

Nitroglycerin Plus Diltiazem Versus Nitroglycerin Alone for Spasm Prophylaxis with Transradial Approach
Abstract: Objectives. The aim of this study was to compare the efficacy of nitroglycerin and diltiazem versus nitroglycerin alone in preventing radial artery spasm (RAS) during transradial coronary procedures. Background. Spasm after transradial access decreases procedural success. Multiple spasmolytics are used to prevent spasm. Individual efficacy of these agents is not conclusively established. Methods. One hundred and fifty patients undergoing coronary procedures through radial artery were enrolled and divided into two groups of 75 patients each. Patients in Group A received 200 µg nitroglycerin plus 2.5 mg diltiazem intra-arterially, and group B patients received 200 µg nitroglycerin plus placebo (saline). Blood pressure (BP) and heart rate (HR) were recorded at baseline and for 5 minutes after cocktail was given. Clinical signs of RAS, such as pain and resistance during catheter maneuver, were recorded in both groups during the procedure. Results. Systolic and diastolic BP decreased significantly in Group A compared to Group B after cocktail was given (P<.001 and P<.022, respectively). There were no significant changes of HR in either group. There was no significant difference in the incidence of clinical RAS between Group A (diltiazem plus nitroglycerin) versus Group B (nitroglycerin alone) (5% vs 7%; P=1.000). Furthermore, we found higher incidence of local burning pain in the forearm in patients that receive intra-arterial diltiazem plus nitroglycerin compared to nitroglycerin alone (21% vs 9%; P=.041). Conclusion. Diltiazem plus nitroglycerin showed no advantage compared to nitroglycerin alone in prevention of RAS in transradial approach.
J INVASIVE CARDIOL 2012;24:122–125
Key words: radial artery spasm, spasmolytic, nitroglycerin, diltiazem
_________________________________________________
The use of the transradial approach (TRA) for coronary intervention has increased tremendously over the past 5 years worldwide. It has been shown that TRA has become popular due to its lower vascular complication rates, reduced procedural costs, earlier patient mobilization, and equivalent procedural success.1-4 TRA has been shown to lower mortality in acute ST-segment elevation infarction patients.5,6
The most common complication of TRA is radial artery spasm (RAS), which can lead to serious complications and is a predictor of procedural failure.7,8 Therefore, spasmolytic cocktail is needed to prevent RAS during coronary procedures in TRA.9 In clinical practice, RAS is manifested by resistance during manipulation of intra-arterial equipment and by patient reporting pain in the forearm.10,11 RAS is observed more frequently during the early phase of operator learning curve, partly because of longer procedure duration, as well as patient and operator apprehension. Experienced operators report a low incidence of manifest RAS.
The most commonly used vasodilator cocktail consists of nitroglycerin and a calcium-channel blocker.10,12 There is uncertainty whether combination pharmacotherapy (calcium-channel blocker plus nitroglycerin) might have an advantage over single agent (nitroglycerin alone) in preventing RAS. Furthermore, diltiazem has been known to cause an uncomfortable burning sensation in the forearm. The aim of this study was to compare the efficacy of nitroglycerin and diltiazem versus nitroglycerin alone in preventing RAS during transradial coronary procedures.
Methods
This study was designed as a single-center, prospective, randomized, placebo-controlled trial (consecutive eligible patients are randomized to receive either nitroglycerin plus diltiazem or nitroglycerin plus placebo). One hundred and fifty patients were included in the study (75 patients for each group). The operators and personnel were blinded to the treatment assignment.
All eligible patients were assigned to receive 200 µg nitroglycerin plus 2.5 mg diltiazem (Group A) or 200 µg nitroglycerin plus placebo (Group B). All drugs were given intra-arterially through the radial sheath. The study protocol was approved by the local ethics committee with all patients provided written informed consent.
Patients with severe left ventricular dysfunction (left ventricular ejection fraction <30%), severe bradycardia (heart rate <40 bpm), second or third degree atrioventricular block, or hypotension (SBP <90 mm Hg) with or without cardiogenic shock were excluded.
Transradial access. All patients had a positive Allen’s test. The radial artery was punctured using either counter-puncture technique or anterior-puncture technique based on operator preference. After the insertion of a 0.025˝ guidewire, a 5 or 6 Fr short hydrophilic sheath (10 cm) was introduced into the radial artery.
Blood pressure (BP) and heart rate (HR) monitoring. Arterial BP and HR were recorded before the administration of spasmolytic cocktails and at 5 minutes after the administration of spasmolytic cocktails. Baseline BP was recorded from the manifold pressure monitoring through the radial sheath before injecting cocktails. Baseline HR was derived from the electrocardiogram monitor. After the injection of either nitroglycerin plus diltiazem or nitroglycerin plus placebo, the BP and HR were recorded continuously. The largest change was recorded.
