

Very Long-Term Clinical Follow-up After Fractional Flow Reserve-Guided Coronary Revascularization
Abstract: Background. Randomized trials using measurement of fractional flow reserve (FFR) to guide percutaneous coronary intervention (PCI) have demonstrated both safety and efficacy with regard to cardiac events. Real-world, long-term outcomes using an FFR-based revascularization strategy are unknown. Methods. Prospective clinical data were collected on consecutive patients referred for coronary angiography and found to have lesions of intermediate severity where the operators were unable to make a decision regarding revascularization based on angiographic, clinical, and stress testing parameters. FFR was measured on intermediate lesions, and revascularization was deferred on those lesions with a measurement >0.8. Clinical outcomes of interest included death, myocardial infarction, and late revascularization status. Results. A total of 151 patients were included in this study. Fifty-seven patients (37.7%) underwent revascularization based on their FFR measurement. The mean length of follow-up was 6.1 years (range, 5-10 years). Follow-up was completed in 97.0%. At the end of the follow-up period, 107 patients (70.9%) were alive. Late revascularization had been performed in 18 patients (11.9%). Comparing the initial revascularization group with the group in which revascularization was deferred, 64.9% and 74.5% were alive, respectively (P=.29). Of the initial revascularization group, 12.3% had undergone late revascularization of the lesion on which FFR was originally performed, compared with 11.7% in the deferred group (P=.99). Conclusions. FFR is a useful adjunct to coronary angiography in selecting patients with lesions of intermediate angiographic severity in whom coronary revascularization may be safely deferred.
J INVASIVE CARDIOL 2012;24(7):309-315
Key words: fractional flow reserve, pressure wire, percutaneous coronary intervention
____________________________________________________
Coronary artery revascularization is appropriate and indicated for many patients with coronary artery disease (CAD).1-3 Selection of patients for revascularization based on visual assessment of coronary stenosis by angiography alone is difficult in some cases since angiography provides limited insight into the physiologic significance of intermediate coronary lesions.4-6 Additional concerns regarding the association between drug-eluting stents and late complications, continued exposure to dual anti-platelet therapy, and increased costs make appropriate use of these devices critical.7
Measurement of fractional flow reserve (FFR) can be used to quantify the flow limitation caused by a coronary stenosis at the time of angiography. When compared to traditional angiography-guided PCI, a strategy of FFR-guided PCI has been shown to be safe and effective in randomized controlled trials.8,9 The Fractional Flow Reserve versus Angiography for Multivessel Evaluation (FAME) study demonstrated that an FFR-based revascularization strategy significantly reduced the combined rate of death, non-fatal myocardial infarction, and repeat revascularization over 1 year, while reducing overall costs.8,10 Long-term, real-world outcomes using this strategy, however, are largely unknown.
We report our experience using a strategy of FFR-guided revascularization in patients with long-term clinical follow-up of up to 10 years. The objective of this analysis was to compare long-term clinical outcomes in patients with intermediate coronary lesions in whom an FFR measurement led to initial coronary revascularization with those whose FFR measurement led to the deferral of revascularization.
Methods
All patients who underwent coronary angiography in our cardiac catheterization laboratory were included in this analysis if an FFR-guided decision regarding revascularization was used during their procedure. All procedures were performed by 2 experienced interventional operators (JDL and SPS) at the Manhattan Campus of the VA New York Harbor Healthcare System in New York, NY, from January 1, 2000 to December 31, 2005.
Coronary angiography was performed using standard techniques and views. The severity of all coronary lesions was initially graded by the operator’s qualitative assessment. The decision to pursue FFR measurement as an adjunct to angiography was made by the operator only in cases when additional information was required after review of angiographic, clinical, and stress testing data to make a decision regarding coronary revascularization. Most commonly, this was needed when stress testing had not been performed or when the results of stress testing appeared discordant from the angiographic data.
For each stenosis included in our analysis, FFR was measured during maximum hyperemia using a coronary pressure guidewire (Radi Medical Systems). Maximum hyperemia was induced using an intracoronary bolus of adenosine (20-40 µg), and the FFR was calculated from the ratio of the mean hyperemic distal coronary pressure and the mean hyperemic proximal coronary pressure.11,12 Often, multiple FFR measurements of the lesion were made, and the lowest measurement was used as the final assessment.
The decision to proceed with or defer coronary revascularization was left to the discretion of the operator. In general, lesions with FFR measurements of <0.75 were considered for revascularization; medical therapy was recommended for lesions with measurements of >0.8. Lesions with measurements in the range of 0.75-0.8 were considered intermediate, and decisions regarding revascularization were made according to the operator’s judgment. The method by which revascularization was performed was also left to the operator and included balloon angioplasty, coronary artery stenting with either bare-metal or drug-eluting stents, and referral for coronary artery bypass grafting (CABG).
