

Recurrent Cardiovascular Events with Paclitaxel-Eluting Versus Bare-Metal Stents in Saphenous Vein Graft Lesions: Insights from the SOS (Stenting of Saphenous Vein Grafts) Trial
ABSTRACT: The Stenting of Saphenous Vein Grafts (SOS) trial demonstrated a reduction in clinical and angiographic adverse events with paclitaxel-eluting stents (PES) compared to bare-metal stents (BMS) in saphenous vein graft (SVG) lesions, but the rate of recurrent adverse events has not been described. Methods. We performed a post hoc, landmark analysis to evaluate the risk of event recurrence following a non-fatal initial event among the SOS trial patients (pts). Results. During a median follow-up of 35 months, the 80 pts enrolled in SOS experienced a total of 78 major cardiovascular events (MACE): 51 in the BMS group and 27 in PES group. No MACE were found in 28 pts (35%) while 52 pts (65%) had at least one event. The initial event was death in 13 pts (16%). Among the 39 pts whose initial event was not fatal, 12 (31%) had one or more subsequent MACE (50% of which were definitely related to the study SVG). The mean and median number of MACE per patient was significantly higher in patients receiving BMS versus PES (1.3 ± 1.2 and 1 ± 1.26 versus 0.6 ± 0.7 and 1 ± 0.825, p = 0.005 and p = 0.008, respectively). The rate of a second MACE following an initial event was 17% in the PES group and 37% in the BMS group (p = 0.24). Ten of 12 pts with recurrent events had received a BMS (83%). Conclusion. Pts undergoing SVG stenting had a high rate of recurrent events after an initial non-fatal event. These events were often related to the target vessel and most occurred in pts who had received a BMS, further supporting the benefit of PES over BMS in SVG lesions.
J INVASIVE CARDIOL 2011;23:216–219
_____________________________________
Patients undergoing saphenous vein graft (SVG) stenting are at high risk for subsequent major adverse cardiac events (MACE). However the event types and rates of recurrent events have received limited study.1 Most studies reporting clinical outcomes after SVG stenting report the time to first event, at which time patients are censored; subsequent events are not included in the analyses, although they may have important clinical implications.1
The Stenting of Saphenous Vein Grafts (SOS) trial (NCT00247208) demonstrated that implantation of paclitaxel-eluting stents (PES) improved angiographic and long-term clinical outcomes compared to bare-metal stents (BMS).2–6 The goal of the present study was to examine the rate and etiology of recurrent MACE in the SOS trial.
Methods
The study design and primary results of the SOS trial have previously been published.2,3,6 Briefly, 80 patients with SVG lesions were randomized to receive a PES or BMS to test the hypothesis that PES implantation in SVG lesions would reduce angiographic restenosis at 12-month follow-up. PES were associated with lower rates of angiographic restenosis, and lower incidence of adverse clinical events as well during a median follow-up of 18 months.2 The benefit was sustained at 35 months.4 In this report, in addition to the incidence of all cause and cardiac death, we analyzed both incident and recurrent myocardial infarction (MI), target vessel revascularization (TVR), target lesion revascularization (TLR), target lesion failure and MACE. All analyses, including the determination of whether an event was related to the target SVG, were blinded to study arm allocation.
Landmark analyses were used to evaluate the risk of major cardiovascular event recurrence following a non-fatal initial event. Using this analytic method, time-to-event was calculated from the time of the initial event. The incidence of adverse events was calculated using the Kaplan-Meier method and comparison between groups was performed using the log-rank test. Continuous variables were reported as mean ± standard deviation or median and compared using the student’s t-test or Wilcoxon rank-sum test. Discrete variables were reported as frequencies and compared using the Pearson Chi-square test. All tests were 2-sided; a p-value < 0.05 was considered significant. Statistical analysis was performed with SPSS Version 18.0 (SPSS Inc., Chicago, Illinois) and JMP 8 (SAS Institute Inc., Cary, North Carolina). The SOS study was approved by the institutional review board of each participating study center, and all patients provided written informed consent.
