

A Very Unusual Origin of Left Subclavian Artery
ABSTRACT: The left internal mammary artery, a branch of the left subclavian artery, is the most commonly used arterial graft during coronary artery bypass grafting. Although extremely rare, an abnormal origin of left subclavian artery may lead to a difficult coronary angiography procedure or result in a catastrophic complication if iatrogenically occluded during a stent-graft repair of thoracic aneurysm. We present a case of an unusual anomalous origin of the left subclavian artery, which was discovered during a diagnostic coronary angiography.
J INVASIVE CARDIOL 2012;24(5):E104-E105
Key words: coronary angiography; aortic arch anomalies; coronary artery bypass grafting
____________________________________________
 Case report. A 62-year-old male with a medical history of ischemic heart disease and coronary artery bypass grafting in 2003, and a redo bypass graft in 2006, admitted to our center with progressive angina and orthopnea. After the clinical evaluation, coronary angiography was performed and revealed that saphenous vein bypass grafts to both circumflex and right coronary arteries were completely occluded at proximal anastomosis. Native circumflex and right coronary arteries were demonstrated through passive retrograde filling from the left anterior descending artery (LAD).
Case report. A 62-year-old male with a medical history of ischemic heart disease and coronary artery bypass grafting in 2003, and a redo bypass graft in 2006, admitted to our center with progressive angina and orthopnea. After the clinical evaluation, coronary angiography was performed and revealed that saphenous vein bypass grafts to both circumflex and right coronary arteries were completely occluded at proximal anastomosis. Native circumflex and right coronary arteries were demonstrated through passive retrograde filling from the left anterior descending artery (LAD).
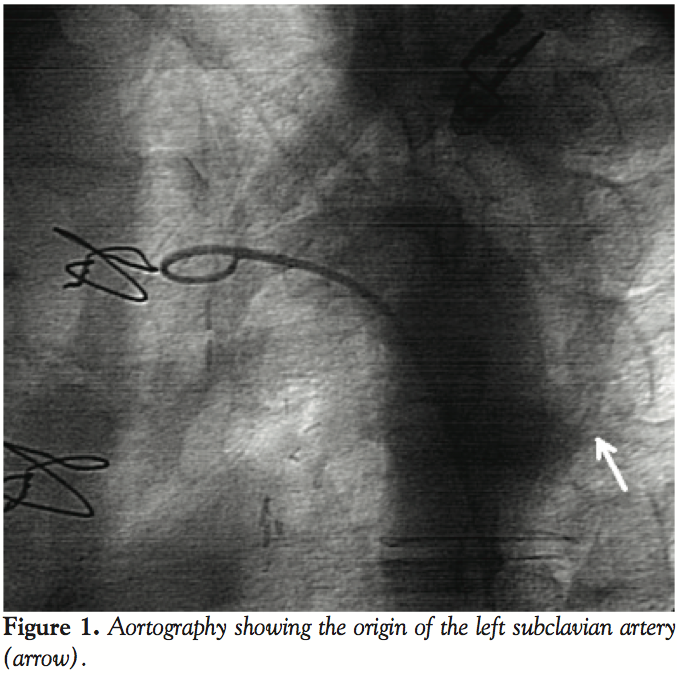
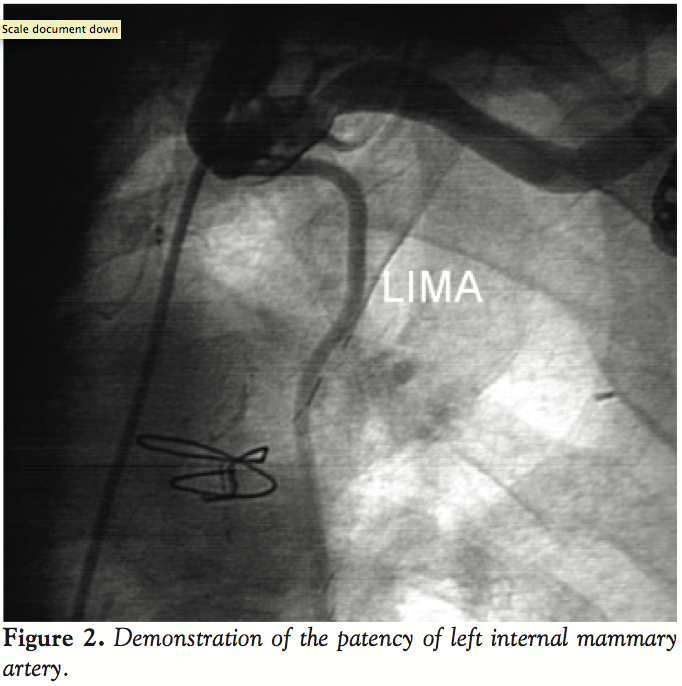 However, many attempts to visualize the bypass grafting of the left internal mammary artery (LIMA) to the LAD failed as the left subclavian artery could not be engaged at aortic arch. After an aortography, we found that the ostium took its origin 5 cm below its presumed position (Figure 1). Thereafter, the left subclavian artery was successfully engaged with a Judkins right 4 catheter and the LIMA was selectively cannulated to check distal patency (Figure 2). Percutaneous interventions for significant occlusions in the left circumflex and right coronary arteries were successfully performed without any complication. No other congenital anomaly was detected in the patient. He was discharged uneventfully on post-admission day 4.
However, many attempts to visualize the bypass grafting of the left internal mammary artery (LIMA) to the LAD failed as the left subclavian artery could not be engaged at aortic arch. After an aortography, we found that the ostium took its origin 5 cm below its presumed position (Figure 1). Thereafter, the left subclavian artery was successfully engaged with a Judkins right 4 catheter and the LIMA was selectively cannulated to check distal patency (Figure 2). Percutaneous interventions for significant occlusions in the left circumflex and right coronary arteries were successfully performed without any complication. No other congenital anomaly was detected in the patient. He was discharged uneventfully on post-admission day 4.