Baseline and follow-up clinical assessments were made by review of the patient’s electronic medical record available through the Veterans Administration. All available records were assessed through July 1, 2010. All follow-up clinical encounters, decisions regarding medical management, and referral for additional testing or revascularization procedures were scheduled or performed according to routine clinical practice at the discretion of the patient’s healthcare providers.
Clinical outcomes of interest included vital status, subsequent myocardial infarction, clinical angina status, and late revascularization of the index lesion. Classification of patient’s mode of presentation, medical co-morbidities, follow-up clinical status, and presence of myocardial infarction were adjudicated by two independent clinicians blinded to coronary catheterization procedural data and index revascularization status. Myocardial infarction (MI) was defined as a rise and fall of cardiac biomarkers above the 99th percentile of the upper reference limit in the setting of symptoms consistent with ischemia or electrocardiographic changes including ST-segment deviation, new left bundle branch block, or new pathologic Q-waves.13 Periprocedural MI was excluded from the analysis.
Stress tests results performed prior to the patient’s referral for angiography were also examined and assessed for concordance and discordance with the subsequent FFR results. FFR results were considered concordant with stress test results if the FFR measurement was <0.8 and there was evidence of ischemia in the corresponding coronary distribution on SPECT imaging, or the FFR measurement was >0.8 and there was no evidence of ischemia in the corresponding coronary distribution on SPECT imaging. The extent of ischemia noted on SPECT imaging was classified according to number of coronary territories affected by ischemia. Patients that underwent exercise stress testing without imaging were excluded from this part of the analysis.
