

Safety and Efficacy of the Frontrunner XP Catheter for Recanalization of Chronic Total Occlusion of the Femoropopliteal Arteries
Abstract: Objective. The purpose of this study was to examine the safety and efficacy of the Frontrunner XP CTO (chronic total occlusion) catheter (Cordis Corporation) for recanalization of CTO of femoropopliteal arteries. Methods. A retrospective analysis of consecutive patients with critical limb ischemia (CLI) who underwent femoropopliteal angioplasty for TransAtlantic Inter-Society Consensus (TASC) class D lesions between 2009 and 2011 was performed. Twenty-two patients were enrolled with a mean age of 58.9 ± 11.5 years. Patients were enrolled with totally occluded arteries (mean occlusion length, 18.0 ± 10.1 cm) that were treated with the Frontrunner XP CTO catheter. All lesions were complex (TASC D) and 86.4% of the lesions were mildly calcified. A Frontrunner catheter was used to treat 22 CTOs after guidewire failure. Results. Twenty-two of the 33 cases (66.7%) had failed previous attempts of percutaneous intervention with conventional guidewire. The Frontrunner catheter was used to treat 22 CTOs after guidewire failure. The Frontrunner catheter successfully facilitated the placement of a guidewire into the distal true lumen in 21 cases (95.5%). Thrombolysis in Myocardial Infarction 3 flow was achieved in all target vessels after further balloon angioplasty or stenting. Conclusions. The Frontrunner XP CTO catheter is safe and effective for successful recanalization of CTO of femoropopliteal arteries and it should be an alternative method after guidewire failure.
J INVASIVE CARDIOL 2013;25(7):344-347
Key words: chronic total occlusions, recanalization, percutaneous transluminal angioplasty, fluoroscopy
_______________________________________
A particularly challenging condition for percutaneous transluminal angioplasty (PTA) is chronic total occlusions (CTOs). CTOs are one of the primary causes of procedural failure in peripheral interventions.1-4
On the other hand, endovascular therapy for complex lesions of the superficial femoral and popliteal artery remains controversial. The TransAtlantic Inter-Society Consensus (TASC; 2000 and 2007) document was published to propose treatment strategies and recommendations for the management of peripheral arterial disease. As per recommendation, TASC A lesions are most suitable for an endovascular procedure, whereas surgery is recommended primarily for TASC D lesions. The TASC document clearly states that more evidence is needed to make firm recommendations about the role of PTA for TASC B and C lesions.3,5,6
Percutaneous negotiation of a guidewire, either intraluminally or subintimally, should be done to recanalize the CTO successfully. However, percutaneous recanalization of long CTOs of the femoropopliteal artery by anterograde methods, using a guidewire and catheter, has only moderate success rates (40%-60%) depending on lesion length, calcification, operator experience, and run-off vessels; negotiation failures lead to failure of CTO recanalization.7 Therefore, other methods that can enhance the success rate of guidewire negotiation, whether intraluminally or subintimally, are needed.
Since Tønnesen et al first reported the utility of retrograde popliteal access two decades ago; this approach has been employed in challenging femoropopliteal interventions.8-13 Currently, retrograde subintimal tracking via the popliteal approach, which utilizes the anatomical characteristics of the femoropopliteal artery, delivers an endovascular solution for unsuccessful anterograde CTO crossings.14
The purpose of this study was to determine the safety and efficacy of the Frontrunner XP CTO catheter (FR-XP; Cordis Corporation) for recanalization of CTO of femoropopliteal arteries after guidewire failure. The FR-XP catheter is a blunt microdissection device that takes advantage of the elastic properties of adventitia versus inelastic properties of fibrocalcific plaque to create fracture planes. This technique may be advantageous in penetrating hard fibrous caps and creating a passage through the CTOs.
