white; and 17% were not detectable.11 Importantly, we decided that it was necessary to exclude these stent strut artifacts from the current analysis; otherwise, the amount of calcium and, especially, the amount of necrotic core (NC) would reflect the artifacts and not the composition of the neointima. Therefore, the outer VH-IVUS contour was drawn to take advantage of the software-imposed gray medial stripe; this medial stripe is 300 μm in thickness and is not included in VH-IVUS analysis. The outer contour was drawn so that the gray medial stripe covered entirely the stent struts and their VH-IVUS artifacts, thus excluding them from the NIH compositional analysis (Figure 1). The inner VH-IVUS contour was at the lumen interface. NIH was classified into fibrotic tissue, fibro-fatty plaque, dense calcium, and NC, and presented as % of NIH area or volume. In-stent fibroatheroma was defined as NIH >40% of stent area and NC >20% of NIH area. In-stent thin-cap fibroatheroma was defined as NIH >40% of stent area, NC >20% of NIH area, and NC in contact with the lumen in ≥ 2 consecutive frames.
We have previously reported that on VH-IVUS most stent struts (80%) appeared white (misclassified as “calcium”) surrounded by red (misclassified as “necrotic core”); 2% appeared just white; and 17% were not detectable.11 Importantly, we decided that it was necessary to exclude these stent strut artifacts from the current analysis; otherwise, the amount of calcium and, especially, the amount of necrotic core (NC) would reflect the artifacts and not the composition of the neointima. Therefore, the outer VH-IVUS contour was drawn to take advantage of the software-imposed gray medial stripe; this medial stripe is 300 μm in thickness and is not included in VH-IVUS analysis. The outer contour was drawn so that the gray medial stripe covered entirely the stent struts and their VH-IVUS artifacts, thus excluding them from the NIH compositional analysis (Figure 1). The inner VH-IVUS contour was at the lumen interface. NIH was classified into fibrotic tissue, fibro-fatty plaque, dense calcium, and NC, and presented as % of NIH area or volume. In-stent fibroatheroma was defined as NIH >40% of stent area and NC >20% of NIH area. In-stent thin-cap fibroatheroma was defined as NIH >40% of stent area, NC >20% of NIH area, and NC in contact with the lumen in ≥ 2 consecutive frames.
 Statistical analysis. Statistical analysis was performed with SAS version 9.1 (SAS Institute, Cary, North Carolina). Comparison of continuous variables was performed with non parametric Mann Whitney U test. Values were presented as median, interquartile range. Categorical variables were analyzed with Fisher’s exact test or chi square test as appropriate. Spearman bivariate correlation analysis was performed between time and % NIH volume or between % NIH and % NC area. Multivariable linear regression analysis was used to determine the predictors of % NC volume. Variables associated with p < 0.20 in Spearman bivariate correlation analysis were included in the regression model. Variables tested were DES, patient age, sex, diabetes mellitus, systemic hypertension, dyslipidemia, smoking, stent age, clinical indication for stent implantation at the index procedure (acute coronary syndrome - Y/N), lesion location, malapposition, stent overlap, and medication before admission (aspirin, clopidogrel, ß-blocker, angiotensin-converting enzyme inhibitor/angiotensin II antagonist, calcium-channel blocker, statin, and insulin). Statistical significance was defined as a two-sided p value < 0.05. The authors had full access to and take full responsibility for the integrity of the data. All authors have read and agree to the manuscript as written.
Statistical analysis. Statistical analysis was performed with SAS version 9.1 (SAS Institute, Cary, North Carolina). Comparison of continuous variables was performed with non parametric Mann Whitney U test. Values were presented as median, interquartile range. Categorical variables were analyzed with Fisher’s exact test or chi square test as appropriate. Spearman bivariate correlation analysis was performed between time and % NIH volume or between % NIH and % NC area. Multivariable linear regression analysis was used to determine the predictors of % NC volume. Variables associated with p < 0.20 in Spearman bivariate correlation analysis were included in the regression model. Variables tested were DES, patient age, sex, diabetes mellitus, systemic hypertension, dyslipidemia, smoking, stent age, clinical indication for stent implantation at the index procedure (acute coronary syndrome - Y/N), lesion location, malapposition, stent overlap, and medication before admission (aspirin, clopidogrel, ß-blocker, angiotensin-converting enzyme inhibitor/angiotensin II antagonist, calcium-channel blocker, statin, and insulin). Statistical significance was defined as a two-sided p value < 0.05. The authors had full access to and take full responsibility for the integrity of the data. All authors have read and agree to the manuscript as written.