Categorical variables are expressed as proportions and compared using the chi-square test or Fisher’s exact test. Normally distributed continuous variables are presented using means and standard deviations, and comparisons were performed using an unpaired two-sided t-test. Non-normally distributed continuous variables are expressed as medians and interquartile ranges, and comparisons were performed using a Wilcoxon test. Clinically relevant patient-level baseline measures were entered into a multivariate logistic regression analysis to investigate relationships with the outcomes of interest. Time-to-death data are presented as a Kaplan-Meier estimate and compared with the log-rank test. A two-sided P<.05 was considered to indicate a statistically significant result. All statistical analyses were performed using SPSS for Windows, version 17.0 (SPSS Inc).
Results
 From January 1, 2000, through December 31, 2005, a total of 151 patients underwent FFR measurement to assess the significance of 171 coronary lesions. Of these patients, 57 (37.7%) had immediate coronary revascularization or referral for CABG, and 94 (62.3%) had revascularization deferred. The mean length of follow-up was 6.1 years.
From January 1, 2000, through December 31, 2005, a total of 151 patients underwent FFR measurement to assess the significance of 171 coronary lesions. Of these patients, 57 (37.7%) had immediate coronary revascularization or referral for CABG, and 94 (62.3%) had revascularization deferred. The mean length of follow-up was 6.1 years.
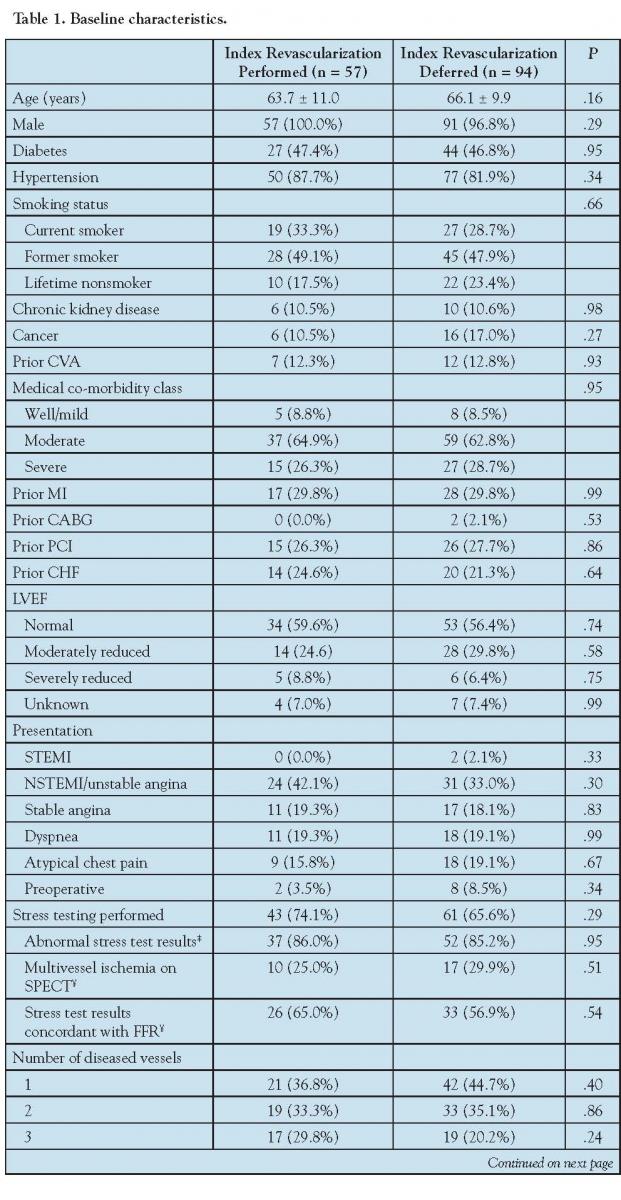
Baseline characteristics were comparable in both groups (Table 1). The mean age 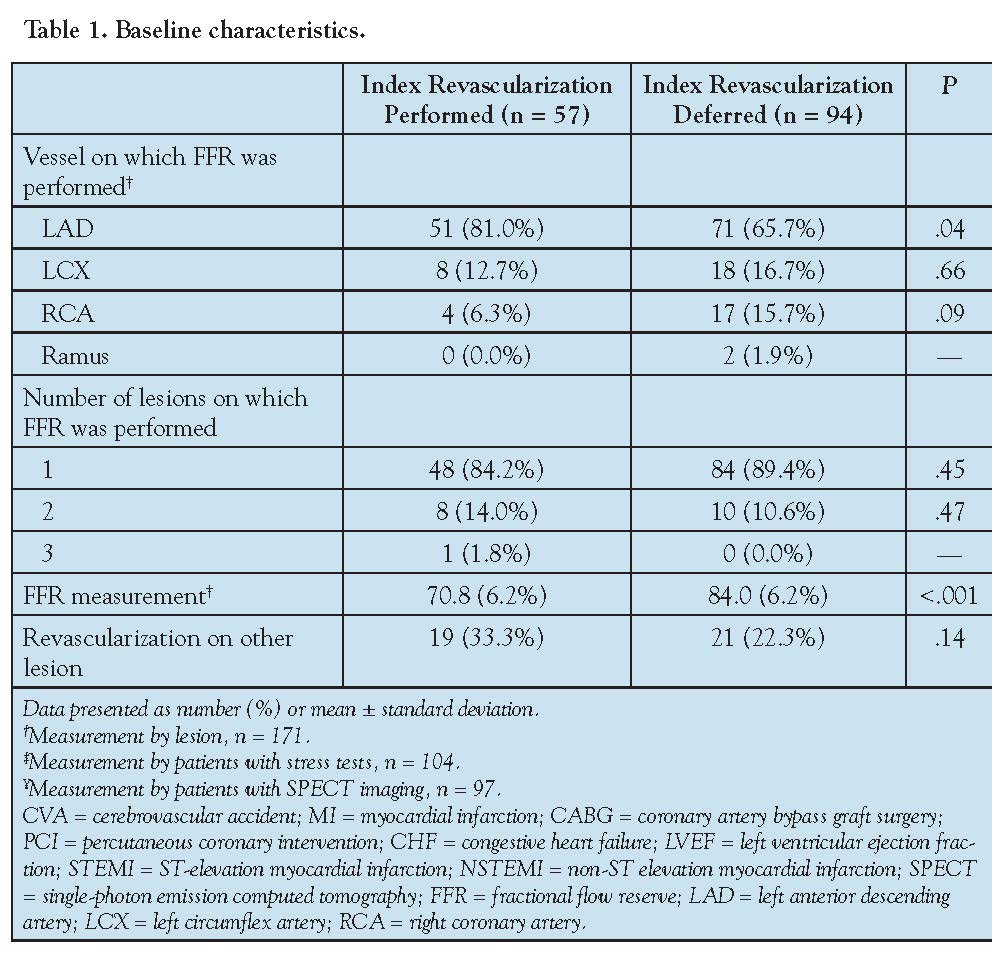 was 65.2 years, and the majority of the patients were male. Approximately one-half of the patients had diabetes, and one-third had prior MI, prior PCI, or abnormal left ventricular function. Over 90% of the patients were considered to have moderate or severe medical co-morbidities. The modes of presentation were similar in both groups, with over one-third of the patients presenting with an acute coronary syndrome. The majority of patients had preceding stress tests, and over 85% of these tests were considered abnormal. Approximately one-quarter of the stress test results included SPECT imaging consistent with multi-vessel ischemia. On angiography, the number of diseased vessels was not significantly different, with more than one-half of patients presenting with multi-vessel coronary disease.