Methods
Patient selection and study population. The study was performed as a retrospective, non- randomized, single-center study and was approved by the local institutional review board. A total of 22 patients with angiographically documented CTOs in the femoropopliteal arteries were enrolled between 2009 and 2011. At least a 6-month history of symptoms was presented for endovascular therapy. Standard guidewire recanalization failed due to calcified lesions in a total of 22 patients (mean age, 58.9 ± 11.5 years), who were then treated with the FR-XP catheter (Figure 1). As per Fontaine Classification, 10 of these patients (45.5%) had intermittent claudication (Stage IIb), 4 patients (18.2%) had rest pain, and 8 patients (36.4%) had ischemic ulcers. Twenty patients had lesions in the superficial femoral artery (SFA), and 2 patients had a lesion in the popliteal artery. The mean occlusion length was 18.0 ± 10.1 cm and 86.4% of the lesions were mildly calcified.
randomized, single-center study and was approved by the local institutional review board. A total of 22 patients with angiographically documented CTOs in the femoropopliteal arteries were enrolled between 2009 and 2011. At least a 6-month history of symptoms was presented for endovascular therapy. Standard guidewire recanalization failed due to calcified lesions in a total of 22 patients (mean age, 58.9 ± 11.5 years), who were then treated with the FR-XP catheter (Figure 1). As per Fontaine Classification, 10 of these patients (45.5%) had intermittent claudication (Stage IIb), 4 patients (18.2%) had rest pain, and 8 patients (36.4%) had ischemic ulcers. Twenty patients had lesions in the superficial femoral artery (SFA), and 2 patients had a lesion in the popliteal artery. The mean occlusion length was 18.0 ± 10.1 cm and 86.4% of the lesions were mildly calcified.
The Frontrunner XP CTO catheter. The FR-XP catheter (Figure 2) was originally designed for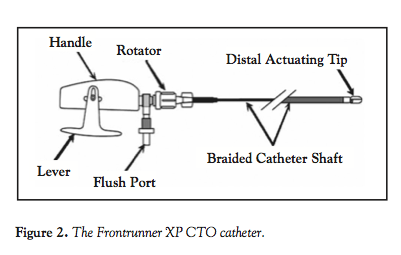 use in coronary arteries. More recently, the device has been increasingly used to facilitate guidewire placement across peripheral CTOs. The FR-XP catheter is used in combination with the Frontrunner Micro Guide catheter (MGC; Cordis Corporation), which provides additional support for the device and acts as a conduit for more rapid wire exchange after crossing of the CTO. The Frontrunner catheter consists of a handle assembly with an integral rotator and a flush port for internal device flushing, a proximal braided shaft for push and torque control, and a flexible distal shaft that may be manually shaped. The radio-opaque, blunt-shaped, distal actuating tip is comprised of a set of bilateral hinged pieces. The device has a 6 Fr profile; blunt microdissection creates an intraluminal pathway through a CTO, enabling guidewire placement in the distal true lumen. The catheter does not have a guidewire lumen.
use in coronary arteries. More recently, the device has been increasingly used to facilitate guidewire placement across peripheral CTOs. The FR-XP catheter is used in combination with the Frontrunner Micro Guide catheter (MGC; Cordis Corporation), which provides additional support for the device and acts as a conduit for more rapid wire exchange after crossing of the CTO. The Frontrunner catheter consists of a handle assembly with an integral rotator and a flush port for internal device flushing, a proximal braided shaft for push and torque control, and a flexible distal shaft that may be manually shaped. The radio-opaque, blunt-shaped, distal actuating tip is comprised of a set of bilateral hinged pieces. The device has a 6 Fr profile; blunt microdissection creates an intraluminal pathway through a CTO, enabling guidewire placement in the distal true lumen. The catheter does not have a guidewire lumen.
The Micro Guide catheter. The MGC with a hydrophilic coating is recommended for use with the FR-XP and is designed to provide additional support to the distal portion of the FR-XP. After crossing the occlusion with the FR-XP, the MGC may be used to facilitate placement of a guidewire across the lesion.
Procedure. Informed written consent was obtained from all patients before treatment. The procedure was performed under local anesthesia, and for all patients, access was obtained with an anterograde or retrograde approach via the ipsilateral or contralateral common femoral artery. Subsequently, all patients received 3000-6000 IU of heparin intra-arterially as per body weight.
