

Tumor Blush: Left Ventricular Cardiac Hemangioma with Supply From Both the Left Anterior Descending and Circumflex Arteries
Abstract: A fifty-year-old male had an echocardiogram for an abnormal electrocardiogram; it revealed a left ventricular mass. A cardiac catheterization revealed normal coronary arteries and a fine tumor blush of the cardiac tumor with feeding arteries from the circumflex as well as the second diagonal coronary vessels. Due to increased risk of embolization, he underwent surgery via a transatrial approach and a 1.5 cm cavernous-capillary hemangioma was removed from the base of the posteromedial papillary muscle. Primary tumors of the heart are rare, and the symptoms and signs depend on the location and size of the tumor. Coronary angiography remains an integral part in the evaluation of cardiac tumors and often can reveal a characteristic ‘tumor blush.’ The natural history of the tumor is unpredictable and excision of the tumor remains the treatment of choice. We present a rare case of characteristic angiographic tumor blush of a left ventricular cardiac hemangioma with feeding arteries from both the left anterior descending as well as the circumflex arteries. This rare two-system supply was due to the intracavitary location of the hemangioma, and fortunately did not pose any excessive difficulty in mobilization and excision during surgery.
J INVASIVE CARDIOL 2012;24:138–139
Key words: cardiac tumor, hemangioma
_________________________________________
Case Description
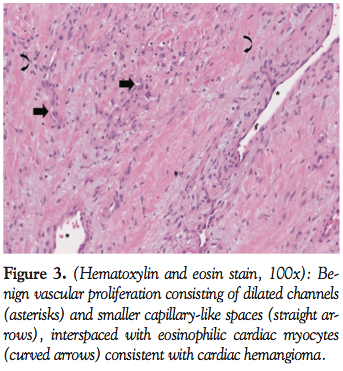
 A 53-year-old man with the history of hypertension and hyperlipidemia was found to have an abnormal electrocardiogram as part of a routine physical examination. A subsequent echocardiogram noted a mobile echo density along the lateral wall of the left ventricle. Further evaluation with cardiac MR showed a round, circumscribed, and homogenous mass measuring about 1.5 cm attached to the posterior papillary muscle. The left ventricular dimensions were normal and there was moderate left atrial enlargement. A cardiac catheterization revealed normal coronary arteries and a fine tumor blush with feeding arteries from the circumflex as well as the second diagonal coronary vessels (Figures 1 and 2). Due to increased risk of embolization, he underwent surgery via transatrial approach. A 1.5 cm pedunculated polypoid tumor was removed from the base of the posteromedial papillary muscle. Histological examination noted the tumor to be a cavernous-capillary type of cardiac hemangioma (Figure 3). On follow-up, he was doing well; a repeat echocardiogram confirmed the absence of the tumor and did not reveal any mitral regurgitation. We present a rare case of cardiac hemangioma with the characteristic tumor blush with the feeding arteries arising both from the branches of the left anterior descending artery as well the circumflex artery that was excised successfully.
A 53-year-old man with the history of hypertension and hyperlipidemia was found to have an abnormal electrocardiogram as part of a routine physical examination. A subsequent echocardiogram noted a mobile echo density along the lateral wall of the left ventricle. Further evaluation with cardiac MR showed a round, circumscribed, and homogenous mass measuring about 1.5 cm attached to the posterior papillary muscle. The left ventricular dimensions were normal and there was moderate left atrial enlargement. A cardiac catheterization revealed normal coronary arteries and a fine tumor blush with feeding arteries from the circumflex as well as the second diagonal coronary vessels (Figures 1 and 2). Due to increased risk of embolization, he underwent surgery via transatrial approach. A 1.5 cm pedunculated polypoid tumor was removed from the base of the posteromedial papillary muscle. Histological examination noted the tumor to be a cavernous-capillary type of cardiac hemangioma (Figure 3). On follow-up, he was doing well; a repeat echocardiogram confirmed the absence of the tumor and did not reveal any mitral regurgitation. We present a rare case of cardiac hemangioma with the characteristic tumor blush with the feeding arteries arising both from the branches of the left anterior descending artery as well the circumflex artery that was excised successfully.
Discussion
 Primary cardiac tumors are rare in the adult population. Autopsy data suggest the prevalence is 0.02%.1 Benign tumors account for 75% of the primary tumors, of which myxomas account for 50%. Cardiac hemangiomas are nonmalignant vascular tumors consisting of blood vessels and are identical to the hemangiomas elsewhere in the body. Hemangiomas are an extremely rare form of tumor and account for only 5% of all benign cardiac tumors.2 They can be histologically classified as cavernous hemangioma (multiple, dilated thin-walled vessels), capillary hemangioma (small vessels like capillaries), and arteriovenous hemangioma or circoid aneurysm (dysplastic malformation of arteries and veins). They often have combined features of capillary, cavernous, and arteriovenous hemangiomas. Among them, cavernous and capillary types are encountered more frequently.