was 65.2 years, and the majority of the patients were male. Approximately one-half of the patients had diabetes, and one-third had prior MI, prior PCI, or abnormal left ventricular function. Over 90% of the patients were considered to have moderate or severe medical co-morbidities. The modes of presentation were similar in both groups, with over one-third of the patients presenting with an acute coronary syndrome. The majority of patients had preceding stress tests, and over 85% of these tests were considered abnormal. Approximately one-quarter of the stress test results included SPECT imaging consistent with multi-vessel ischemia. On angiography, the number of diseased vessels was not significantly different, with more than one-half of patients presenting with multi-vessel coronary disease.
With regard to FFR measurement and revascularization, the LAD was the most frequently assessed coronary artery, and it was more often assessed in patients in the initial revascularization group (81.0%) than in the deferred group (65.7%; P=.04). In patients with a preceding stress test, FFR results were concordant with the nuclear findings in 67.2% of those in the initial revascularization group and 59.0% in the deferred group (P=.38). By design, the FFR measurement was significantly lower in the initial revascularization group (0.71) compared to that of the deferred group (0.83; P<.001). There was a trend toward more revascularization of additional lesions in the initial revascularization group (33.3%) than the deferred group (22.3%; P=.14). In patients who underwent initial revascularization of the index lesion, 78% underwent PCI while the remaining patients underwent CABG.
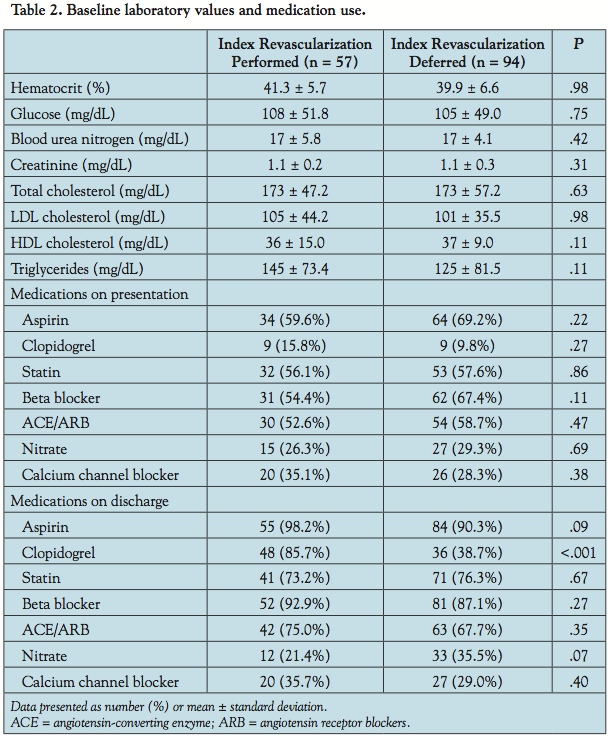 Baseline laboratory measurements and use of medications were similar between both groups (Table 2). Following index cardiac catheterization, use of all medication classes increased in comparison to presentation with the exception of nitrates and calcium channel blockers. The proportion of patients using clopidogrel on discharge was significantly higher in the initial revascularization group (85.7%) compared to the deferred group (38.7%; P<.001).
Baseline laboratory measurements and use of medications were similar between both groups (Table 2). Following index cardiac catheterization, use of all medication classes increased in comparison to presentation with the exception of nitrates and calcium channel blockers. The proportion of patients using clopidogrel on discharge was significantly higher in the initial revascularization group (85.7%) compared to the deferred group (38.7%; P<.001).