Results
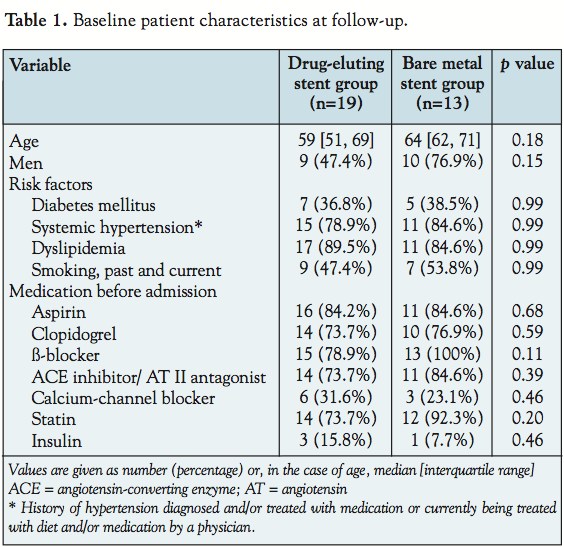
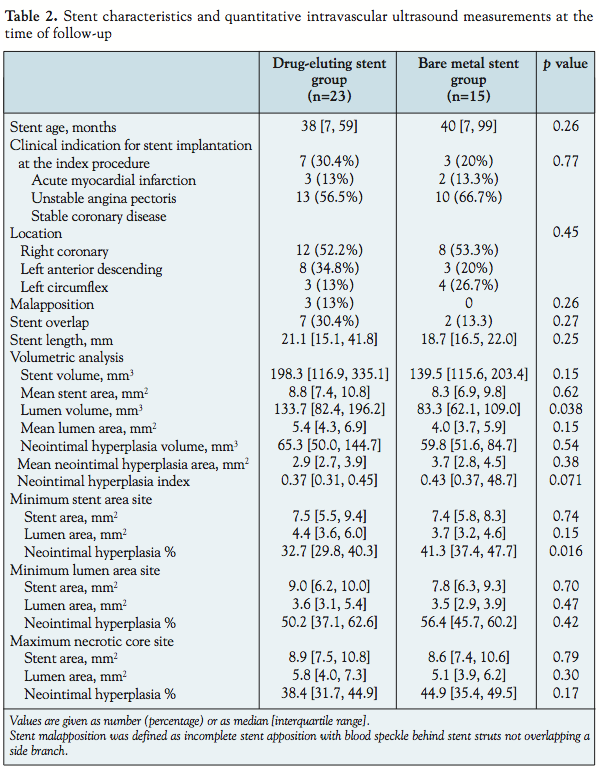 Baseline characteristics. Coronary risk factors were similar in both groups, (Table 1) including clinical indication for percutaneous coronary intervention at the time of the index procedure (Table 2). There was no difference in stent age between DES (median 38 [interquartile range, 7–59], minimum 3, maximum 66 months) vs. BMS (median 40 [interquartile range, 7–99], minimum 3, maximum 144 months), (p = 0.26). There was no difference in medication usage before admission between the 2 groups. Statins were used in 75% of DES-treated patients and in 90% of BMS-treated patients.
Baseline characteristics. Coronary risk factors were similar in both groups, (Table 1) including clinical indication for percutaneous coronary intervention at the time of the index procedure (Table 2). There was no difference in stent age between DES (median 38 [interquartile range, 7–59], minimum 3, maximum 66 months) vs. BMS (median 40 [interquartile range, 7–99], minimum 3, maximum 144 months), (p = 0.26). There was no difference in medication usage before admission between the 2 groups. Statins were used in 75% of DES-treated patients and in 90% of BMS-treated patients.
