

ADVERTISEMENT
Successful Placement of a Stent in a Previously Treated Un-Stentable Vessel Segment, Made Possible by the ACS Hi-Torque Wiggle Wire‚Ñ¢: A Case Report
 Case Description. A 66-year-old male presented with angina pectoris. He had a long history of coronary artery disease treated with multiple coronary interventions over an eight-year period. Significant cardiac risk factors included hypertension and hyperlipidemia. His first coronary intervention was in 1993 when a tortuous RCA with a proximal Shepherd’s Crook underwent percutaneous transluminal coronary angioplasty (PTCA). He did well until 1997 when he presented with recurrent symptoms and developed a new lesion in the
Case Description. A 66-year-old male presented with angina pectoris. He had a long history of coronary artery disease treated with multiple coronary interventions over an eight-year period. Significant cardiac risk factors included hypertension and hyperlipidemia. His first coronary intervention was in 1993 when a tortuous RCA with a proximal Shepherd’s Crook underwent percutaneous transluminal coronary angioplasty (PTCA). He did well until 1997 when he presented with recurrent symptoms and developed a new lesion in the 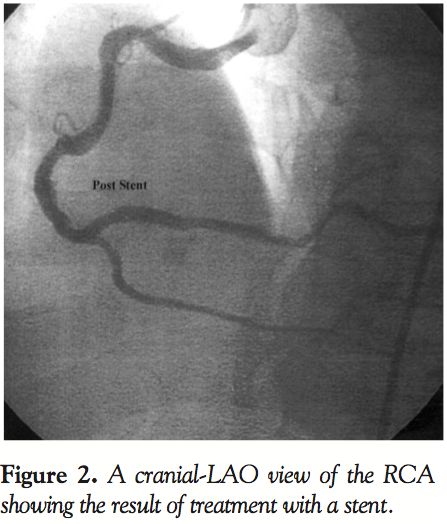 proximal RCA treated with PTCA and a 4.0 x 15 mm Palmaz-Schatz Stent (Johnson and Johnson, New Brunswick, New Jersey). In 2000, the patient again developed symptoms and was found to have mild proximal RCA stenosis in the previously stented segment, a new 75% stenosis in the originally treated PTCA site (1993) and some mild distal disease. With some difficulty, a 4.0 x 13 mm Tetra Stent (ACS/Guidant, Santa Clara, Calif.) was deployed, and due to an edge dissection, an additional 3.5 x 8.0
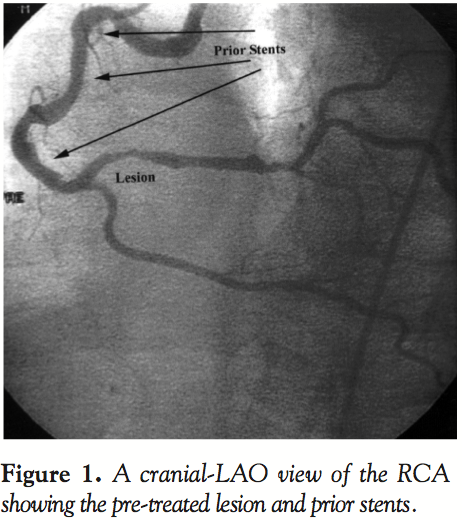
proximal RCA treated with PTCA and a 4.0 x 15 mm Palmaz-Schatz Stent (Johnson and Johnson, New Brunswick, New Jersey). In 2000, the patient again developed symptoms and was found to have mild proximal RCA stenosis in the previously stented segment, a new 75% stenosis in the originally treated PTCA site (1993) and some mild distal disease. With some difficulty, a 4.0 x 13 mm Tetra Stent (ACS/Guidant, Santa Clara, Calif.) was deployed, and due to an edge dissection, an additional 3.5 x 8.0  mm Tetra Stent was placed distally in overlapping fashion. Five months later, due to recurrent symptoms, the RCA was again found to have recurrent disease. The area of previously diagnosed mild distal disease now progressed to critical disease with a 90% minimally calcified stenosis distal to the prior stented segments, which were widely patent. PTCA was performed on the distal segment, leaving a less than 25% residual stenosis and no dissection. Despite multiple attempts with an assortment of guiding catheters (JR4, Hockey-stick, Amplatz, and Multipurpose), wires (hydrophyllic, extra-support, and soft) and techniques (femoral and brachial access), a stent could not be passed down the tortuous vessel, especially through the previously stented segments. One year later, the patient again developed recurrent disease in the same area of the RCA and again could only be treated with PTCA. Finally, one year later, recurrent disease in the same un-stented region of the RCA prompted another intervention (Figure 1). The lesion was again treated with PTCA via the femoral artery, however a novel wire designed to assist in the delivery of a stent in complex anatomical situations was used. An ACS Hi-Torque Wiggle Wire™ (ACS/Guidant, Santa Clara, Calif.) was advanced across the treated area and a 3.0 x 13 mm Penta Stent (ACS/Guidant, Santa Clara, Calif.) was easily advanced and deployed, resulting in successful treatment and 110% of pre-treatment lumen diameter (Figure 2). At nine months, the patient is completely asymptomatic.