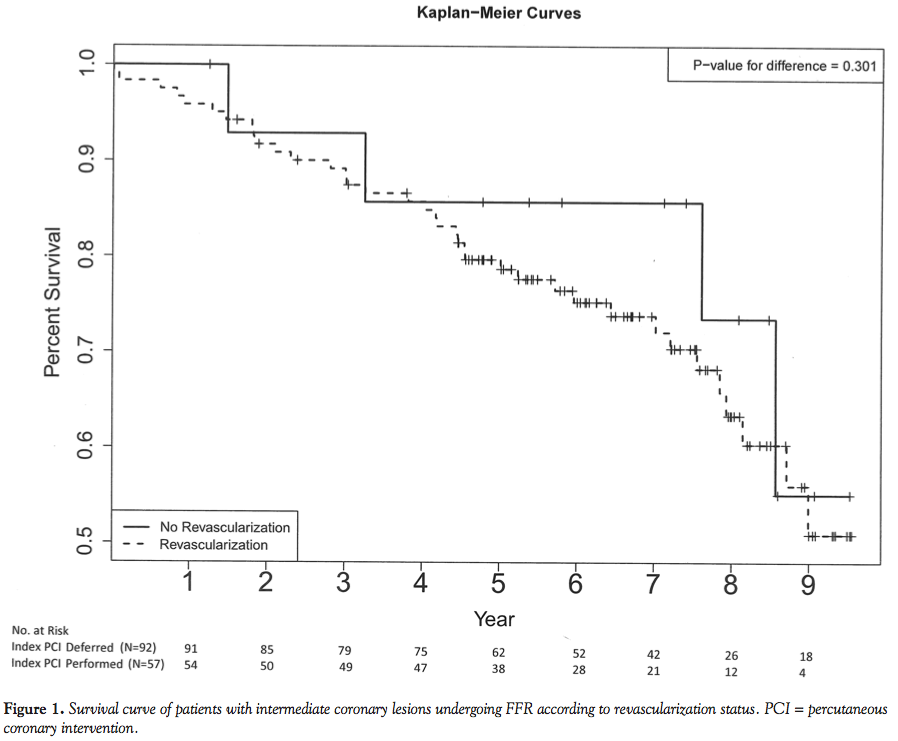
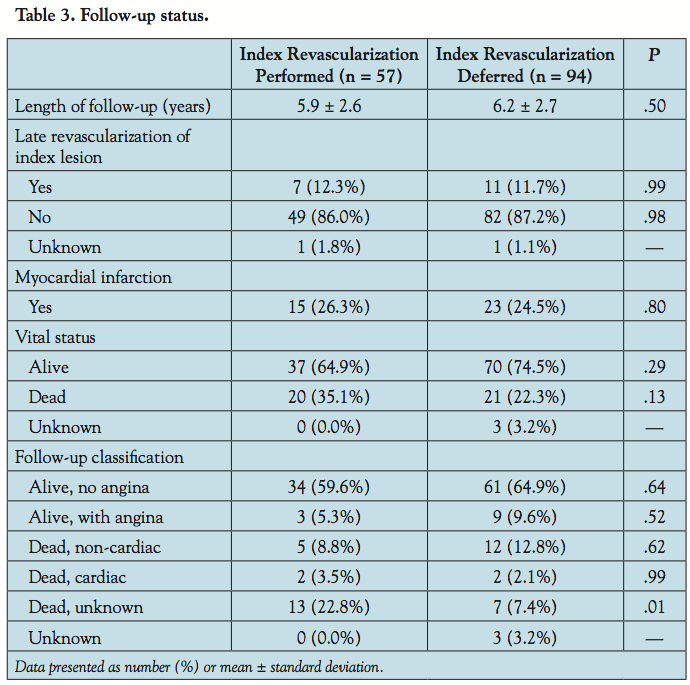 Follow-up was complete in all but 3 patients (97%). All 3 patients with unknown follow-up status were in the deferred group. The mean length of follow-up was 5.9 years in the initial revascularization group and 6.2 years in the deferred group (P=.50). During the follow-up period, death occurred in 20 patients (35.1%) in the initial revascularization group and 21 patients (22.3%) in the deferred group (P=.13; Table 3). The cause of death was unknown in most cases in the initial revascularization group, while a non-cardiac cause of death was most common in the deferred group. Survival in both groups is shown by means of Kaplan-Meier curves, and no significant difference was noted (P=.30; Figure 1).
Follow-up was complete in all but 3 patients (97%). All 3 patients with unknown follow-up status were in the deferred group. The mean length of follow-up was 5.9 years in the initial revascularization group and 6.2 years in the deferred group (P=.50). During the follow-up period, death occurred in 20 patients (35.1%) in the initial revascularization group and 21 patients (22.3%) in the deferred group (P=.13; Table 3). The cause of death was unknown in most cases in the initial revascularization group, while a non-cardiac cause of death was most common in the deferred group. Survival in both groups is shown by means of Kaplan-Meier curves, and no significant difference was noted (P=.30; Figure 1).
 Subsequent MI occurred in 15 patients (26.3%) in the initial revascularization group, and 23 patients (24.5%) in the deferred group (P=.80). Late revascularization of the index lesion was subsequently performed in 7 patients (12.3%) in the initial revascularization group and 10 patients (11.7%) in the deferred group (P=.84). At the end of follow-up, 59.6% of patients in the initial revascularization group were alive and free of angina, compared to 64.9% of patients in the deferred group (P=.64). Revascularization status of the index lesion at the time of FFR was not a predictor of death, MI, or late revascularization when examined in a univariate analysis or multivariate model.