 Grayscale IVUS measurements. As shown in Table 2 and when normalized for stent length, mean stent area, mean lumen area, and mean NIH area were similar comparing DES versus BMS, although neointimal volume index (%NIH volume) tended to be smaller in the DES group as compared to the BMS group (0.37 [0.31, 0.45] vs. 0.43 [0.37, 48.7], respectively, p = 0.071). At the minimum stent area site, %NIH was less in the DES group than in the BMS group (p=0.016).
Grayscale IVUS measurements. As shown in Table 2 and when normalized for stent length, mean stent area, mean lumen area, and mean NIH area were similar comparing DES versus BMS, although neointimal volume index (%NIH volume) tended to be smaller in the DES group as compared to the BMS group (0.37 [0.31, 0.45] vs. 0.43 [0.37, 48.7], respectively, p = 0.071). At the minimum stent area site, %NIH was less in the DES group than in the BMS group (p=0.016).
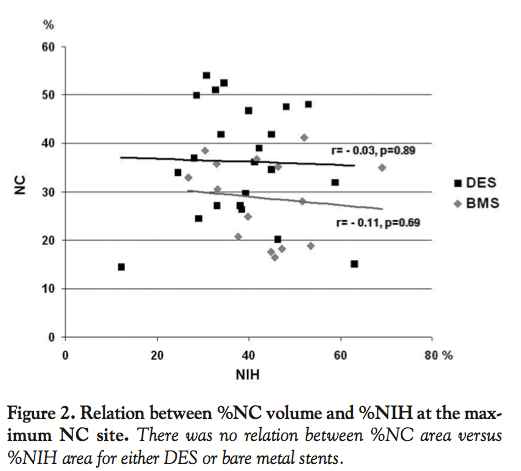 VH-IVUS findings. In early stage BMS (≤ 12 months, n = 7), most of the NIH was detected as fibrous or fibro-fatty, 90 ± 3.2%. Overall %necrotic core (NC) volume was significantly higher in DES than BMS: 19.5 [16.3, 25.6] vs. 12.1 [8.2, 18.5] (p = 0.006). There was no difference of VH-IVUS findings between overlapped and non-overlapped DES sites (Table 3). There was no relation between % NC versus the amount of NIH at the maximum NC site in DES or BMS (Figure 2).
VH-IVUS findings. In early stage BMS (≤ 12 months, n = 7), most of the NIH was detected as fibrous or fibro-fatty, 90 ± 3.2%. Overall %necrotic core (NC) volume was significantly higher in DES than BMS: 19.5 [16.3, 25.6] vs. 12.1 [8.2, 18.5] (p = 0.006). There was no difference of VH-IVUS findings between overlapped and non-overlapped DES sites (Table 3). There was no relation between % NC versus the amount of NIH at the maximum NC site in DES or BMS (Figure 2).
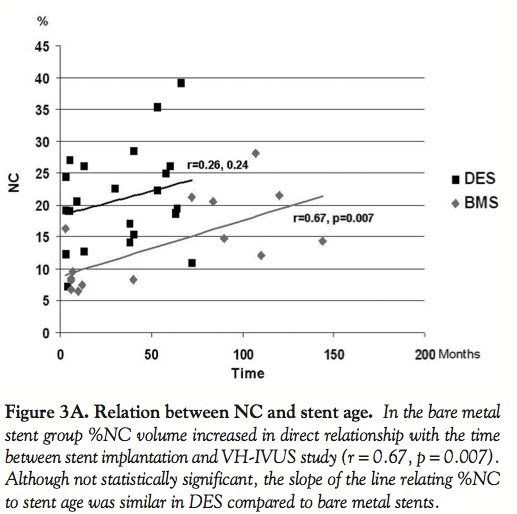 In BMS, %NC volume significantly increased with time (r = 0.67, p = 0.007, Figure 3A). Although the slope of the line relating %NC volume to stent age was similar between DES and BMS, there was not a similar statistically significant relationship between %NC volume and stent age in the DES group, possibly because there were fewer old DES than old BMS (r = 0.26, p = 0.24). At any giving time point, the %NC in DES was higher than in BMS. Figure 3B shows the relation between % dense calcium volume and stent age; dense calcium significantly increased with time in DES (r=0.42, p=0.049), and marginally increased in BMS (r=0.48, p=0.074).