After initial angiographic imaging, the CTO was crossed with a 0.035˝ hydrophilic guidewire (Terumo). When guidewire advancement could not be achieved into the CTO despite several attempts, the Frontrunner catheter was used to facilitate the intraluminal negotiation of the guidewire. After jaw opening and closing, and passage through the proximal cap of the CTO,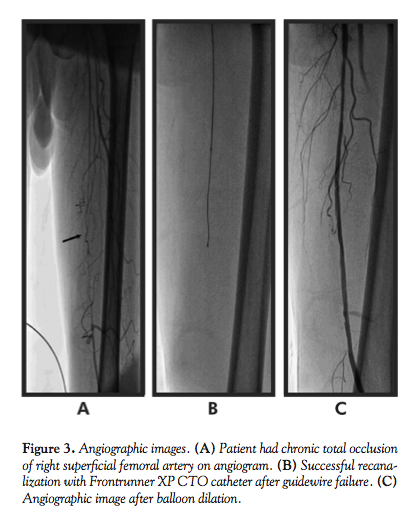 the Frontrunner microtome was navigated forward through the occluded segments with its jaws closed. Then, to create a larger microdissection canal, the Frontrunner catheter was repeatedly pulled back with an “open jaw.” The Frontrunner catheter was crossed within 2 minutes in all target vessels. Fluoroscopic roadmapping was used throughout to verify the alignment of the catheters with the vessel lumen. After the initial passage of the Frontrunner catheter, it was advanced into the distal reconstituted artery and used for guidewire introduction. Balloon angioplasty or adjunctive stenting was performed after guidewire introduction (Figure 3).
the Frontrunner microtome was navigated forward through the occluded segments with its jaws closed. Then, to create a larger microdissection canal, the Frontrunner catheter was repeatedly pulled back with an “open jaw.” The Frontrunner catheter was crossed within 2 minutes in all target vessels. Fluoroscopic roadmapping was used throughout to verify the alignment of the catheters with the vessel lumen. After the initial passage of the Frontrunner catheter, it was advanced into the distal reconstituted artery and used for guidewire introduction. Balloon angioplasty or adjunctive stenting was performed after guidewire introduction (Figure 3).
Postprocedural treatment. During the intervention, all patients received 3000-6000 IU of unfractionated heparin intra-arterially; after treatment, intravenous heparin was administered at 4000–5000 IU subcutaneously every 12 hours for 2 days. On discharge, a lifetime regimen of oral acetylsalicylic acid (150 mg/day) and 4-week course of clopidogrel (75 mg/day) were initiated.
Results
The Frontrunner catheter was used in 22 patients. The overall technical success rate was 95.5%. Nineteen patients (86.4%) had lesions in the superficial femoral artery (SFA), and 2 patients (9.1%) had a lesion in the popliteal artery. The mean occlusion length was 18.0 ±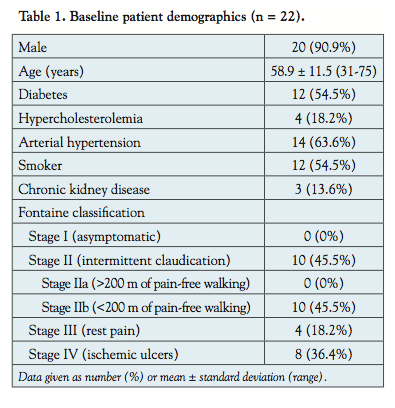 10.1 cm. All lesions were considered complex (TASC D), and 86.4% of the lesions were mildly calcified. Diabetes was present in 12 patients (54.5%) and 14 patients (63.6%) had arterial hypertension. All baseline patient demographics and femoropopliteal lesion characteristics are summarized in Tables 1 and 2, respectively.
10.1 cm. All lesions were considered complex (TASC D), and 86.4% of the lesions were mildly calcified. Diabetes was present in 12 patients (54.5%) and 14 patients (63.6%) had arterial hypertension. All baseline patient demographics and femoropopliteal lesion characteristics are summarized in Tables 1 and 2, respectively.
Twenty-two of the 33 cases (66.7%) had failed previous attempts of percutaneous intervention with conventional guidewires. The Frontrunner catheter was used to treat 22 CTOs after guidewire failure. The Frontrunner catheter successfully facilitated the placement of the guidewire into the distal true lumen in 21 cases (95.5%). TIMI 3 flow was achieved in all target vessels after further balloon angioplasty or stenting.
