

ADVERTISEMENT
A Rare Case of a Coronary Vascular Ring Arising from an Anomalous Single Coronary Artery
ABSTRACT: We report a rare finding of a pair of coronary artery anomalies noted on computed tomography coronary angiography in an asymptomatic 75-year-old woman. This patient had a single coronary artery that bifurcated into a left main coronary artery (with an unfavorable interarterial course) and a right coronary artery. This gave rise to a vascular ring around the atrioventricular groove. We propose that the presence of this vascular ring may have been protective against the potentially ischemic course of the single-origin coronary artery passing between the aorta and pulmonary trunk.
J INVASIVE CARDIOL 2012;24(6):E129-E130
_______________________________________
Major congenital coronary anomalies are rare, and are estimated to occur in 0.3% of the general population.1,2 In a series of over 70,000 coronary angiograms, the reported incidence of anomalous origin of the left coronary artery from the right coronary artery (RCA) was only 0.006%.1
We characterize a rare combination of coronary artery anomalies, which to our knowledge, has not been previously described. A single coronary artery originating from the right coronary sinus gives rise to a coronary vascular ring around the atrioventricular (AV) groove that subsequently supplies the RCA, left anterior descending (LAD), and left circumflex (LCx) arteries.
Case Report. In July 2006, an asymptomatic 75-year-old woman was referred for computed tomography coronary angiogram (CTCA). Her cardiac risk factors were mild hypercholesterolemia and prior cigarette smoking (quit 1981); her family history could not be known. Medical history was remarkable for hypothyroidism, pelvic fracture at age 71, and a small meningioma. Her medications and supplements included alendronate, senna, ocuvite, calcium, folic acid, vitamin C, and a multivitamin. Cardiac exam was relatively unremarkable, and ECG showed nonspecific ST-T wave abnormalities. Her total cholesterol was 215 mg/dL and LDL 145 mg/dL.
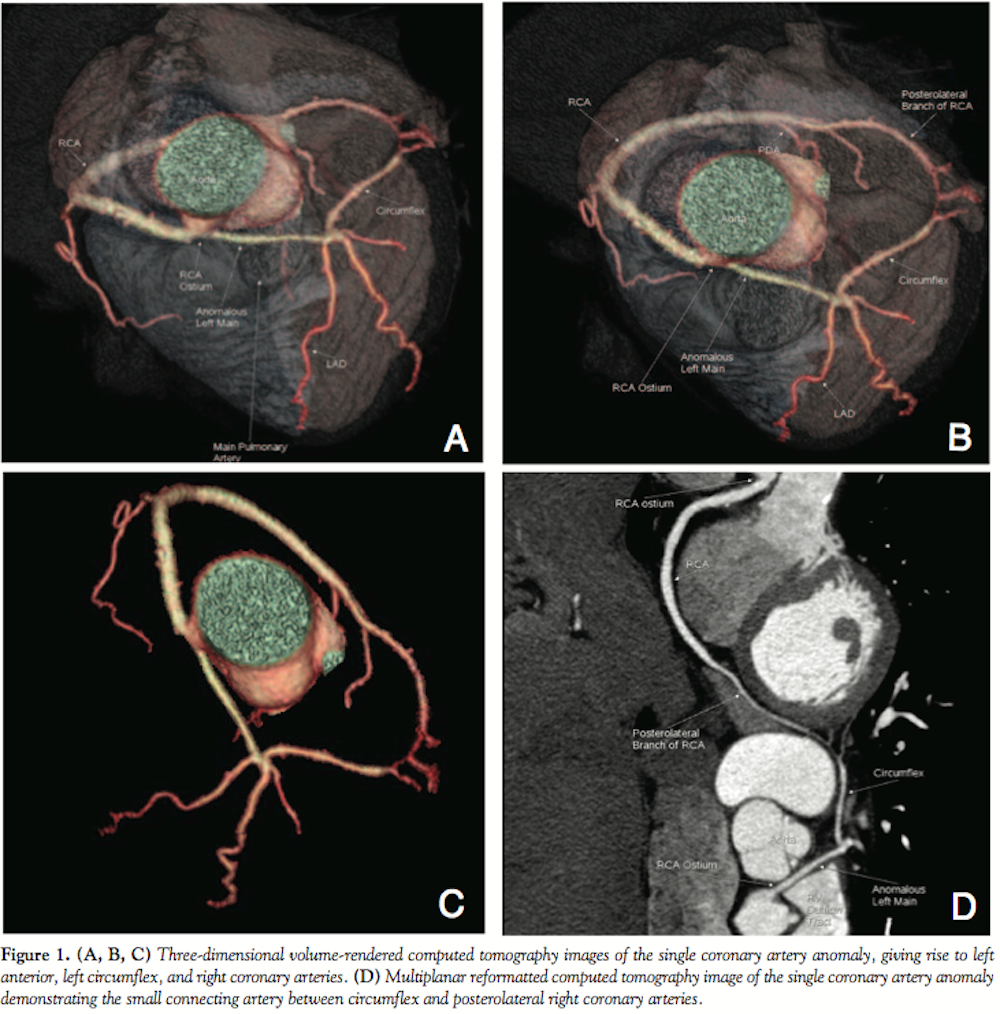 A CTCA was performed (Figure 1, Video 1). There was a single coronary artery, which arose from the right coronary sinus and bifurcated into the RCA and left main (LM) coronary artery. The RCA followed its expected course in the right AV groove. The LM coronary artery passed between the aorta and pulmonary trunk in an unfavorable configuration. At the anterior interventricular groove, the anomalous LM gave rise to the LAD and then continued to supply the LCx artery. There was an arterial conduit connecting the posterolateral RCA and LCx, which completed a ring that traversed the entire AV groove.