In BMS, %NC volume significantly increased with time (r = 0.67, p = 0.007, Figure 3A). Although the slope of the line relating %NC volume to stent age was similar between DES and BMS, there was not a similar statistically significant relationship between %NC volume and stent age in the DES group, possibly because there were fewer old DES than old BMS (r = 0.26, p = 0.24). At any giving time point, the %NC in DES was higher than in BMS. Figure 3B shows the relation between % dense calcium volume and stent age; dense calcium significantly increased with time in DES (r=0.42, p=0.049), and marginally increased in BMS (r=0.48, p=0.074).
 Variables with a p value < 0.2 on univariable analysis ―DES, stent age, dyslipidemia and clinical indication for stent implantation at the index procedure (acute coronary syndrome - Y/N)― were entered into a multivariable linear regression model to adjust for baseline differences. Independent predictors of % NC volume were DES (p = 0.003) and stent age (p= 0.043).
Variables with a p value < 0.2 on univariable analysis ―DES, stent age, dyslipidemia and clinical indication for stent implantation at the index procedure (acute coronary syndrome - Y/N)― were entered into a multivariable linear regression model to adjust for baseline differences. Independent predictors of % NC volume were DES (p = 0.003) and stent age (p= 0.043).
There were 9 VH-IVUS in-stent fibroatheroma in the DES group compared to 5 in the BMS group (p=1.0). There were 8 VH-IVUS in-stent thin-cap fibroatheroma in the DES group compared to 0 in the BMS group (p = 0.013). The incidence of VH-IVUS in-stent thin-cap fibroatheroma was 28.6% (< 1 year), 66.7% (1–3 yrs), 37.5% (1–5 yrs), 20.0% (> 5 yrs) respectively. Examples are shown in Figure 4. The borderline in-stent thin-cap fibroatheroma (NC in contact with the lumen and satisfied 2 of the following criteria; NIH > 40% of stent area, NC > 20% of NIH area and present in ≥ 2 consecutive frames) was observed in 4 DES and 4 BMS (p = 0.4).
the BMS group (p=1.0). There were 8 VH-IVUS in-stent thin-cap fibroatheroma in the DES group compared to 0 in the BMS group (p = 0.013). The incidence of VH-IVUS in-stent thin-cap fibroatheroma was 28.6% (< 1 year), 66.7% (1–3 yrs), 37.5% (1–5 yrs), 20.0% (> 5 yrs) respectively. Examples are shown in Figure 4. The borderline in-stent thin-cap fibroatheroma (NC in contact with the lumen and satisfied 2 of the following criteria; NIH > 40% of stent area, NC > 20% of NIH area and present in ≥ 2 consecutive frames) was observed in 4 DES and 4 BMS (p = 0.4).
 Treatment after coronary angiography and IVUS. After coronary angiography and IVUS, percutaneous coronary intervention was performed in 27 of 30 patients. Optimal medical therapy without percutaneous coronary intervention was selected for 3 patients. Target lesion revascularization was performed in 25 stents: DES 15 (65.2%) and BMS 10 (66.7%), p = 0.99. Target vessel revascularization was performed in 34 stents: DES 21 (91.3%) and BMS 13 (86.7%), p = 0.99.
Treatment after coronary angiography and IVUS. After coronary angiography and IVUS, percutaneous coronary intervention was performed in 27 of 30 patients. Optimal medical therapy without percutaneous coronary intervention was selected for 3 patients. Target lesion revascularization was performed in 25 stents: DES 15 (65.2%) and BMS 10 (66.7%), p = 0.99. Target vessel revascularization was performed in 34 stents: DES 21 (91.3%) and BMS 13 (86.7%), p = 0.99.