Results
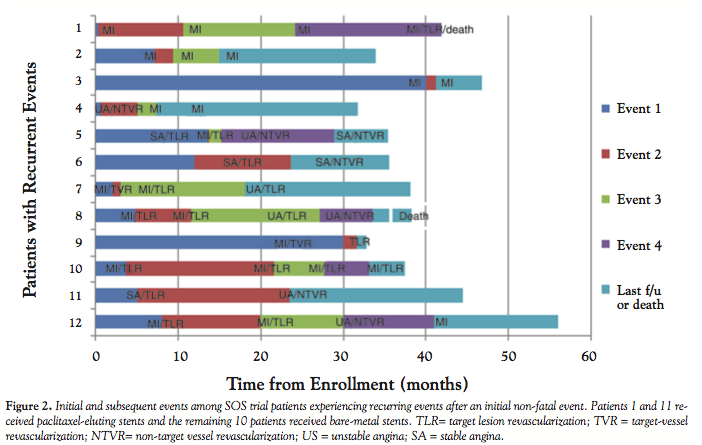
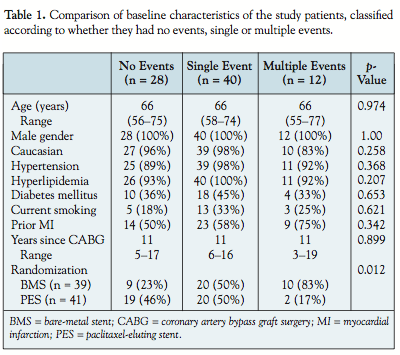
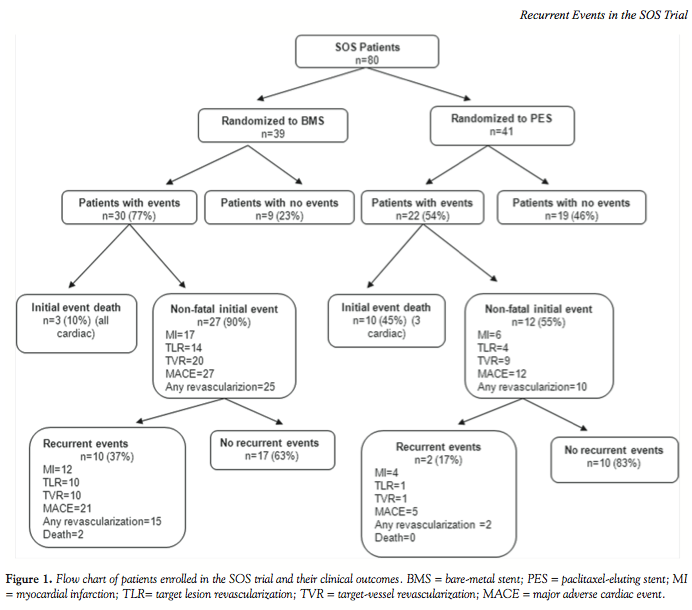 During a median follow-up of 35 months, 52 of the 80 patients (65%) enrolled in the SOS trial experienced at least one adverse cardiovascular event (Figure 1). Fifteen patients died; 13 of those deaths occurred as the initial adverse cardiovascular event. Of the 39 patients who had at least one non-fatal event, 12 (31%) had one or more subsequent major cardiovascular events (total, 26 events; Figure 2). The baseline characteristics of patients who experience zero, one, or multiple events were similar (Table 1). Patients with multiple events were more likely to have received a BMS. The mean and median number of major cardiovascular events per patient was significantly higher in patients receiving BMS versus PES (1.3 ± 1.2 and 1 ± 1.26 vs. 0.6 ± 0.7 and 1 ± 0.825, p = 0.005 and p = 0.008, respectively). The baseline characteristics of patients with at least one non-fatal event were similar between PES and BMS-treated patients.
During a median follow-up of 35 months, 52 of the 80 patients (65%) enrolled in the SOS trial experienced at least one adverse cardiovascular event (Figure 1). Fifteen patients died; 13 of those deaths occurred as the initial adverse cardiovascular event. Of the 39 patients who had at least one non-fatal event, 12 (31%) had one or more subsequent major cardiovascular events (total, 26 events; Figure 2). The baseline characteristics of patients who experience zero, one, or multiple events were similar (Table 1). Patients with multiple events were more likely to have received a BMS. The mean and median number of major cardiovascular events per patient was significantly higher in patients receiving BMS versus PES (1.3 ± 1.2 and 1 ± 1.26 vs. 0.6 ± 0.7 and 1 ± 0.825, p = 0.005 and p = 0.008, respectively). The baseline characteristics of patients with at least one non-fatal event were similar between PES and BMS-treated patients.
 Overall, 20 patients (16 in BMS arm and 4 in PES arm) underwent TLR during follow-up. Most patients who received a BMS at baseline received a DES at follow-up (14/16, 88%). Embolic protection devices were utilized in 5/20 TLRs (25%).
