

Pitfalls of Angiography in the Assessment of Atherosclerosis: The Role of Optical Coherence Tomography
Abstract: We report the case of a patient presenting with unstable angina, in whom information obtained by coronary angiography was inconclusive for the existence of a culprit lesion in the ostium of the right coronary artery. The use of optical coherence tomography was required for proper lesion assessment.
J INVASIVE CARDIOL 2012;24(5):246-247
Key words: optical coherence tomography, atherosclerosis, coronary angiography
_________________________________________
Case Report
 A 52-year-old male patient presented at the emergency department with progressive exertion dyspnea over the last 3 days. He had a history of smoking (70 pack years) and dyslipidemia treated with statins. T-wave inversion was evident at leads II, III, and aVF in the electrocardiogram, while cardiac biomarkers were negative. He was admitted to the coronary care unit and treated medically. Coronary angiography, performed 32 hours later, revealed an ostial lesion in the right coronary artery, while atheromatic disease was not
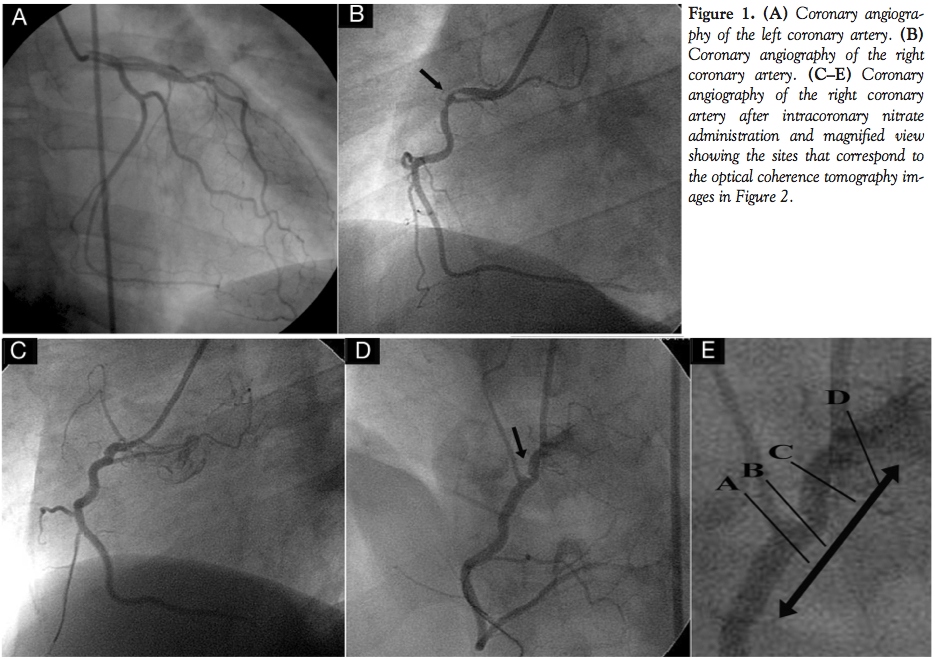
A 52-year-old male patient presented at the emergency department with progressive exertion dyspnea over the last 3 days. He had a history of smoking (70 pack years) and dyslipidemia treated with statins. T-wave inversion was evident at leads II, III, and aVF in the electrocardiogram, while cardiac biomarkers were negative. He was admitted to the coronary care unit and treated medically. Coronary angiography, performed 32 hours later, revealed an ostial lesion in the right coronary artery, while atheromatic disease was not 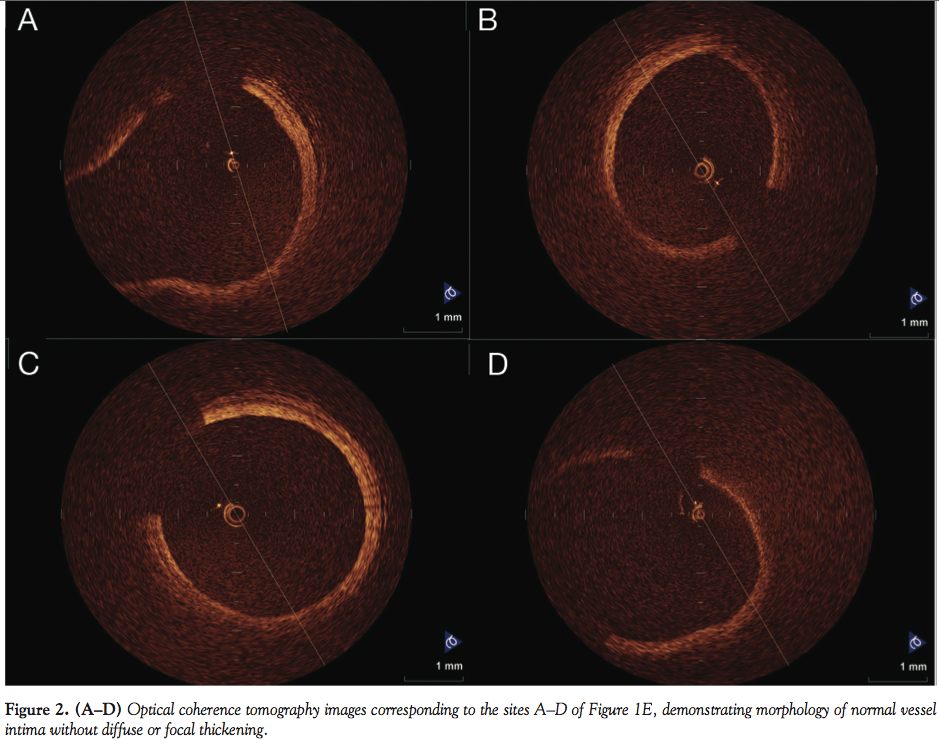 evident in the left coronary artery (Figures 1A and 1B). Coronary spasm was suspected and intracoronary nitrates were given to the patient leading to resolution of the spasm (Figures 1C and 1D). However, a focal luminal contrast deficit was still evident in the right anterior oblique view (arrow), raising the question of a significant lesion. In order to better assess the lesion morphology, we performed optical coherence tomography (OCT) examination of the lesion, using the non-occlusive image acquisition technique of the M3 Light Lab system and the LightLab OCT wire (LightLab Imaging, Inc), as previously described.1,2 Pullback of the OCT wire was performed in the proximal 25 mm of the artery as shown by the arrows (Figure 1E; sites A–D correspond to the panels of Figure 2). All acquired OCT images demonstrated morphology of normal vessel intima without diffuse or focal thickening (Figure 2). OCT study revealed no evidence of atheroma, thrombus, intimal disruption, or stenosis. However, vessel eccentricity was detected