Discussion
The data herein reported are the first to our knowledge demonstrating consistent differences between the VH-IVUS appearance of in-stent NIH comparing DES versus BMS, with more NC in DES as well as in older BMS. While the frequency of VH-IVUS in-stent fibroatheroma was similar between DES and BMS, VH-IVUS in-stent thin-cap fibroatheroma was observed only in the DES group. The incidence of VH-IVUS thick-cap fibroatheroma within stent was similar between DES and BMS groups. In early stage BMS (≤ 12 months), most of the NIH was detected as fibrous or fibro-fatty. This indicates that VH-IVUS recognizes smooth muscle cells and extracellular matrix as fibrous or fibro-fatty tissue (green or green yellow). Small NC or dense calcium present in the early stage BMS could be original atherosclerotic tissue that may be protruding through the stent struts.
Neointimal coverage of BMS is nearly complete by 3 to 6 months.12 Angiographic regression of in-stent luminal narrowing occurs from 6 months to 3 years post-BMS implantation. Conversely, tissue within DES is characterized by a lack of smooth muscle cells, fibrin deposition, and incomplete endothelialization.13 Coronary artery vessel walls are normally protected from lipid transport across the vessel wall by maintaining an efficient endothelial barrier. Plaque progression is initiated by endothelial dysfunction or damage that allows increased permeability of lipoproteins and upregulation of adhesion molecules.14 The anti-proliferative effect of drugs such as sirolimus and paclitaxel is not limited to smooth muscle cells. They also prevent re-growth of endothelial cells; leaving stent struts uncovered by either smooth muscle cells or endothelial cells, allowing accelerated infiltration of lipids and monocytes and hastening the process of atherosclerosis.15 It is possible that underlying atherosclerotic lesions progress even more rapidly after DES implantation than do native coronary plaques with eventual luminal thrombosis. The inflammation by DES also may have resulted in the increase of % dense calcium (Figure 3B). Conversely, the neointima in BMS is made up of smooth muscle cells and extracellular matrix6 that may act as a shield to prevent invasion of macrophages that results in neoatherosclerosis.
In autopsy cases Nakazawa et al.15 reported that the incidence of atherosclerotic change (NIH with foamy macrophage infiltration) was seen in only 10% of BMS lesions (8 of 77) compared with 35% in DES lesions (23 of 66; p < 0.0004). There was a significant difference in the timing of atherosclerotic change; the earliest atherosclerotic changes in DES were observed at 4 months after stent implantation. In contrast, atherosclerotic changes occurred beyond 2 years in BMS, remaining a rare finding until 4 years. The earliest NC formation in DES was observed at 9 months compared with 5 years in BMS. In an optical coherence tomography study, Takano at al indicated that lipid-laden intima and neovascularization were more frequent in BMS ≥ 5 years old compared with BMS < 6 months old.16 These findings are very similar to the results of our in vivo study. NC increased with time in BMS; however, more NC was present from the early phase in DES (Figure 3A). Thus, the mechanism of restenosis in DES may include more newly formed atherosclerosis and less vascular smooth muscle cells and accumulation of extracelluar matrix components compared with BMS.