Overall, 20 patients (16 in BMS arm and 4 in PES arm) underwent TLR during follow-up. Most patients who received a BMS at baseline received a DES at follow-up (14/16, 88%). Embolic protection devices were utilized in 5/20 TLRs (25%).
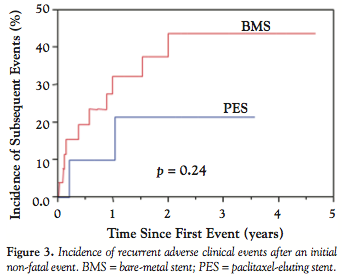 Using the landmark survival analysis method, during a median follow-up of 25 months after the first adverse event, a subsequent MACE occurred in 12 patients (31%); 10 (37%) in the BMS group versus 2 (17%) in the PES group (p = 0.24) (Figure 3). At least one of those events was definitely related to the target SVG in 6 patients, and was not related in 3 patients; its relationship to the target SVG could not be determined in 3 patients (Figure 2). The recurrent MACE were related to the target SVG in 48% of BMS versus 20% of PES patients, and were not related to the target SVG in 24% of BMS versus 20% of PES patients. The relationship to the target SVG could not be determined in 28% of the BMS versus 60% of the PES patients (p = 0.386).
Using the landmark survival analysis method, during a median follow-up of 25 months after the first adverse event, a subsequent MACE occurred in 12 patients (31%); 10 (37%) in the BMS group versus 2 (17%) in the PES group (p = 0.24) (Figure 3). At least one of those events was definitely related to the target SVG in 6 patients, and was not related in 3 patients; its relationship to the target SVG could not be determined in 3 patients (Figure 2). The recurrent MACE were related to the target SVG in 48% of BMS versus 20% of PES patients, and were not related to the target SVG in 24% of BMS versus 20% of PES patients. The relationship to the target SVG could not be determined in 28% of the BMS versus 60% of the PES patients (p = 0.386).
 There were 26 subsequent MACE that occurred after an initial event; 11 out of these 26 recurrences (42%) were definitely related to the target SVG. Twenty-two of the 26 recurrent events (85%) presented as acute coronary syndromes.
There were 26 subsequent MACE that occurred after an initial event; 11 out of these 26 recurrences (42%) were definitely related to the target SVG. Twenty-two of the 26 recurrent events (85%) presented as acute coronary syndromes.
Discussion
The main findings of our study are: 1) patients undergoing SVG stenting who have a first adverse event have a high incidence of recurrent MACE that commonly manifest as acute coronary syndromes; 2) recurrent events are often related to the vein graft that was originally stented; and 3) recurrent events are more likely to occur in patients who receive BMS than DES.
Patients undergoing SVG stenting are known to be at high risk for subsequent events. Annual mortality has been reported as high as 11% in such patients.7 In addition, there is a high risk for non-fatal MI and TVR.1 Our study adds to the current body of knowledge by demonstrating that SVG percutaneous coronary intervention patients often have multiple MACE, during a median follow-up of nearly 3 years. Most clinical trial primary endpoint analyses are based on time to first cardiovascular event analyses, ignoring or censoring events occurring subsequent to the first event.8 Yet, such events can be associated with significant morbidity and mortality, making their analysis important, although they may also magnify the apparent benefit of more effective therapy, since patients who suffer an initial event have increased risk for more events, especially in the early period after the first event.8
Patients who require percutaneous coronary intervention after having undergone coronary artery bypass graft surgery are generally relatively old, and often have multiple comorbidities.9 Such patients may die for reasons other than their coronary anatomy. Indeed, many patients in the SOS trial died of non-cardiac causes.4 The present study suggests, however, that recurrent events are often due to target SVG failure. Therefore, efforts to prevent SVG failure may be important not only early, but also late after SVG stenting.