Subsequent MI occurred in 15 patients (26.3%) in the initial revascularization group, and 23 patients (24.5%) in the deferred group (P=.80). Late revascularization of the index lesion was subsequently performed in 7 patients (12.3%) in the initial revascularization group and 10 patients (11.7%) in the deferred group (P=.84). At the end of follow-up, 59.6% of patients in the initial revascularization group were alive and free of angina, compared to 64.9% of patients in the deferred group (P=.64). Revascularization status of the index lesion at the time of FFR was not a predictor of death, MI, or late revascularization when examined in a univariate analysis or multivariate model.
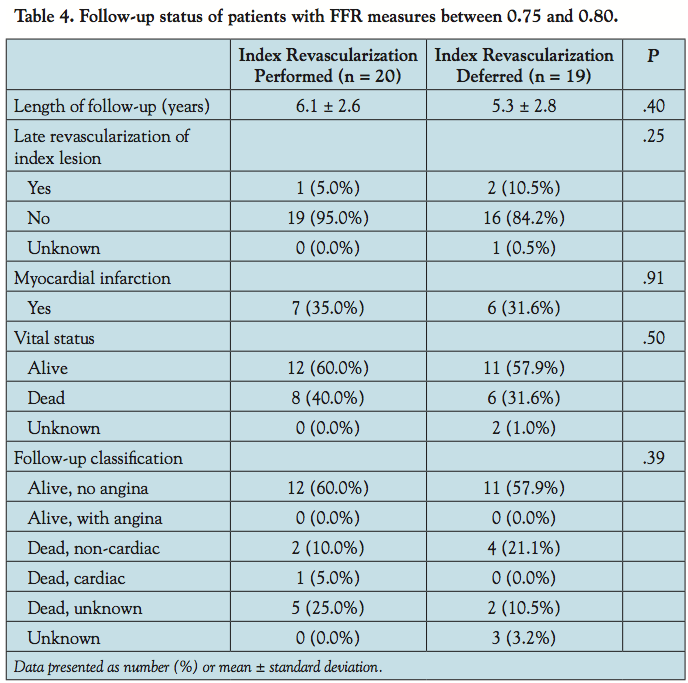 In addition, 39 patients had a total of 40 lesions with an FFR measurement in the so-called FFR “grey zone,” between 0.75 and 0.80. Initial revascularization was performed on 20 of these patients and 19 were deferred. Of the 20 patients who underwent initial revascularization, 17 (85%) underwent PCI; the remaining 3 patients (15%) underwent CABG. The mean length of follow-up in this small subgroup was 5.7 years, though 2 of the patients had an unknown clinical status at the end of follow-up. Long-term clinical outcomes in this small group of patients were similar to those of the overall cohort, and no significant differences between the initial revascularization and deferred groups were noted (Table 4).
In addition, 39 patients had a total of 40 lesions with an FFR measurement in the so-called FFR “grey zone,” between 0.75 and 0.80. Initial revascularization was performed on 20 of these patients and 19 were deferred. Of the 20 patients who underwent initial revascularization, 17 (85%) underwent PCI; the remaining 3 patients (15%) underwent CABG. The mean length of follow-up in this small subgroup was 5.7 years, though 2 of the patients had an unknown clinical status at the end of follow-up. Long-term clinical outcomes in this small group of patients were similar to those of the overall cohort, and no significant differences between the initial revascularization and deferred groups were noted (Table 4).
Discussion
Randomized clinical trials have shown that an FFR-guided revascularization strategy is safe, effective, and reduces overall healthcare costs in the short-term (1-2 years).8-10 Our data obtained in a non-randomized, real-world setting suggest that there are no adverse long-term outcomes associated with use of an FFR-guided revascularization strategy for intermediate-severity coronary lesions. We believe our cohort has one of the longest follow-up periods of patients undergoing FFR-based revascularization, and includes a higher-risk patient population than most prior analyses.14-17
The two largest randomized trials evaluating the use of FFR are the FAME study and the Deferral of Percutaneous Coronary Intervention (DEFER) study. In the FAME study, lesions with >50% stenosis were first identified as targets for percutaneous intervention based on angiography, and patients were then randomized to a routine angiography-guided intervention or an FFR-guided approach.8 In the DEFER study, stable patients with intermediate coronary lesions (>50% stenosis) and no evidence of reversible ischemia were randomized to deferral or performance of PCI, and FFR was used to guide therapy in the deferral arm only.9 While these two trials compare the use of an FFR-guided strategy to the usual angiography-guided care, our analysis examines long-term outcomes when the FFR-guided PCI strategy supported by these studies is applied to patients in a non-randomized fashion.
