

Use of the Retrograde Approach for Primary Percutaneous Coronary Intervention of an Inferior ST-Segment Elevation Myocardial Infarction
Abstract: Percutaneous coronary intervention (PCI) during ST-segment elevation myocardial infarction (STEMI) can be challenging due to limited distal vessel visualization. We present a case of challenging antegrade wiring during PCI of an inferior STEMI resulting in inadvertent subintimal wiring and ballooning. Recognition of this scenario prior to stenting allowed vessel rescue using the retrograde chronic total occlusion revascularization technique.
J INVASIVE CARDIOL 2013;25(9):483-484
Key words: retrograde approach, STEMI, primary PCI
___________________________
A 64-year-old man with symptomatic peripheral vascular disease underwent a right femoral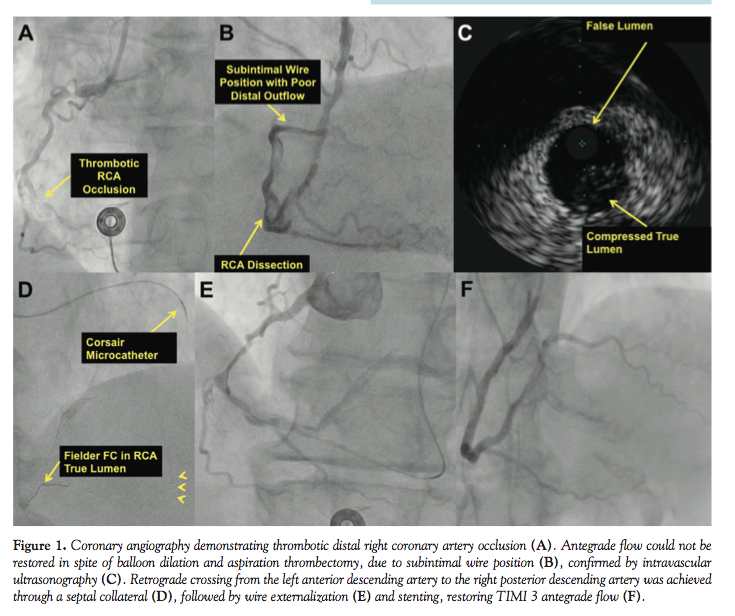 endarterectomy and profundoplasty. Postoperatively, he developed chest pain and inferior ST-segment elevation, prompting emergent cardiac catheterization, which revealed a tortuous and calcified right coronary artery (RCA) with a distal thrombotic occlusion (Figure 1A). There was significant difficulty advancing a guidewire through the occlusion. Ultimately, a Pilot 200 guidewire (Abbott Vascular) through a Venture microcatheter (St Jude Medical) crossed into what appeared to be the distal posterior descending artery. In spite of multiple balloon inflations and aspiration thrombectomy, the RCA outflow remained poor (Figure 1B). Intravascular ultrasonography demonstrated distal wire position within the subintimal space with compression of the distal true lumen (Figure 1C). Multiple attempts to re-enter the distal true lumen were unsuccessful.
endarterectomy and profundoplasty. Postoperatively, he developed chest pain and inferior ST-segment elevation, prompting emergent cardiac catheterization, which revealed a tortuous and calcified right coronary artery (RCA) with a distal thrombotic occlusion (Figure 1A). There was significant difficulty advancing a guidewire through the occlusion. Ultimately, a Pilot 200 guidewire (Abbott Vascular) through a Venture microcatheter (St Jude Medical) crossed into what appeared to be the distal posterior descending artery. In spite of multiple balloon inflations and aspiration thrombectomy, the RCA outflow remained poor (Figure 1B). Intravascular ultrasonography demonstrated distal wire position within the subintimal space with compression of the distal true lumen (Figure 1C). Multiple attempts to re-enter the distal true lumen were unsuccessful.
Left radial artery access was obtained. A Fielder FC guidewire (Abbott Vascular) was advanced over a Corsair microcatheter (Asahi Intecc) through a septal collateral into the posterior descending artery and the distal RCA (Figure 1D). The Fielder FC wire easily crossed the mid-RCA occlusion, and was advanced into the antegrade guide catheter and exchanged for a Viper wire (Cardiovascular Systems, Inc) that was externalized (Figure 1E). Multiple stents were successfully deployed in the mid and distal RCA, restoring Thrombolysis in Myocardial Infarction (TIMI) 3 flow (Figure 1F). The posterior descending was jailed by a stent deployed from the distal RCA into the posterolateral vessel and due to prolonged fluoroscopy time (46.75 minutes), radiation exposure (342,800 Gycm2), and contrast administration (525 mL), no further intervention was performed. The patient’s biomarkers peaked as follows: creatine kinase, 580 U/L; creatine kinase-MB fraction, 150.6 ng/mL; and troponin I, 9.99 ng/mL. Transthoracic echocardiogram obtained the next day showed a left ventricular ejection fraction of 48% with mild inferior/inferolateral hypokinesis.
Our case demonstrates utilization of a chronic total occlusion crossing technique in the setting of failure to cross an acute coronary occlusion due to acute myocardial infarction. Recognition of subintimal wire position is important, since subintimal stenting will result in side-branch occlusion and no reflow.1 Alternative treatment strategies include use of various guidewires with an acute distal bend2 or a dedicated re-entry device (Stingray; Boston Scientific Corporation).3 If all attempts to re-enter the distal true lumen fail, emergency coronary artery bypass graft surgery may be required.
References
- Patel V, Banerjee S, Brilakis ES. Treatment of inadvertent subintimal stenting during intervention of a coronary chronic total occlusion. Future Medicine Interv Cardiol. 2013;5:166-169.
- Michael TT, Papayannis AC, Banerjee S, Brilakis ES. Subintimal dissection/reentry strategies in coronary chronic total occlusion interventions. Circ Cardiovasc Interv. 2012;5(5):729-738.
- Martinez-Rumayor AA, Banerjee S, Brilakis ES. Knuckle wire and stingray balloon for recrossing a coronary dissection after loss of guidewire position. JACC Cardiovasc Interv. 2012;5(10):e31-e32.
From the VA North Texas Healthcare System and University of Texas Southwestern Medical Center, Dallas, Texas.
Presented at the 2013 American College of Cardiology Annual Scientific Session, San Francisco, California.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Brilakis reports consulting fees/speaker honoraria from St Jude Medical, Terumo, Janssen, Sanofi, Asahi, and Bridgepoint Medical/Boston Scientific; research grant from Guerbet; spouse is an employee of Medtronic. Dr Patel and Dr Zankar have no disclosures.
Manuscript submitted May 3, 2013 and accepted June 10, 2013.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Dallas VA Medical Center (111A), 4500 South Lancaster Road, Dallas, TX 75216. Email: esbrilakis@gmail.com