The efficacy and safety of DES in SVGs is still being debated. Although 8 meta-analyses10–17 and one systematic review1 were published in 2010, all demonstrating benefit with DES implantation, most of the data included in those meta-analyses came from retrospective registry studies. The only two prospective, randomized-controlled trials of DES in SVGs have shown conflicting results. In the RRISC trial, there was a similar need for TVR among patients receiving DES and BMS, and yet there was a higher mortality with DES at a median follow-up of 32 months.7 In contrast, the SOS trial demonstrated a significant reduction in TLR and MI, with a similar mortality, among patients receiving a PES versus BMS during a median follow-up of 35 months.4 In the present SOS trial subanalysis, most recurrent events occurred in patients who had initially received a BMS, further supporting a benefit of PES in SVG lesions. Currently DES are utilized in the majority of SVG interventions in the US, suggesting that interventionalists perceive DES to be beneficial in this setting.9 Whether the divergent results of RRISC and SOS are related to the type of stent used (sirolimus-eluting in RRISC versus paclitaxel-eluting in SOS) remains an area of active investigation.18 Three large multicenter, randomized-controlled trials are currently examining the role of DES in SVGs.1,19 In addition, stenting of intermediate SVG lesions might prevent their progression to symptoms, as was shown in the Moderate Vein Graft Lesion Stenting with the Taxus Stent and Intravascular Ultrasound (VELETI) trial;20 such a strategy is currently being examined in the 450-patient multicenter VELETI II trial (NCT01223443). Medical therapy with aspirin, aggressive low-density lipoprotein cholesterol lowering,21 and possibly high-density lipoprotein cholesterol raising (e.g., using niacin, as is currently being evaluated in the Atherosclerosis Lesion Progression Intervention using Niacin Extended Release in Saphenous Vein Grafts trial; NCT01221402) is also being examined for the prevention and treatment of SVG disease.
Our study has important limitations. The etiology and frequency of recurrent adverse events was a non-prespecified, post hoc analysis of the SOS trial, and included a small number of patients. All study patients were men, and even though gender differences are unlikely to contribute to the findings of this study, extrapolation of the results to women should be done with caution.
In summary, in this post hoc analysis of the SOS trial, a high rate of recurrent cardiac events was seen. These events were often related to the initially stented SVG and occurred in patients who received BMS more often than in patients receiving PES.
References
- Brilakis ES, Saeed B, Banerjee S. Drug-eluting stents in saphenous vein graft interventions: A systematic review. EuroIntervention 2010;5:722–730.
- Brilakis ES, Lichtenwalter C, de Lemos JA, et al. A randomized controlled trial of a paclitaxel-eluting stent versus a similar bare-metal stent in saphenous vein graft lesions the SOS (Stenting of Saphenous Vein Grafts) trial. J Am Coll Cardiol 2009;53:919–928.
- Lichtenwalter C, de Lemos JA, Roesle M, et al. Clinical presentation and angiographic characteristics of saphenous vein graft failure after stenting: Insights from the SOS (Stenting of Saphenous Vein Grafts) trial. JACC Cardiovasc Interv 2009;2:855–860.
- Brilakis ES, Lichtenwalter C, Abdel-karim AR, et al. Continued benefit from paclitaxel-eluting compared to bare-metal stent implantation in saphenous vein graft lesions during long-term follow-up of the SOS (Stenting of Saphenous Vein Grafts) trial. JACC Cardiovasc Interv 2011;4:176–182.
- Michael TT, Badhey N, Banerjee S, Brilakis ES. Comparison of characteristics and outcomes of saphenous vein graft patients who were vs. those who were not enrolled in the stenting of saphenous vein grafts randomized controlled trial. J Investig Med 2011;59:259–266.
- Badhey N, Lichtenwalter C, de Lemos JA, et al. Contemporary use of embolic protection devices in saphenous vein graft interventions: Insights from the stenting of saphenous vein grafts trial. Catheter Cardiovasc Interv 2010;76:263–269.
- Vermeersch P, Agostoni P, Verheye S, et al. Increased late mortality after sirolimus-eluting stents versus bare-metal stents in diseased saphenous vein grafts: Results from the randomized DELAYED RRISC trial. J Am Coll Cardiol 2007;50:261–267.
- Nissen SE. Cardiovascular outcomes in randomized trials: Should time to first event for “hard” endpoints remain the standard approach? J Am Coll Cardiol 2009;54:2363–65.
- Brilakis ES, Wang TY, Rao SV, et al. Frequency and predictors of drug-eluting stent use in saphenous vein bypass graft percutaneous coronary interventions: A report from the American College of Cardiology National Cardiovascular Data CathPCI Registry. JACC Cardiovasc Interv 2010;3:1068–1073.
- Lee MS, Yang T, Kandzari DE, et al. Comparison by meta-analysis of drug-eluting stents and bare-metal stents for saphenous vein graft intervention. Am J Cardiol 2010;105:1076–1082.
- Meier P, Brilakis ES, Conti R, et al. Drug-eluting versus bare-metal stent for treatment of saphenous vein grafts: A meta-analysis. PLoS One 2010;5:E11040.
- Joyal D, Filion KB, Eisenberg MJ. Effectiveness and safety of drug-eluting stents in vein grafts: A meta-analysis. Am Heart J 2010;159:159–169; E4.