In comparison to FAME and DEFER, our overall cohort is most similar to the FFR arm of FAME: all patients in this group underwent FFR evaluation and PCI was performed on lesions with FFR ≤0.80. The deferred group in our study is most similar to the deferred group in DEFER: all patients in this group also underwent FFR evaluation, and no PCI was performed based on the results (FFR ≥0.75). It must be acknowledged that the patients enrolled in FAME were scheduled for coronary intervention, whereas our patients were referred for both diagnostic studies and PCI. Long-term clinical outcomes from FAME, DEFER, and other studies are available, with varied results. In FAME, 2-year rates of death, MI, and CABG or PCI in the FFR arm of the study were 2.6%, 6.1%, and 10.6%, respectively.14 In DEFER, 5-year rate of both cardiac and non-cardiac death was 3.3% in the deferred group. Target vessel revascularization was performed in 8.9% in this group, and no Q-wave or non-Q wave MIs were noted.15 When compared to these trials, our cohort had a much higher rate of death and MI, regardless of whether revascularization was performed or deferred, though the rate of subsequent revascularization was similar.
The higher rate of adverse outcomes in our cohort is likely explained by the longer follow-up period, the high proportion of patients presenting with an acute coronary syndrome, and the high degree of medical co-morbidities present. DEFER was a study of patients with stable coronary disease and no ischemia on stress testing, and while a similar proportion of patients included in FAME presented with unstable angina, our patient group had a much higher incidence of diabetes and hypertension when compared with these trials.8,9 Also, as a non-randomized, real-world analysis, our study population likely includes patients with medical co-morbidities, such as cancer, chronic kidney disease, and severe heart failure, that might otherwise preclude patients from inclusion in a randomized controlled trial. Overall, our cohort represents a sicker population when compared with most studies of FFR, including previously reported results from other non-randomized cohorts.16,17
Study limitations. There are several limitations to our study. First, our analysis is a non-randomized observational cohort study: FFR of intermediate coronary lesions was performed according to operator discretion — not per protocol —as would be the case in a randomized controlled trial. As such, unrecognized confounders may have entered into the clinical decision to initially perform an FFR measurement, or in the ultimate decision regarding revascularization. Our inclusion of only a small number of lesions over a decade-long period suggests this is the case, despite the fact that the same operators performed the procedures over the entire course of the study period. Since we did not examine data on patients in whom FFR was not performed, it is difficult to discern the rationale behind FFR use in each case compared to those in which it was not performed.
One possibility is that these unmeasured confounders may have selected for a lower-risk patient group, as higher-risk patients may have been felt to have a greater need for aggressive revascularization without further ancillary coronary testing. Given the comparatively high burden of co-morbid conditions in our patient group, and the mortality rate of approximately 28% over a mean of 6 years, we feel this is unlikely to be true.
Certainly, operator comfort and expertise in performance and interpretation of FFR, as well as trends in the overall use of FFR, changed over the study period. As the accumulated data pool supporting the use of FFR has grown, so has the use of FFR in our laboratory, raising the possibility that there may also be unrecognized differences in FFR use among patients included in earlier and later parts of the study. Additionally, more recent trends in technique of FFR measurement, including utilization of increased adenosine doses for increased sensitivity, are not captured with our data.18
The ability to capture follow-up events that did not occur within our medical system was also limited. Although many of our patients exclusively receive medical care within the VA healthcare system, and significant hospitalizations and cardiac events were likely to be captured in the electronic medical record even when occurring outside of our system, it is possible that significant clinical events were missed. Likewise, while patient deaths occurring outside of the VA system are recorded in the medical record, data useful in determining a cause of death were limited. Follow-up was also incomplete in 3 patients. An additional analysis in which a “worst case scenario” of repeat revascularization, MI, and cardiac death was assigned to the 3 missing patients was performed and no significant alterations in the overall findings of this cohort study were found.
Our study began in the era prior to drug-eluting stents and concluded in 2005 when a large majority of procedures were done with these devices. It is possible that our results would have been different if all the procedures were done in the current era, but this limitation is inherent in any study evaluating very long-term outcomes since therapies change over time.