The neointima in BMS typically imparts a white hue on angioscopic examination. Conversely, Higo et al7 found yellow-colored, newly-formed neointima over DES struts; even among lesions that did not have a yellow hue at baseline, yellow-colored, newly-formed neointima was detected in 95% of lesions at follow-up. It is conceivable that the presence of an intense yellow hue in stented segments represents an atherosclerotic plaque that may be prone to rupture and may contribute to the frequency of late stent thrombosis, which is akin to vulnerable plaques in non-stented arteries.15 On the other hand, yellow neointima was never observed in BMS within 12 months of implantation.7
In-stent thin-cap fibroatheroma and late stent thrombosis. Several studies have shown that delayed arterial healing and stent malapposition may be important causes of very late stent thrombosis after DES placement.12,13,17–19 Angioscopy studies have demonstrated that up to 20% of DES struts are uncovered at 2 years.20 However, the reported rate of very late stent thrombosis is not that high, suggesting that other factors may be important in the pathophysiology of stent thrombosis. Lee et al21 reported that in-stent neointimal rupture was observed in 43.5% of DES patients with very late stent thrombosis. Overall, very late stent thrombosis occurred at a mean of 50.8 ± 36.2 months after the index procedure, and occurred sooner after DES implantation than BMS implantation (33.2 ± 12.5 vs. 108.4 ± 26.5 months, p < 0.001), which is consistent with the longer time needed to develop intra-stent neoatherosclerotic plaque and plaque rupture. Plaque rupture due to rapidly formed in-stent neoatherosclerosis might play a more important role in the pathophysiology of very late stent thrombosis in DES than was previously thought; and may be the reason why very late stent thrombosis is very rare in BMS compared with DES.5 In the present study NC was observed earlier in DES than in BMS. Furthermore, in the time frame we measured, 8 VH-IVUS in-stent thin-cap fibroatheroma were observed only in DES while all of the VH-IVUS in-stent fibroatheroma in BMS were covered with a thick fibrous cap. It is plausible that % necrotic core increase and VH-IVUS in-stent thin-cap fibroatheroma may be associated with in-stent neointimal rupture resulting in stent thrombosis.
Methodologic considerations. The assessment of plaque composition after stent implantation by VH-IVUS has the problem of stent strut artifact.11 VH-IVUS classified plaque between inner and outer contours. If the outer VH-IVUS contour is drawn at the external elastic membrane and the inner contour is drawn at the lumen, the plaque area between the inner and outer contour would include all of the stent struts (as well as the persistent plaque and NIH) whose artifacts increase the % dense calcium and NC (Figure 1). On the other hand, if the outer VH-IVUS contour is drawn within the stent struts to exclude the stent strut artifact, then a significant amount of NIH would be lost because it would be “covered” by the 300 µm thick, software-imposed gray medial stripe. Therefore, we hit on the novel approach to use the 300 µm thick, software-imposed gray medial stripe to our advantage by drawing the outer contour so that the gray medial stripe covered the stent strut artifacts, but not the NIH. Thus, this method for assessment of NIH within stent struts removes the strut artifact completely while minimizing loss of NIH. This is shown in Figure 1.
Study limitations. First, this study was a single-center, nonrandomized, retrospective study with a small sample size. Second, IVUS and, in particular, VH-IVUS was not available from the initial stent implantation procedure; it is possible that plaque morphology of the original lesion may also influence the composition of the NIH in the long term. Third, choice of BMS versus DES and the use of VH-IVUS were at the operator’s discretion, which may have introduced bias into patient selection for this study. Fourth, in removing the VH-IVUS artifacts of the stent struts, we lost a very small amount of NIH just inside the struts. Fifth, VH-IVUS is not validated for NIH; however, the accuracy of VH-IVUS assessment of plaque composition in de novo lesions is well established. This study confirmed that VH-IVUS recognizes smooth muscle cells and extracellular matrix as fibrous or fibro-fatty tissue (green or green yellow). Further, the findings of NIH and time course of NC in the present study correspond to previous pathological, optical coherence tomography, and angioscopic studies, thereby supporting the validity of the current findings.
Conclusion
This in vivo VH-IVUS study demonstrates that the composition of NIH within DES is different from BMS, suggesting that the process of in-stent NIH in DES and BMS is diverse.
References
- Morice MC, Serruys PW, Sousa JE, et al; RAVEL Study Group. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346:1773–1780.
- Moses JW, Leon MB, Popma JJ, et al; SIRIUS Investigators. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349:1315–1323.
- Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005;293:2126–2130.
- Pfisterer M, Brunner-La Rocca HP, Buser PT, et al; BASKET-LATE Investigators. Late clinical events after clopidogrel discontinuation may limit the benefit of drug-eluting stents: An observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol 2006;48:2584–2591.