Cocktail administration. All patients were randomized before the procedure began. Patients in Group A received 200 µg nitroglycerin in 2 mL normal saline with 2.5 mg diltiazem in 10 mL of normal saline, and Group B patients received 200 µg nitroglycerin in 2 mL saline with 10 mL saline as placebo. All drugs were given intra-arterially through the radial sheath.
Coronary procedure. Coronary angiography and percutaneous coronary intervention (PCI) were performed according to the standard techniques. A 0.035˝ x 260 cm-long guidewire was used to deliver or exchange catheters. The first choice catheter was 5 Fr Optitorque for diagnostic procedures and the Judkins Right 3.5 x 6 Fr (for right coronary artery) and EBU 3.5 x 6 Fr catheters (for left coronary artery) in all PCI cases.
All patients received intravenous unfractionated heparin 5000 IU for diagnostic procedure and 100 IU/kg if PCI was planned.
Procedural variables, including number of punctures, vasovagal reaction, procedural success, resistance during catheter maneuver, local forearm pain, and procedural time, were recorded. Demographic data were recorded.
Definitions. Primary endpoint was defined as the occurrence of RAS. Vasovagal reaction (cardioinhibitory as well as vasodepressor) was defined as symptomatic hypotension and/or bradycardia after cocktail administration, associated with nausea and/or flushing, that required additional therapy including aggressive volume repletion. Procedural success was defined as completion of the intended procedure via the initial access site. Local burning pain was defined as burning sensation experienced by the patient in the forearm that was used for the access, without the presence of catheter resistance. RAS was defined as resistance during catheter maneuver, inability to freely manipulate the catheter, and/or difficulty in removing the catheter with the presence of concomitant forearm pain during the procedure. Total procedural time was calculated from local anesthetic injection to introducer sheath removal.
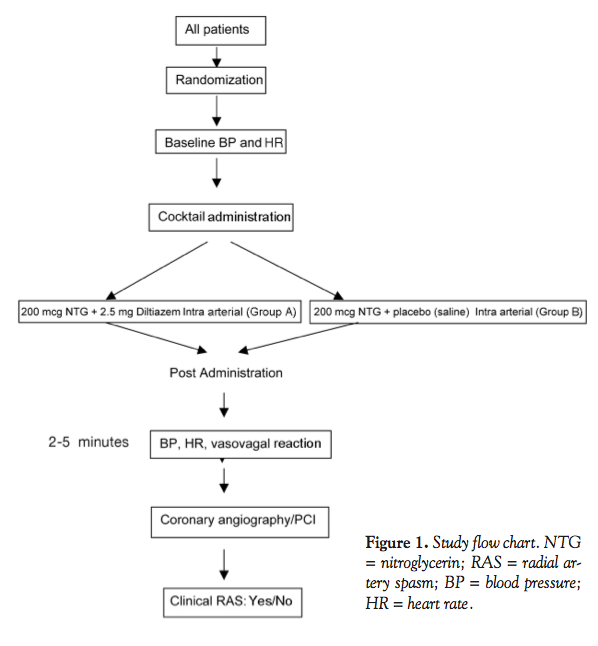 Statistical analysis. Data were expressed as mean ± standard deviation for normally distributed numeric variables, and as median (minimum-maximum) for continuous variables not fitting a normal distribution, while percentages were used for categorical variables. Chi-square test was used to compare categorical variables and student’s t-test or Mann-Whitney U-test were used to compare differences between the two groups. Using 80% study power, a minimum of 65 patients were needed in each group for evaluating an effect on the primary endpoint of RAS using a 10% incidence of RAS. A P-value of <.05 was considered statistically significant. All statistical analyses were performed using SPSS 17.0. A study flow chart can be seen in Figure 1.
Statistical analysis. Data were expressed as mean ± standard deviation for normally distributed numeric variables, and as median (minimum-maximum) for continuous variables not fitting a normal distribution, while percentages were used for categorical variables. Chi-square test was used to compare categorical variables and student’s t-test or Mann-Whitney U-test were used to compare differences between the two groups. Using 80% study power, a minimum of 65 patients were needed in each group for evaluating an effect on the primary endpoint of RAS using a 10% incidence of RAS. A P-value of <.05 was considered statistically significant. All statistical analyses were performed using SPSS 17.0. A study flow chart can be seen in Figure 1.