mm Tetra Stent was placed distally in overlapping fashion. Five months later, due to recurrent symptoms, the RCA was again found to have recurrent disease. The area of previously diagnosed mild distal disease now progressed to critical disease with a 90% minimally calcified stenosis distal to the prior stented segments, which were widely patent. PTCA was performed on the distal segment, leaving a less than 25% residual stenosis and no dissection. Despite multiple attempts with an assortment of guiding catheters (JR4, Hockey-stick, Amplatz, and Multipurpose), wires (hydrophyllic, extra-support, and soft) and techniques (femoral and brachial access), a stent could not be passed down the tortuous vessel, especially through the previously stented segments. One year later, the patient again developed recurrent disease in the same area of the RCA and again could only be treated with PTCA. Finally, one year later, recurrent disease in the same un-stented region of the RCA prompted another intervention (Figure 1). The lesion was again treated with PTCA via the femoral artery, however a novel wire designed to assist in the delivery of a stent in complex anatomical situations was used. An ACS Hi-Torque Wiggle Wire™ (ACS/Guidant, Santa Clara, Calif.) was advanced across the treated area and a 3.0 x 13 mm Penta Stent (ACS/Guidant, Santa Clara, Calif.) was easily advanced and deployed, resulting in successful treatment and 110% of pre-treatment lumen diameter (Figure 2). At nine months, the patient is completely asymptomatic.
_________________________________
From SJH Cardiology Associates, St. Joseph’s Hospital, Syracuse, New York.
Address reprint requests to: Alan J. Simons, MD, SJH Cardiology Associates, 101 Union Avenue, Suite 607, New York, NY 13203.
How Would you Manage this Case?
Larry J. Diaz-Sandoval, MD and Ik-Kyung Jang, MD
Knight Center for Interventional Cardiovascular Therapy Massachusetts General Hospital, Harvard Medical School
Boston, Massachusetts
It is undeniable that the advances made in the field of interventional cardiology over the past twenty years are the result of constant and resilient efforts to fulfill the needs of an ever-growing demand for new technologies. This process of innovation is accomplished through the creation of new devices by industry and the implementation and improvisation of new techniques in using these devices by interventional cardiologists. The case presented here illustrates an infrequent, however rather frustrating, scenario for the interventional cardiologist.
We agree with the authors who took a smart approach to this problem. Nonetheless, we consider worth mentioning a few other strategies that could have been employed:
- “Buddy Wire technique.” A second 0.014 guidewire could have been used in order to provide more support by preserving the local geometric relations, which would help to advance the stent delivery system.
- “Deflection technique.” A second guidewire could have been passed to the distal vessel, and then an angioplasty balloon could have been parked at the level of resistance, acting as a “shield” to block the point of resistance. This would deflect the stent delivery system through that point, allowing it to reach the lesion site.1
- “Angled-tip technique.” A small “bend” could have been created at the tip of the stent delivery system to help the stent avoid the point of resistance and allow it to pass to the lesion site.
Due to its sinusoidal design, it is often difficult to advance the Wiggle Wire. The technique we have been using in our laboratory consists in advancing an over-the-wire balloon over a regular wire, and then exchanging it for a Wiggle Wire. We consider the use of the Wiggle Wire a very effective technique that is based on the same principle as the other three techniques. Besides, the Microglide‚ coating at the distal end of the wire facilitates tracking of balloon and stent catheters through tortuous, calcified and previously stented segments.
References
- Abernethy WB, Choo JK, Oesterle SN, Jang IK. Balloon deflection technique: A method to facilitate entry of a balloon catheter into a deployed stent. Cathet Cardiovasc Interven 2000;51:312–313.
_________________________________________________________________
Raoul Bonan, MD
Montreal Heart Institute
Montreal, Quebec, Canada
This is a valuable technical paper about a “new–old” wire which will generate a good deal of interest if Guidant continues to produce it. It is an old wire, at least in concept, because it was used in the coronary “angioscopy” era to allow visualization of the entire artery.
The clinical history of this patient is interesting, especially because it shows the “Achilles Heel” of the stent: restenosis! Stent restenosis is difficult to treat, even in a non-tortuous vessel, and it is surprising that vascular brachytherapy was not mentioned at least as a catheter-based treatment option as opposed to a stent-based one which is more “tractable.”
