

Stingray Balloon Used in Slender Percutaneous Coronary Intervention for Chronic Total Occlusion
ABSTRACT: Slender chronic total occlusion (CTO) percutaneous coronary intervention (PCI) using 5 Fr radial Ikari catheter is possible in simple CTO cases. We report a case where we initially thought the LAD CTO was short and easy, but we found that the CTO had a considerable amount of calcium and also some tortuosity, making simple wire crossing impossible. We used a Stingray balloon to perform re-entry by tracking the balloon over an Ultimate Bros 3 gram wire using an extension wire. We successfully punctured into true lumen and completed stenting through a slender 5 Fr system. This case demonstrates the beauty of combining the advances in CTO PCI from the East and the West together and also demonstrates the possibility of using the Stingray system in a 5 Fr guiding catheter.
J INVASIVE CARDIOL 2013;25(7):E155-E158
Key words: chronic total occlusion
____________________________________
The use of 5 Fr transradial percutaneous coronary intervention (PCI) is increasing in our center and it is not unusual to proceed with 5 Fr PCI even in chronic total occlusion (CTO) lesions if the operator judges the CTO to be easy with a high chance of single antegrade wire crossing. We describe a case where the operator (EBW) misjudged a short mid-left anterior descending (LAD) CTO to be “easy” and during 5 Fr CTO PCI found significant tortuosity and calcification within the short-segment CTO. By using the Bridgepoint Stingray balloon (Boston Scientific Corporation) through a slender 5 Fr system, the operator was able to complete the CTO PCI. The stingray system can extend the CTO complexity in 5-Fr compatible CTO PCI.
Case Report. A 58-year-old gardener with a past history of smoking, hypertension, and hyperlipidemia was admitted with chest pain, anterolateral ST depression, and a small troponin leak. Coronary angiography was performed through a 5 Fr right radial approach and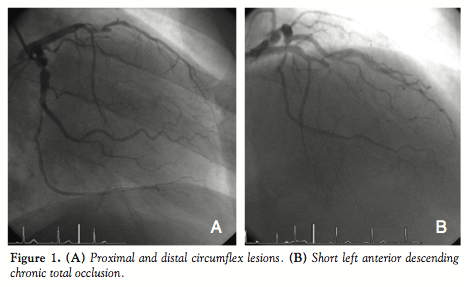 showed 90% stenosis in the proximal circumflex artery, 80% stenosis in the distal circumflex, and 100% short-segment CTO in the mid-left anterior descending (LAD) artery (Figure 1). Although the CTO was calcified, it was deemed to be short and therefore a slender PCI approach was taken.
showed 90% stenosis in the proximal circumflex artery, 80% stenosis in the distal circumflex, and 100% short-segment CTO in the mid-left anterior descending (LAD) artery (Figure 1). Although the CTO was calcified, it was deemed to be short and therefore a slender PCI approach was taken.
A 5 Fr Ikari left 3.5 guiding catheter (Terumo Corporation) was used1 to engage the left main. After stenting was performed to the circumflex artery with excellent angiographic results, a Fielder XT wire (Asahi Intecc Co, Ltd) with a Corsair microcatheter (Asahi Intecc Co, Ltd) was used to approach the CTO. Usually, it is highly desirable to place a contralateral catheter for retrograde injection even when antegrade contrast filling seems adequate, as in this case. As often occurs when antegrade wiring begins, the antegrade collaterals may diminish and retrograde opacification of the distal vessel will allow accurate re-entry into the distal lumen and reduce the risk of extensive subintimal dissection. However, in this case, the operator deemed the CTO to be extremely easy and thus started an antegrade attempt without the use of contralateral injection. After a short while, the XT wire was unable to penetrate into the lesion due to calcification. An Ultimate Bros 3 gram wire (Asahi Intecc Co, Ltd) was used, but it went into the subintimal space distal to the distal cap of the CTO. At this point, the operator realized that there was also a significant bend at the CTO in the LAD and in order to re-enter the true distal lumen, the CTO wire would have to make a large turn. After several minutes of wire manipulation, it was clear that no currently available wire would be able to make this turn. At this point, the placement of a contralateral catheter was considered again, but antegrade injection showed if anything an improvement in antegrade collateral flow. Using the wire position relative to the distal lumen contrast, the operator felt that it was possible to put a Stingray balloon over the wire and puncture in the direction of the contrast and gain re-entry into the true distal lumen.