Discussion. A wide range of aortic arch anomalies, primarily based upon single case studies have been described with an incidence of 1%-3% of congenital heart disease patients.1 The clinical picture extends beyond life-threatening aortic vascular rings compressing trachea to asymptomatic cases identified on imaging techniques indicated for unrelated reasons. Patients diagnosed with anomalies involving aortic arch frequently have a microdeletion on chromosome 22. Microdeletion of chr22q11.2 is seen in 1 in 6000 births and 81% of cases are associated with cardiac abnormalities.2 The most common anomalies seen with microdeletion of chr22q11.2 are Tetralogy of Fallot, truncus arteriosus, and interrupted aortic arch. Anomalies of lateralization of aortic arch and subclavian arteries also occur more frequently in relation with this deletion.3 It is known that in patients with conotruncal malformations, anomalies of the subclavian arteries are the most important anatomical marker for the presence of monosomy 22q11.2, independent of the laterality of the aortic arch.4
The origin of right subclavian artery is embryologically derived from fourth aortic arch while the left subclavian artery does not have embryological relations to aortic arches but is derived from the seventh intersegmental artery. As the development proceeds, the seventh intersegmental artery turning out to be the left subclavian artery moves cranially and comes close to the left common carotid artery. Because of its developmentally different origin, the reported cases of anomalies are very rare compared to the right subclavian artery.5
Anomalies of subclavian arteries, which have been defined to date, are accompanied by aortic arch anomalies and other congenital heart diseases or present as single cases. Left subclavian artery anomalies are extremely rare but they have been known to accompany in cases of an anomalous right aortic arch. Right aortic arch anomalies may be accompanied by a retroesophageal left subclavian artery or with both left descending aorta and anomalous origin of left subclavian artery.6 Subclavian arteries may have aberrant origins with or without having a relation to diverticulum of Kommerell.7 Isolation of subclavian artery defined as loss of connection with aorta, and congenital or acquired aneurysm of intrathoracic subclavian arteries are also defined as extremely rare case reports.8-10
An anomalous left subclavian artery originating from the distal descending aorta is an extremely rare type of malformation that has not been reported before in a patient who had otherwise normal anatomy. It is most probably due to interrupted movement of the seventh intersegmental artery cranially during embryogenesis rather than anomalous aortic arch development. To our knowledge, there has been no report about interruption of the differential growth process of left subclavian artery, which normally shifts its origin cranially.
Clinical importance of this unusual origin can be related to the LIMA. Visualization of graft patency during coronary angiography could be a challenge because of unusual origin. Another clinical issue is stent-graft repairs of thoracic aorta. It may be beneficial to properly identify its origin before the procedure, as stent-grafting of thoracic aorta carries the potential risk for iatrogenic occlusion. Physical examination and conventional imaging techniques such as chest x-ray or barium esophagography may not expose any finding for an anomalous origin. Therefore, MRI or multislice computerized tomography constitutes the non-invasive diagnostic strategy while aortography is an invasive option.
References
- Powell AJ, Mandell VS. Vascular rings and slings. In: Nadas' Pediatric Cardiology. 2nd ed. Philadelphia: Saunders Elsevier; 2006:811.
- Botto LD, May K, Fernhoff PM, et al. A population-based study of the 22q11.2 deletion: phenotype, incidence, and contribution to major birth defects in the population. Pediatrics. 2003;112(1 Pt 1):101-107.
- McElhinney DB, Clark BJ 3rd, Weinberg PM, et al. Association of chromosome 22q11 deletion with isolated anomalies of aortic arch laterality and branching. J Am Coll Cardiol. 2001;37(8):2114-2119.
- Rauch R, Rauch A, Koch A, et al. Laterality of the aortic arch and anomalies of the subclavian artery-reliable indicators for 22q11.2 deletion syndromes? Eur J Pediatr. 2004;163(11):642-645.
- Moore KL, Persaud TVN. The Developing Human: Clinically oriented embryology. 6th ed. Philadelphia: W.B. Saunders Company; 1998:481-482.
- Weinberg PM. Aortic arch anomalies. J Cardiovasc Magn Reson. 2006;8(4):633-643.
- Kawano T, Soeda M, Hata H, Hirayama A. Multidetector computed tomography images of right aortic arch and a left subclavian artery arising from a Kommerell diverticulum. J Am Coll Cardiol. 2010;55(7):697.
- Nath PH, Castaneda-Zuniga W, Zollikofer C, etc. Isolation of a subclavian artery. AJR Am J Roentgenol. 1981;137(4):683-688.
- Carnero Alcázar M, Marianeschi S, Ruiz Alonso E, García Torres E, Comas JV. Left arm underdevelopment secondary to an isolated left subclavian artery in tetralogy of Fallot. Ann Thorac Surg. 2010;89(2):637-639.
- Dougherty MJ, Calligaro KD, Savarese RP, DeLaurentis DA. Atherosclerotic aneurysm of the intrathoracic subclavian artery: a case report and review of the literature. J Vasc Surg. 1995;21(3):521-529.
____________________________________________
From the Cardiology Department, Ankara University, Ankara, Turkey.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted November 21, 2011 and accepted December 14, 2011.
Address for correspondence: Basar Candemir, MD, Ankara University School of Medicine, Cardiology Department, Heart Center, 06590, Dikimevi, Ankara, Turkey. E-mail: Basarcandemir@yahoo.com