- Sanchez-Recalde A, Valero SJ, Moreno R, et al. Safety and efficacy of drug-eluting stents versus bare-metal stents in saphenous vein grafts lesions: A meta-analysis. EuroIntervention 2010;6:149–160.
- Testa L, Agostoni P, Vermeersch P, et al. Drug-eluting stents versus bare-metal stents in the treatment of saphenous vein graft disease: A systematic review and meta-analysis. EuroIntervention 2010;6:527–536.
- Hakeem A, Helmy T, Munsif S, et al. Safety and efficacy of drug-eluting stents compared with bare-metal stents for saphenous vein graft interventions: A comprehensive meta-analysis of randomized trials and observational studies comprising 7,994 patients. Catheter Cardiovasc Interv 2011;77:343–355.
- Paradis JM, Belisle P, Joseph L, et al. Drug-eluting or bare-metal stents for the treatment of saphenous vein graft disease: A Bayesian meta-analysis. Circ Cardiovasc Interv 2010;3:565–576.
- Wiisanen ME, Abdel-Latif A, Mukherjee D, Ziada KM. Drug-eluting stents versus bare-metal stents in saphenous vein graft interventions: A systematic review and meta-analysis. JACC Cardiovasc Interv 2010;3:1262–1273.
- Lee MS, Hu PP, Aragon J, et al. Comparison of sirolimus-eluting stents with paclitaxel-eluting stents in saphenous vein graft intervention (from a Multicenter Southern California Registry). Am J Cardiol 2010;106:337–341.
- Brilakis ES, Berger PB. Should bare-metal or drug-eluting stents be used during PCI of saphenous vein graft lesions: Waiting for Godot? Catheter Cardiovasc Interv 2008;72:815–818.
- Rodes-Cabau J, Bertrand OF, Larose E, et al. Comparison of plaque sealing with paclitaxel-eluting stents versus medical therapy for the treatment of moderate nonsignificant saphenous vein graft lesions. The Moderate Vein Graft Lesion Stenting with the Taxus Stent and Intravascular Ultrasound (VELETI) pilot trial. Circulation 2009;120:1978–1986.
- Brilakis ES, de Lemos JA, Cannon CP, et al. Outcomes of patients with acute coronary syndrome and previous coronary artery bypass grafting (from the Pravastatin or Atorvastatin Evaluation and Infection Therapy [PROVE IT-TIMI 22] and the Aggrastat to Zocor [A to Z] trials). Am J Cardiol 2008;102:552–558.
_________________________________________
From the 1Veteran Affairs North Texas Healthcare System, Dallas, Texas; 2University of Texas Southwestern Medical Center, Dallas, Texas, 3Department of Internal Medicine, University of Toledo, Toledo, Ohio, 4Central Arkansas Veterans Healthcare System and University of Arkansas for Medical Sciences, Little Rock, Arkansas, 5Onassis Cardiac Surgery Center, Athens, Greece, 6Michael E. DeBakey Veterans Affairs Medical Center, Houston, Texas, 7Iowa City Veteran Affairs Medical Center, Iowa City, Iowa, 8Medical College of Wisconsin, Milwaukee, Wisconsin, and 9Geisinger Clinic, Danville, Pennsylvania.
Funding and Disclosures: The SOS trial was funded by the Department of Veterans Affairs VISN-17 Startup Award and by the Clark R. Gregg grant of the Harris Methodist Foundation to Dr. Brilakis. Dr. de Lemos reports speaker honoraria from Bristol-Myers Squibb/Sanofi-Aventis and consulting income from Johnson and Johnson (< $10,000). Dr. Obel works predominantly with cardiac rhythm devices and has speaker agreements with St. Jude, Medtronic, and Boston Scientific. Dr. Addo has served on the Speaker’s Bureau for Sanofi-Aventis, Merck-Schering, Eli Lilly and Daiichi-Sankyo. Dr. Rossen participated in multicenter clinical studies supported by Boston Scientific. Dr. Berger owns equity in Lumen, Inc. Dr. Banerjee has served on the Speakers’ Bureau for St. Jude Medical Center, Medtronic Corp., and Johnson & Johnson and has received a research grant from Boston Scientific. Dr. Brilakis reports speaker honoraria from St. Jude Medical and Terumo and research support from Abbott Vascular and Infraredx and his spouse is an employee of Medtronic.
Manuscript submitted January 10, 2011, provisional acceptance given January 24, 2011, final version accepted February 18, 2011.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Dallas VA Medical Center (111A), 4500 South Lancaster Rd., Dallas, TX 75216. Email: esbrilakis@yahoo.com