Although the Stingray balloon is 6 Fr compatible according to the product manual, the authors of this paper had previously made measurements to the balloon and deemed that it could pass through a 5 Fr Ikari Catheter. Therefore, the Corsair catheter was pushed forward into the calcified CTO to create a space for the Stingray balloon. An extension wire (Asahi Intecc Co, Ltd) was connected to the Ultimate Bros 3 gram wire and the Corsair catheter was removed and exchanged with the Stingray balloon in its place (Figure 2A). The Stingray balloon was deliberately placed at the most proximal part of the distal cap in order to make a re-entry puncture that minimized the subintimal segment. We will discuss the reasons for this in the discussion later. Perhaps due to the smaller size of the subintimal space generated by the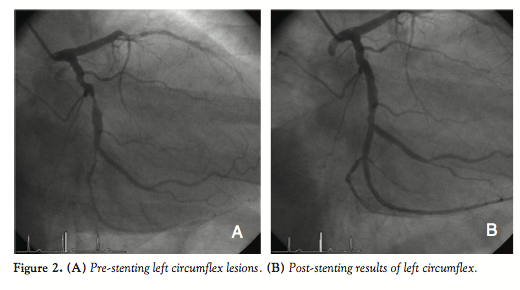 Corsair compared to the CrossBoss catheter, or perhaps because of the heavy calcification, the Stingray’s balloon wings did not fill well with contrast. However, from previous angiography, it was clear that the distal true lumen lied underneath the Ultimate Bros 3 wire and slightly toward the septal side of it. Therefore, the Stingray CTO re-entry guidewire (Boston Scientific) was used to puncture inferiorly and a Pilot 150 wire (Abbott Vascular) was used to follow this tract into the distal LAD. After using an extension wire to remove the Stingray balloon, antegrade contrast injection confirmed the wire position (Figure 2B). Since the 5 Fr system only allowed for long wire removal of the over-the-wire Stingray balloon, great care had to be taken not to lose the wire position during backing out of the Stingray balloon or exchanging the Corsair catheter. The Corsair catheter was then passed into the distal LAD and a Rinalto wire (Asahi Intecc Co, Ltd) was placed instead of the Pilot 150. A 2.5
Corsair compared to the CrossBoss catheter, or perhaps because of the heavy calcification, the Stingray’s balloon wings did not fill well with contrast. However, from previous angiography, it was clear that the distal true lumen lied underneath the Ultimate Bros 3 wire and slightly toward the septal side of it. Therefore, the Stingray CTO re-entry guidewire (Boston Scientific) was used to puncture inferiorly and a Pilot 150 wire (Abbott Vascular) was used to follow this tract into the distal LAD. After using an extension wire to remove the Stingray balloon, antegrade contrast injection confirmed the wire position (Figure 2B). Since the 5 Fr system only allowed for long wire removal of the over-the-wire Stingray balloon, great care had to be taken not to lose the wire position during backing out of the Stingray balloon or exchanging the Corsair catheter. The Corsair catheter was then passed into the distal LAD and a Rinalto wire (Asahi Intecc Co, Ltd) was placed instead of the Pilot 150. A 2.5 x 15 mm Apex Balloon (Boston Scientific) was used to predilate the lesion and a 3.0 x 38 mm Promus Element stent was placed to cover the CTO lesion. After postdilatation, this produced a marvelous angiographic result (Figure 3).
x 15 mm Apex Balloon (Boston Scientific) was used to predilate the lesion and a 3.0 x 38 mm Promus Element stent was placed to cover the CTO lesion. After postdilatation, this produced a marvelous angiographic result (Figure 3).