Discussion
Chronic occlusions account for a significant portion of peripheral vascular lesions and have historically represented a serious technical challenge to endovascular interventionalists using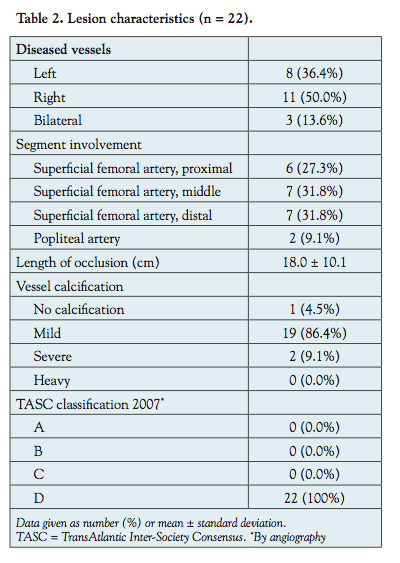 conventional guidewires and catheters.15 Currently, endovascular methods are used increasingly as the initial approach for treating femoropopliteal disease, since they have been shown to result in lower morbidity and mortality compared to bypass surgery.16
conventional guidewires and catheters.15 Currently, endovascular methods are used increasingly as the initial approach for treating femoropopliteal disease, since they have been shown to result in lower morbidity and mortality compared to bypass surgery.16
Subintimal recanalization with distal reentry, known as percutaneous intentional extraluminal recanalization (PIER), has been advocated in recent years as a solution to the problem of unsuccessful pass through multisegmental, long, calcified occlusions. London et al reported a 90% technical success rate for SFA subintimal angioplasty in a series of patients with a mean occlusion length of 15 cm.17 This approach, however, has been limited in some cases by the lack of controlled reentry into the true lumen of the target vessel. Additionally, true lumen reentry using hydrophilic wires and catheters is not achieved until subintimal passage to a site significantly remote from the level of vessel lumen patency, causing subintimal angioplasty or stenting to extend beyond the occluded segment.
The Frontrunner catheter, a relatively new device, is thought to selectively cause disruption of plaques and the adventitia and is designed to improve the technical success of traversing complex lesions. To date, however, recanalization success with this new device and the impact of the technology are unknown for peripheral arteries, and it has not been tested in large trials or randomized studies. This paper reports a single-center experience with the Frontrunner-XP in revascularization of complex femoropopliteal arterial occlusions (TASC D lesions). In our study, 22 patients with CTOs of femoropopliteal arteries were enrolled after intraluminal guidewire failure. The indications for treatment were severe claudication, pain at rest, and minor trophic changes of the limb. Primary endpoints of the study were immediate technical and clinical success. In our study, the success rate using the Frontrunner catheter was 95.5%. Although the number of patients was small and calcium in the lesions was not assessed, our study included only patients with failure of guidewire advancement into the CTO.
The FR-XP is a blunt microdissection device that takes advantage of the elastic properties of adventitia versus the inelastic properties of fibrocalcific plaque to create fracture planes. This technique may be advantageous in penetrating hard fibrous caps of SFA occlusions. The device separates atherosclerotic plaque in various tissue planes, creating a passage through the CTO.
Study limitations. Some limitations of the present study need to be addressed. First, this study included only a small number of patients. Second, this study was not randomized and no matched subintimal (PIER) or retrograde-treated occlusions via popliteal access were available for comparison. Third, there was a bias in patient selection since FR-XP recanalization was performed only in patients in whom intraluminal guidewire recanalization failed. However, this bias was unfavorable for the FR-XP group, since it included more difficult cases with longer and older occlusions. Thus, the bias in patient selection does not weaken, but rather strengthens, the results of our study.
Conclusion
Frontrunner XP CTO catheters are safe and effective for successful revascularization of CTO of femoropopliteal arteries. They may facilitate crossing complex calcified CTOs in the peripheral arteries. Although the study sample was small, appropriate use of these approaches appears to be safe and effective after failed recanalization of CTOs of the femoropopliteal arteries by conventional methods using guidewires and angiographic catheters.