Primary cardiac tumors are rare in the adult population. Autopsy data suggest the prevalence is 0.02%.1 Benign tumors account for 75% of the primary tumors, of which myxomas account for 50%. Cardiac hemangiomas are nonmalignant vascular tumors consisting of blood vessels and are identical to the hemangiomas elsewhere in the body. Hemangiomas are an extremely rare form of tumor and account for only 5% of all benign cardiac tumors.2 They can be histologically classified as cavernous hemangioma (multiple, dilated thin-walled vessels), capillary hemangioma (small vessels like capillaries), and arteriovenous hemangioma or circoid aneurysm (dysplastic malformation of arteries and veins). They often have combined features of capillary, cavernous, and arteriovenous hemangiomas. Among them, cavernous and capillary types are encountered more frequently.
 Hemangiomas can present at all ages, though the diagnosis is usually made during the fifth decade of life.3 They usually are red-blue in color and appear as a soft, spongy, non-encapsulated mass. Commonly they are single, sessile, or polypoid and range from 2-3.5 cm. The epicardium is the most common location for cardiac hemangiomas, but they may also be found in myocardium and the endocardium. Bizzard et al found that 21% of cardiac hemangiomas involved the anterior wall of the right ventricle and 21% the lateral wall of the left ventricle.4
Hemangiomas can present at all ages, though the diagnosis is usually made during the fifth decade of life.3 They usually are red-blue in color and appear as a soft, spongy, non-encapsulated mass. Commonly they are single, sessile, or polypoid and range from 2-3.5 cm. The epicardium is the most common location for cardiac hemangiomas, but they may also be found in myocardium and the endocardium. Bizzard et al found that 21% of cardiac hemangiomas involved the anterior wall of the right ventricle and 21% the lateral wall of the left ventricle.4
Most cardiac hemangiomas are found incidentally as patients are usually asymptomatic, as was the case with our patient. Symptoms, if present, depend on the location, size of the tumor, and its relationship to the surrounding structures. Symptomatic patients may present with dyspnea, palpitation, atypical chest pain, or even angina due to coronary steal. In some patients, cardiac hemangiomas cause arrhythmias, pericardial effusions, congestive heart failure, right ventricular outflow obstruction, coronary insufficiency, embolization, and sudden death.
Echocardiography is a sensitive and noninvasive modality for detecting hemangiomas.5 Cardiac catheterization and magnetic resonance imaging (MRI) are superior in the qualitative diagnosis of the tumor. MRI can demonstrate the extent of intramural development more accurately and hypervascular nature of the hemangioma.
Cardiac catheterization can reveal a characteristic ‘tumor blush.’ A tumor blush is the enhancement of the tumor by the contrast agents, representing abnormal new vessel formation feeding the tumor. The tumor blush has been previously described in a variety of cardiac tumors, including hemangiomas, myxomas, and pheochromocytomas among others. Coronary angiography plays an important role in the preoperative assessment of the cardiac tumors to evaluate the feeding arteries arising from the coronary vessels and also to exclude obstructive coronary artery disease. Needless to say, such information is necessary to plan the operative intervention. In our patient, the feeding arteries arose from both the diagonal branch of the left descending artery and the circumflex artery. This has not been described previously, and is likely due to the tumor location within the left ventricular cavity. The tumor was easily mobilized and excised; it did not present any undue surgical challenges.
The natural history of cardiac hemangioma is unpredictable and not entirely known, as they are often diagnosed at postmortem examinations. Complete resection remains the treatment of choice. After complete resection, the prognosis is generally favorable with a low recurrence rate. Even an incomplete resection is reported to produce long-term benefits. Spontaneous resolution and regression after treatment with steroids have been rarely reported.
Acknowledgments. The authors would like to gratefully acknowledge the contribution of Jennifer Garbaini, MD, Division of Pathology, Albany Medical Center for providing the images used in this article.
References
- Reynen K. Frequency of primary tumors of the heart. Am J Cardiol. 1996;77(1):107.
- Serri K Schraub P, Lafitte S, Roudaut R. Cardiac hemangiomas presenting as atypical chest pain, Eur J Echocardiogr. 2007;8(1):17-18.
- Thomas JE, Eror AT, Kenney M, Caravalho J Jr. Asymtomatic right cavernous hemangioma: a case report and review of literature. Cardiovasc Pathol. 2004;13(6):341-344.
- Bizzard C, Latremoui C, Jebara VA, et al. Cardiac hemangioma. Ann Thorac Surg. 1993;56(2):390-394.
- Cunningham T, Lawrie GM, Stavinoha J Jr, Quinones MA, Zoghbi WA. Cavernous hemangioma of right ventricle: echocardiographic-pathologic correlates. J Am Soc Echocardiogr. 1993;6(3 Pt 1):335-340.
_________________________________________
From the Division of Cardiology, Albany Medical Center, Albany, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted August 8, 2011, provisional acceptance given August 15, 2011, final version accepted November 15, 2011.
Address for correspondence: Dr. Avinash Murthy, 75, Willett Street, Albany, NY 12210. Email: avinklr@yahoo.com