focally (Figure 2B), which probably led to the angiographic misinterpretation of luminal contrast deficit. Thus, despite being considered the golden standard for detection of coronary atherosclerosis, coronary angiography is subject to errors and misinterpretation in cases of extremely eccentric and tortuous lesions, in which invasive imaging techniques, such as optical coherence tomography, can minimize diagnostic errors.
evident in the left coronary artery (Figures 1A and 1B). Coronary spasm was suspected and intracoronary nitrates were given to the patient leading to resolution of the spasm (Figures 1C and 1D). However, a focal luminal contrast deficit was still evident in the right anterior oblique view (arrow), raising the question of a significant lesion. In order to better assess the lesion morphology, we performed optical coherence tomography (OCT) examination of the lesion, using the non-occlusive image acquisition technique of the M3 Light Lab system and the LightLab OCT wire (LightLab Imaging, Inc), as previously described.1,2 Pullback of the OCT wire was performed in the proximal 25 mm of the artery as shown by the arrows (Figure 1E; sites A–D correspond to the panels of Figure 2). All acquired OCT images demonstrated morphology of normal vessel intima without diffuse or focal thickening (Figure 2). OCT study revealed no evidence of atheroma, thrombus, intimal disruption, or stenosis. However, vessel eccentricity was detected focally (Figure 2B), which probably led to the angiographic misinterpretation of luminal contrast deficit. Thus, despite being considered the golden standard for detection of coronary atherosclerosis, coronary angiography is subject to errors and misinterpretation in cases of extremely eccentric and tortuous lesions, in which invasive imaging techniques, such as optical coherence tomography, can minimize diagnostic errors.
References
- Prati F, Cera M, Ramazzotti V, et al. From bench to bedside: a novel technique of acquiring OCT images. Circ J. 2008;72(5):839-843.
- Toutouzas K, Karanasos A, Tsiamis E, et al. New insights by optical coherence tomography into the differences and similarities of culprit ruptured plaque morphology in non-ST elevation myocardial infarction and ST-elevation myocardial infarction. Am Heart J. 2011;161(6):1192-1199.
_________________________________________
From the Department of Cardiology, Hippokration Hospital, Athens Medical School, Athens, Greece.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted November 3, 2011 and accepted December 6, 2011.
Address for correspondence: Dr Konstantinos Toutouzas, Hippokration Hospital, Athens Medical School, Dept. of Cardiology, 114 Vas. Sophias, Athens, Attiki, Greece. Email: ktoutouz@otenet.gr