References
- Kjellgren O, Feld S, Loyd D, Schroth G, Anderson HV, Smalling RW. Successful treatment of chronic total peripheral occlusions that failed conventional techniques using the stiff backend of the Glidewire. Cathet Cardiovasc Diagn.1995;36(4):360-363.
- Gupta AK, Ravimandalam K, Rao VR, et al. Total occlusion of iliac arteries: results of balloon angioplasty. Cardiovasc Intervent Radiol. 1993;16(3):165-177.
- Bolia A, Miles KA, Brennan J, Bell PR. Percutaneous transluminal angioplasty of occlusions of the femoral and popliteal arteries by subintimal dissection. Cardiovasc Intervent Radiol.1990;13(6):357-363.
- Henry M, Amor M, Ethevenot G, Henry I, Mentre B, Tzvetanov K. Percutaneous endoluminal treatment of iliac occlusions: long-term follow-up in 105 patients. J Endovasc Surg.1998;5(3):228-235.
- Bolia A, Brennan J, Bell PR. Recanalisation of femoro-popliteal occlusions: improving success rate by subintimal recanalisation. Clin Radiol.1989;40(3):325.
- Ingle H, Nasim A, Bolia A, et al. Subintimal angioplasty of isolated infragenicular vessels in lower limb ischemia: long-term results.J Endovasc Ther. 2002;9(4):411-416.
- van der Heijden FH, Eikelboom BC, Banga JD, Mali WP. Management of superficial femoral artery occlusive disease. Br J Surg.1993;80(8):959-963.
- Tonnesen KH, Sager P, Karle A, Henriksen L, Jorgensen B. Percutaneous transluminal angioplasty of the superficial femoral artery by retrograde catheterization via the popliteal artery. Cardiovasc Intervent Radiol.1988;11(3):127-131.
- Zaitoun R, Iyer SS, Lewin RF, Dorros G. Percutaneous popliteal approach for angioplasty of superficial femoral artery occlusions. Cathet Cardiovasc Diagn. 1990;21(3):154-158.
- Heenan SD, Vinnicombe SJ, Buckenham TM, Belli AM. Percutaneous transluminal angioplasty by a retrograde subintimal transpopliteal approach. Clin Radiol. 1994;49(11):824-827; discussion 827-828.
- Villas PA, Cohen G, Goyal A, Putnam SG 3rd, Ball D. The merits of percutaneous transluminal angioplasty of a superficial femoral artery stenosis via a retrograde popliteal artery approach.J Vasc Interv Radiol.1999;10(3):325-328.
- Yilmaz S, Sindel T, Ceken K, Alimoglu E, Luleci E. Subintimal recanalization of long superficial femoral artery occlusions through the retrograde popliteal approach. Cardiovasc Intervent Radiol.2001;24(3):154-160.
- Cutress ML, Blanshard K, Shaw M, Bown M, White S, Sayers RD. Retrograde subintimal angioplasty via a popliteal artery approach. Eur J Vasc Endovasc Surg. 2002;23(3):275-276.
- Spinosa DJ, Harthun NL, Bissonette EA, et al. Subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) for subintimal recanalization to treat chronic critical limb ischemia. J Vasc Interv Radiol.2005;16(1):37-44.
- Etezadi V, Benenati JF, Patel PJ, Patel RS, Powell A, Katzen BT. The reentry catheter: a second chance for endoluminal reentry at difficult lower extremity subintimal arterial recanalizations.J Vasc Interv Radiol. 2010;21(5):730-734.
- Dalman RL, Taylor LM Jr. Basic data related to infrainguinal revascularization procedures. Ann Vasc Surg.1990;4(3):309-312.
- London NJ, Srinivasan R, Naylor AR, et al. Subintimal angioplasty of femoropopliteal artery occlusions: the long-term results. Eur J Vasc Surg.1994;8(2):148-155.
From 1KMC, Manipal, Karnataka, India, 2Sahajanand Medical Tech Pvt Ltd, Surat, Gujarat, India, and 3MCOAHS, Manipal, Karnataka, India.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 6, 2013, and accepted April 3, 2013.
Address for correspondence: Ranjan K. Shetty, MBBS, MD, DM, Associate Professor, Department of Cardiology, KMC, Manipal-576104, Karnataka, India. Email: ranjanshettyk@yahoo.com