Nevertheless, the concept of “re-centering” the tip of any device to transfer the push administrated at the other end, is part of the state-of-the-art of catheterization. The sinusoidal wire version replicated at its best the technique of pulling the wire when pushing a catheter device that will not progress any further in a vessel. Much like driving a car, accelerating (or pushing) the catheter will tend to steer the “car” toward the outside curve. Pulling the wire will “cut” toward the inside of the curve, and then re-centering the tip of the catheter will free the tip as well as the energy accumulated by the non-progressing push.
_________________________________________________________________
Rafael Beyar, MD, DSc
Director, Division of Invasive Cardiology
Rambam Medical Center
Haifa, Israel
A case similar to the one described here1 is often encountered by everyone in the catheterization laboratory experiencing a wide range of cases. While everybody is concerned these days to minimize restenosis by using the best drug-eluting stent, it is clear that the mechanical property of the procedure is a major determinant of immediate success.
Inability to cross tortuous, calcified or previously stented vessels is often the main reason for procedural failure. The case described here1 presents a patient with a proximal tortuous vessel that has been previously stented and who then developed a distal recurrent restenotic lesion.
Attempts to deliver a stent to a distal lesion across torturous proximal lesions should have three typical components:
- Guiding catheter. An adequate guiding catheter should always be selected for lesions of expected tortuosity that will provide adequate force to drive the device (balloon or stent) across the tortuosity. It can be an extra back-up guiding catheter for the left coronary system or an AL1 or AL2 catheter for the right coronary artery. Other sophisticated-shaped catheters exist and should match the vessel anatomy. A Shepherd Crook RCA may present a unique challenge that should be handled with a specifically designed catheter. The selection of the guiding catheter is sometimes the most important decision taken at the early stages of the procedure, before difficulties are encountered.
- Wire crossing. Crossing the lesion with a wire is the next challenge in a case of proximal tortuosity. I would often select one of the soft and flexible wires to cross the lesion and secure a distal wire across it. A second, stiffer wire can be used to cross the lesion after the first wire has been secured. A Wiggle Wire (ACS/Guidant, Santa Clara, Calif.), or a Platinum Plus wire can be used for cases in which excessive tortuosity is expected with or without a previously positioned Buddy Wire.2 These wires offer a pathway to avoid vessel tortuosity, with partial straightening of the artery for better passage of the stent delivery system. I would typically use the stiff wire to perform predilatation with the balloon, and then try to cross it over the same stiff wire with one of the better third-generation stents.
Wire technology has silently progressed in tandem with progress in stent technology. The wires in our facility’s arsenal offer unique features for crossing tortuous vessels, using special design aspects and unique superglide coatings to provide optimal performance. It is the interplay between the flexibility and smoothness of the tip, with the stiffness of the proximal portion of the wire, that determines its performance in these difficult cases. We need to learn to recognize the unique features of each of our tools so as to maximize their performance.
- Stent selection. Stent selection is highly important in these cases. The most important features here are the system flexibility and the smoothness of the stent surface over the balloon. Stents that have minimal flare-up of the stent struts upon bending typically perform best in such cases. Longer stents have a tendency to “lock” over bends, particularly if flaring up of the stent struts occurs while the stent bends. This “locking” can be released by gentle motion and steady gentle force on the stent. Sometimes pulling the wire slightly can lead to release of that lock. Shorter stents generally behave more favorably over longer stents in tortuous vessels. Use of the Buddy Wire is recommended in cases where problems may be identified in advance and in cases where the initial crossing with a stent over a single wire has failed.
The case presented here shows how the selection of an adequate wire and stent resulted in successful delivery and deployment of a stent.
In cases where severe tortuosity and stent delivery problems are anticipated, I would not select a drug-eluting stent today, since they lack the advanced mechanical properties shared by some of the modern bare-metal stents. Future developments of drug-eluting stents will undoubtedly place them in the same mechanical categories as the third-generation bare-metal stents available today.
Proper stent delivery technique is also extremely important. Operator patience is required when faced with a stent that does not cross a tortuous segment. Long-term gentle force may often lead to success in cases where difficulties are encountered. Extreme force should be avoided and may cause complications such as stent loss and vessel damage. Most importantly, the limits of the procedure should be recognized in time so that the procedure can be stopped safely without major complications. Primum Non-Nocere is the sacred motto in the catheterization laboratory!
Summary. This case demonstrates that PCI is often challenged by mechanical factors related to vessel tortuosity, calcifications and prior proximal stenting. Optimal selection of an appropriate guiding catheter, wire and stent often results in mechanical success, which is the fist step towards procedural and long-term clinical success.
References
- Simons AJ and Caputo RP. Successful placement of a stent in a previously treated un-stentable vessel segment made possible by the ACS Hi-Torque Wiggle Wire: A case report. J Invas Cardiol 2004;16:29–31.
- Aude YW, et al. Combination wiggle wire, “Buddy” wire technique for stent delivery in calcified tortuous coronary arteries. Am J Cardiol 2001;88:42.