- Jensen LO, Maeng M, Kaltoft A, et al. Stent thrombosis, myocardial infarction, and death after drug-eluting and bare-metal stent coronary interventions. J Am Coll Cardiol 2007;50:463–470.
- Farb A, Kolodgie FD, Hwang JY, et al. Extracellular matrix changes in stented human coronary arteries. Circulation 2004;110:940–947.
- Higo T, Ueda Y, Oyabu J, et al. Atherosclerotic and thrombogenic neointima formed over sirolimus drug-eluting stent: An angioscopic study. JACC: Cardiovasc Imaging 2009;2:616–624.
- Nasu K, Tsuchikane E, Katoh O, et al. Accuracy of in vivo coronary plaque morphology assessment: A validation study of in vivo virtual histology compared with in vitro histopathology. J Am Coll Cardiol 2006;47:2405–2412.
- Nair A, Kuban BD, Tuzcu EM, et al. Coronary plaque classification with intravascular ultrasound radiofrequency data analysis. Circulation 2002;106:2200–2206.
- Mintz GS, Nissen SE, Anderson WD, et al. American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies (IVUS). A report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol 2001;37:1478–1492.
- Kim SW, Mintz GS, Hong YJ, et al. The virtual histology intravascular ultrasound appearance of newly placed drug-eluting stents. Am J Cardiol 2008;102:1182–1186.
- Finn AV, Nakazawa G, Joner M, et al. Vascular responses to drug eluting stents: Importance of delayed healing. Arterioscler Thromb Vasc Biol 2007;27:1500–1510.
- Joner M, Finn AV, Farb A, et al. Pathology of drug-eluting stents in humans: Delayed healing and late thrombotic risk. J Am Coll Cardiol 2006;48:193–202.
- Traub O, Berk BC. Laminar shear stress: Mechanisms by which endothelial cells transduce an atheroprotective force. Arterioscler Thromb Vasc Biol 1998;18:677–685.
- Nakazawa G, Vorpahl M, Finn AV, Narula J, et al. One step forward and two steps back with drug-eluting-stents: From preventing restenosis to causing late thrombosis and nouveau atherosclerosis. JACC: Cardiovasc Imaging 2009;2:625–628.
- Takano M, Yamamoto M, Inami S, et al. Appearance of lipid-laden intima and neovascularization after implantation of bare-metal stents extended late-phase observation by intracoronary optical coherence tomography. J Am Coll Cardiol 2009;55:26–32.
- Cook S, Wenaweser P, Togni M, et al. Incomplete stent apposition and very late stent thrombosis after drug-eluting stent implantation. Circulation 2007;115:2426–2434.
- Hassan AK, Bergheanu SC, Stijnen T, et al. Late stent malapposition risk is higher after drug-eluting stent compared with bare-metal stent implantation and associates with late stent thrombosis. Eur Heart J 2010;31:1172–1180.
- Maehara A, Mintz GS, Lansky AJ, et al. Volumetric intravascular ultrasound analysis of Paclitaxel-eluting and bare metal stents in acute myocardial infarction: The harmonizing outcomes with revascularization and stents in acute myocardial infarction intravascular ultrasound substudy. Circulation 2009;120:1875–1882.
- Takano M, Yamamoto M, Xie Y, et al. Serial long-term evaluation of neointimal stent coverage and thrombus after sirolimus-eluting stent implantation by use of coronary angioscopy. Heart 2007;93:1533–1536.
- Lee CW, Kang SJ, Park DW, et al. Intravascular ultrasound findings in patients with very late stent thrombosis after either drug-eluting or bare-metal stent implantation. J Am Coll Cardiol 2010;55:1936–1942.
_____________________________________________
From the Washington Hospital Center, Division of Cardiology, Washington, DC and the †Cardiovascular Research Foundation, New York, New York.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 18, 2011, provisional acceptance given April 18, 2011, final version accepted May 4, 2011.
Address for correspondence: Dr. Ron Waksman, Washington Hospital Center, Division of Cardiology, 110 Irving St., NW, Suite 4B-1, Washington, DC 20010. Email: ron.waksman@medstar.net