Discussion. CTO intervention has developed in leaps and bounds in the past decade. The Japanese introduced retrograde CTO PCI2 and intravascular ultrasound-guided reverse CART3 and thereby improving success rates of CTO PCI dramatically.4 The increasing popularity of transradial intervention5,6 and the smaller body habitus of Asian patients have led to the development of “slender PCI” in Japan.7 With the increasing advances in wire technology and the introduction of Fielder XTA, Gaia First, and Gaia Second wires (Asahi Intecc Co, Ltd), single-wire antegrade success is increasing. Therefore, it is now usual to perform CTO PCI with a 5 Fr guiding catheter system in Asia, where these wires are available. In the West, the development of the Bridgepoint re-entry devices, such as the Stingray balloon,8 has improved CTO PCI success.9 In the United States, the combination of using dual injection, bilateral femoral approach, rapid switching between antegrade and retrograde approach, and the use of Bridgepoint devices has given rise to a new algorithm for CTO with improved success rates.10 The Bridgepoint system is usually used with an 8 Fr femoral approach. In Japan, there is almost a rejection of the United States methods and the Bridgepoint devices. Some of the resistance to the Bridgepoint devices comes from the concern with creating longer then necessary subintimal segments and the need for 8 Fr catheters. Of course, the retrograde reverse CART technique also produces long subintimal segments, but the length of these segments is minimized in classic retrograde reverse CART.
in Asia, where these wires are available. In the West, the development of the Bridgepoint re-entry devices, such as the Stingray balloon,8 has improved CTO PCI success.9 In the United States, the combination of using dual injection, bilateral femoral approach, rapid switching between antegrade and retrograde approach, and the use of Bridgepoint devices has given rise to a new algorithm for CTO with improved success rates.10 The Bridgepoint system is usually used with an 8 Fr femoral approach. In Japan, there is almost a rejection of the United States methods and the Bridgepoint devices. Some of the resistance to the Bridgepoint devices comes from the concern with creating longer then necessary subintimal segments and the need for 8 Fr catheters. Of course, the retrograde reverse CART technique also produces long subintimal segments, but the length of these segments is minimized in classic retrograde reverse CART.
Our case demonstrates that the Stingray re-entry balloon and wire can be used in a manner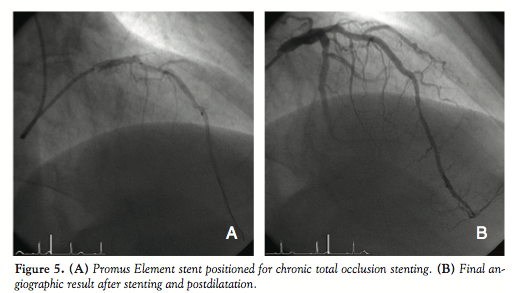 that does not extend the subintimal segment length and can also be used in conjuncture with a 5 Fr transradial “slender” system. We hope that this demonstration relieves some of the resistance against Bridgepoint devices and CTO operators can add this useful device into the armament in the fight against CTO.
that does not extend the subintimal segment length and can also be used in conjuncture with a 5 Fr transradial “slender” system. We hope that this demonstration relieves some of the resistance against Bridgepoint devices and CTO operators can add this useful device into the armament in the fight against CTO.
Conclusions. We reported a case of 5 Fr transradial slender PCI of LAD CTO using the Stingray re-entry system. This is the first demonstration of the 5 Fr compatibility of the Stingray system and represents taking the best of the CTO developments in the East and the West; by combining these advantages, we can achieve successful PCI of CTOs quickly, elegantly, and slenderly.