Finally, our study represents a small cohort of male patients at a single VA medical center. Though no significant differences in outcomes of interest were noted, the small sample size of our study limits our ability to detect such differences with certainty. As such, findings should be interpreted with caution. Further, the temptation to interpret our analysis as a comparison of initial revascularization and deferral of revascularization of equivalent lesions must be resisted: in our real-world analysis of our application of an FFR-guided revascularization strategy, we are only able to compare the long-term results of initial revascularization of hemodynamically significant lesions with deferral of those lesions that were angiographically suspicious yet ultimately hemodynamically insignificant as measured by FFR. Given that our results are largely consistent with those found in larger randomized trials, we believe that this analysis adds to the accumulating data supporting the use of FFR in guiding revascularization decision-making for lesions of intermediate angiographic severity in the cardiac catheterization laboratory.
Conclusions
Use of FFR as an adjunct to coronary angiography in selecting patients with coronary lesions of intermediate angiographic severity in whom coronary revascularization may be deferred is a feasible and safe strategy. We did not detect significant differences in the risk of death or need for late revascularization for up to 10 years in patients in whom revascularization was deferred based on FFR measurement when compared to those patients with significant FFR measurements requiring revascularization. Further studies of FFR with very long-term follow-up are needed.
References
- Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Accessed at: www.myamericanheart.org.
- Mehta SR, Cannon CP, Fox KAA, et al. Routine vs selective invasive strategies in patients with acute coronary syndromes. JAMA. 2005;293(23):2908-2917.
- Shaw LJ, Berman DS, Maron DJ. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117(10):1283-1291.
- Tonino, PAL, Fearon WF, De Bruyne B, et al. Angiographic versus functional severity of coronary artery stenosis in the FAME study. J Am Coll Cardiol. 2010;55(25):2816-2821.
- Fischer JJ, Samady H, McPhearson JA, et al. Comparison between visual assessment and quantitative angiography versus fractional flow reserve for native coronary narrowings of moderate severity. Am J Cardiol. 2002;90(3):210-215.
- Topol EJ, Nissen SE. Our preoccupation with coronary luminology: the dissociation between clinical and angiographic findings in ischemia heart disease. Circulation. 1999;92(8):2333-2342.
- Pfisterer M, Brunner-La Rocca HP, Buser PT. Late clinical events after clopidogrel discontinuation may limit the benefit of drug-eluting stents: an observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol. 2006;48(12):2584-2591.
- Tonino, PAL, De Bruyne B, Pijls NHJ, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360(3):213-224.
- Bech GJW, De Bruyne B, Pijls NHJ, et al. Fractional flow reserve to determine the appropriateness of angioplasty in moderate artery stenosis: a randomized trial. Circulation. 2001;103(24):2928-2934.
- Fearon WF, Bornschein B, Tonino PAL, et al. Economic evaluation of fractional flow reserve guided percutaneous coronary intervention in patients with multivessel disease. Circulation. 2010;122(24):2545-2550.
- De Brunye B, Pijls NHJ, Barbato E, et al. Intracoronary and intravenous adenosine 5’-triphosphate, adenosine, papaverine, and contrast medium to assess fractional flow reserve in humans. Circulation. 2003;107(14):1877-1883.
- Pijls NHJ, Van Golder B, Van det Voort P, et al. Fractional flow reserve. A useful index to evaluate the influence of an epicardial coronary stenosis on myocardial blood flow. Circulation. 1995;92(11):3183-3195.
- Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. Circulation. 2007;116(22):2634-2653.
- Pijls NHJ, Fearon WF, Tonino PAL, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease. J Am Coll Cardiol. 2010;56(3):177-184.
- Pijls NHJ, van Schaardenburgh P, Manoharan G, et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER study. J Am Coll Cardiol. 2007;49(21):2105-2111.
- Rieber J, Jung P, Koenig A, et al. Five-year follow-up in patients after therapy stratification based on intracoronary pressure measurement. Am Heart J. 2007;153(3):403-409.
- Wongpraparut N, Yalamanchili V, Pasnoori V, et al. Thirty-month outcome after fractional flow resertve-guided versus conventional multivessel percutaneous coronary intervention. Am J Cardiol. 2005;96(7):877-884.
- De Lucca G, Venegoni L, Iorio S, Giuliani L, Marino P. Effects of increasing doses of intracoronary adenosine on the assessment of fractional flow reserve. JACC Cardiovasc Interv. 2011;4(10):1079-1084.
____________________________________________________
From the VA New York Harbor Health Care System, New York Campus and New York University School of Medicine, New York, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted December 20, 2011, provisional acceptance given January 23, 2012, final version accepted February 13, 2012.
Address for correspondence: Steven P. Sedlis, MD, Cardiology, VA New York Harbor Health Care System New York Campus, 423 East 23rd Street, New York, NY 10010. Email: Steven.Sedlis@va.gov