A CTCA was performed (Figure 1, Video 1). There was a single coronary artery, which arose from the right coronary sinus and bifurcated into the RCA and left main (LM) coronary artery. The RCA followed its expected course in the right AV groove. The LM coronary artery passed between the aorta and pulmonary trunk in an unfavorable configuration. At the anterior interventricular groove, the anomalous LM gave rise to the LAD and then continued to supply the LCx artery. There was an arterial conduit connecting the posterolateral RCA and LCx, which completed a ring that traversed the entire AV groove.
The coronary artery calcium score was 42 (50th percentile for age and gender). There was a non-obstructive (5%-15%) lesion in the proximal segment of the RCA.
Given the findings of an anomalous single coronary artery and the interarterial course of the LM coronary artery, a nuclear stress test was done. It showed no evidence of inducible ischemia.
She was treated with atorvastatin 10 mg and aspirin 81 mg. Six years later, at age 81, the patient remains asymptomatic in good health.
Discussion. Anomalous coronary arteries that originate from the opposite sinus can be differentiated by their course either around or between the aorta and right ventricular outflow tract/pulmonary trunk; the former are associated with a benign clinical course in contrast to the latter.2 Interarterial subtypes of coronary anomalies may be predisposed to ischemia secondary to exercise-induced compression between the aorta and pulmonary outflow, anatomical compression unrelated to exercise, abnormal orifice of the anomalous artery, or coronary vasospasm.3 Patients can present with signs and symptoms of cardiac ischemia, or with sudden cardiac death.4,5 It has been estimated that 14% of sudden deaths among young athletes are due to anomalous coronary arteries.6 Accordingly, the American College of Cardiology/American Heart Association guidelines have a class I recommendation for surgical revascularization where the LM coronary artery is involved, and for the RCA when it is associated with evidence of ischemia.
A congenital, abnormal communicating artery between the RCA and LCx arteries has previously been reported.7 However, to our knowledge, this is the first report of both coronary anomalies occurring in the same patient. We propose the name Ella’s Locket for this anomaly. We posit that the arterial collateral creating a coronary ring may protect against ischemia from the unfavorable, interarterial anatomy of the LM coronary artery.
Non-invasive imaging techniques including CTCA and magnetic resonance imaging can be useful in understanding coronary anomalies by allowing accurate visualization of coronary anatomy as well as their relationship to adjacent cardiac structures.8-10 Furthermore, the availability of multiple views including 3-dimensional reconstructions can aid diagnostic interpretation.9,10 In addition, the CTCA allows accurate coronary assessment while avoiding potential morbidity associated with invasive coronary imaging.
Acknowledgment. The authors wish to thank Drs. Jennifer Yu and Roxana Mehran for their assistance.
References
- Tuncer C, Batyraliev T, Yilmaz R, Gokce M, Eryonucu B, Koroglu S. Origin and distribution anomalies of the left anterior descending artery in 70,850 adult patients: multicenter data collection. Catheter Cardiovasc Interv. 2006;68(4):574-585.
- Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002;105(20):2449-2454.
- Rossi PA, Rapeport K, Fisher EA, Depasquale N. Coronary artery spasm as a cause of chest pain in a patient with anomalous origin of the right coronary artery from the left sinus of Valsalva. Tex Heart Inst J. 1988;15(2):124-127.
- Vianna CB, Gonzalez MM, Dallan LA, et al. Anomalous coronary artery causing transmural ischaemia and ventricular tachycardia in a high school athlete. Resuscitation. 2007;74(1):183-186.
- Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol. 2000;35(6):1493-1501.
- Maron BJ, Pelliccia A. The heart of trained athletes: Cardiac remodeling and the risk of sports, including sudden death. Circulation. 2006;114:1633-1644.
- Phillips DA, Berman J. A variation in the origin of the posterior descending coronary artery. Cardiovasc Intervent Radiol. 1984;7(2):75-77.
- Roncalli J, Elbaz M, Chabbert V. A rare single coronary artery with an anomalous origin of the left coronary artery from the posterior atrioventricular right coronary artery. BMJ Case Rep. 2009;2009:bcr2006095919.
- van Ooijen PM, Dorgelo J, Zijlstra F, Oudkerk M. Detection, visualization and evaluation of anomalous coronary anatomy on 16-slice multidetector-row CT. Eur Radiol. 2004;14(12):2163-2171.
- Dodd JD, Ferencik M, Liberthson RR, et al. Congenital anomalies of coronary artery origin in adults: 64-MDCT appearance. AJR Am J Roentgenol. 2007;188(2):W138-W146.
_______________________________________
From the 1Dalton School, New York, New York, 2Mount Sinai Medical Center, New York, New York, and the 3Columbia University Medical Center, New York-Presbyterian Hospital, and Advanced Cardiovascular Imaging, New York, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted December 6, 2011, provisional acceptance given January 2, 2012, final version accepted January 23, 2012.
Address for correspondence: M. Robert Peters, MD, Department of Radiology, Columbia University Medical Center, New York-Presbyterian Hospital, and Advanced Cardiovascular Imaging, New York, NY 10032. Email: petersmd@gmail.com