From the 1Department of Medicine and Therapeutics, Prince of Wales Hospital, Chinese University Hong Kong, Hong Kong and 2the Department of Cardiovascular Medicine, Tokai University School of Medicine, Kanagawa, Japan.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Ikari holds the patent for the Ikari catheter; Dr Wu reports travel expenses paid by Innotronik to learn about the BridgePoint.
Manuscript submitted January 9, 2013, provisional acceptance given January 22, 2013, final version accepted February 11, 2013.
Address for correspondence: Dr E.B. Wu, Department of Medicine and Therapeutics, Prince of Wales Hospital, Ngan Shing Rd, Shatin, Hong Kong. Email: ebwu@netvigator.com
References
- Ikari Y, Nakajima H, Iijima R, et al. Initial characterization of Ikari guide catheter for transradial coronary intervention. J Invasive Cardiol. 2004;16(2):65-68.
- Surmely JF, Katoh O, Tsuchikane E, Nasu K, Suzuki T. Coronary septal collaterals as an access for the retrograde approach in the percutaneous treatment of coronary chronic total occlusions. Catheter Cardiovasc Interv. 2007;69(6):829-832.
- Rathore S, Katoh O, Tsuchikane E, Oida A, Suzuki T, Takase S. A novel modification of the retrograde approach for the recanalization of chronic total occlusion of the coronary arteries intravascular ultrasound guided reverse controlled antegrade and retrograde tracking. JACC Cardiovasc Interv. 2010;3(2):155-164.
- Morino Y, Kimura T, Hayashi Y, et al; J-CTO Registry Investigators. In-hospital outcomes of contemporary percutaneous coronary intervention in patients with chronic total occlusion insights from the J-CTO registry (multicenter CTO registry in Japan). JACC Cardiovasc Interv. 2010;3(2):143-151.
- Gilchrist IC. Transradial catheterization’s grass roots epidemic. JACC Cardiovasc Interv. 2010;3(10):1032-1034.
- Bertrand OF, Rao SV, Pancholy S, et al. Transradial approach for coronary angiography and interventions: results from the first international transradial practice survey. JACC Cardiovasc Interv. 2010;3(10):1022-1031.
- Masutani M, Yoshimachi F, Matsukage T, Ikari Y, Saito S. Use of slender catheters for transradial angiography and interventions. Indian Heart J. 2008;60(1 Suppl A):A22-A26.
- Werner GS, Schofer J, Sievert H, Kugler C, Reifart NJ. Multicentre experience with the BridgePoint devices to facilitate recanalisation of chronic total coronary occlusions through controlled subintimal re-entry. Eurointervention. 2011;7(2):192-200.
- Whitlow PL, Burke MN, Lombardi Wl, et al. FAST-CTOs Trial Investigators. Use of a novel crossing and re-entry system in coronary chronic total occlusions that have failed standard crossing techniques: results of the FAST-CTOs (Facilitated Antegrade Steering Technique in Chronic Total Occlusions) trial. JACC Cardiovasc Interv. 2012;5(4):393-401.
- Brilakis ES, Grantham JA, Rinfret S, et al. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5(4):367-379.
_______________________________
From the 1Department of Medicine and Therapeutics, Prince of Wales Hospital, Chinese University Hong Kong, Hong Kong and 2the Department of Cardiovascular Medicine, Tokai University School of Medicine, Kanagawa, Japan.
Disclosure: The authors have completed and returned the ICMJE Form for Dis- closure of Potential Conflicts of Interest. Dr Ikari holds the patent for the Ikari catheter; Dr Wu reports travel expenses paid by Innotronik to learn about the BridgePoint. Manuscript submitted January 9, 2013, provisional acceptance given January 22, 2013, final version accepted February 11, 2013.
Address for correspondence: Dr E.B. Wu, Department of Medicine and Ther- apeutics, Prince of Wales Hospital, Ngan Shing Rd, Shatin, Hong Kong. Email: ebwu@netvigator.com