Results
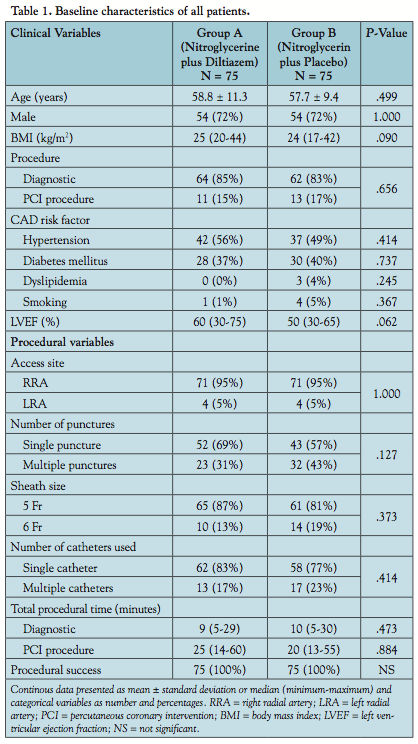 Baseline characteristics including type of procedure, access site, number of punctures, and total procedural time between the groups are shown in Table 1. There were no significant differences noted in clinical and procedural variables between the two groups.
Baseline characteristics including type of procedure, access site, number of punctures, and total procedural time between the groups are shown in Table 1. There were no significant differences noted in clinical and procedural variables between the two groups.
The differences of BP and HR between the two groups before and after cocktails are shown in Table 2. Systolic and diastolic BP decreased significantly after cocktail administration in Group A compared to Group B.
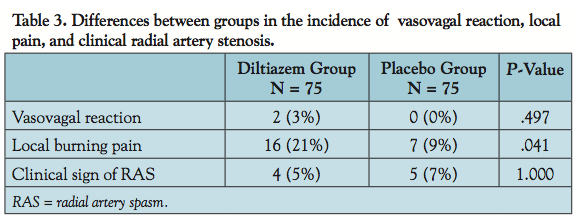
The incidence of local pain was significantly higher in the diltiazem group (P=.041). The incidences of vasovagal reaction, local pain, and clinical signs of RAS are shown in Table 3.
Discussion
 The radial artery is a muscular artery with concentric layers of smooth muscle cells (SMC) found predominant in the tunica media.15 RAS occurs due to contraction of SMC in response to activation of the predominant α-1-adrenoreceptors and, to a lesser extent, α-2-adrenoreceptors. These receptors are stimulated by circulating catecholamines and by mechanical stimuli (catheter or wire manipulation), pain sensation due to multiple punctures, or anxiety.7 The radial artery has been classified as a type III artery16 and has a higher receptor-mediated contractility (to endothelin-1 and angiotensin II),17 hence a higher risk of spasm compared to other vessels.
The radial artery is a muscular artery with concentric layers of smooth muscle cells (SMC) found predominant in the tunica media.15 RAS occurs due to contraction of SMC in response to activation of the predominant α-1-adrenoreceptors and, to a lesser extent, α-2-adrenoreceptors. These receptors are stimulated by circulating catecholamines and by mechanical stimuli (catheter or wire manipulation), pain sensation due to multiple punctures, or anxiety.7 The radial artery has been classified as a type III artery16 and has a higher receptor-mediated contractility (to endothelin-1 and angiotensin II),17 hence a higher risk of spasm compared to other vessels.
 The incidence of RAS during transradial procedures varies from 10%-12%. In current practice, intra-arterial calcium-channel blocker and nitroglycerin are the most common drug combination used to prevent RAS.10,12 Diltiazem is a high-specificity L-channel calcium blocker that inhibits the influx of extracellular calcium ions during membrane depolarization of cardiac and vascular smooth muscle, resulting in dilation of the coronary and systemic arteries, including the radial arteries.13
The incidence of RAS during transradial procedures varies from 10%-12%. In current practice, intra-arterial calcium-channel blocker and nitroglycerin are the most common drug combination used to prevent RAS.10,12 Diltiazem is a high-specificity L-channel calcium blocker that inhibits the influx of extracellular calcium ions during membrane depolarization of cardiac and vascular smooth muscle, resulting in dilation of the coronary and systemic arteries, including the radial arteries.13
Our study showed a higher incidence of local burning pain in patients who received intra-arterial diltiazem plus nitroglycerin compared to nitroglycerin alone (21% vs 9%; P=.041). This may be due to acidic pH of diltiazem solution, versus vasodilatory action causing burning pain. Diltiazem-induced vasodilatation not infrequently causes a raised urticarial rash on the flexor aspect of the forearm.
Nitroglycerin exerts its vasodilator effect through nitric oxide (NO) stimulating guanylate cyclase in the vascular smooth muscle cells.14 This study showed that there was a decrease in mean systolic and diastolic BP after nitroglycerin was given, but the decrease in BP was less compared to the group receiving both nitroglycerin and diltiazem. This is probably because of a synergistic effect of nitroglycerin and diltiazem in causing systemic vasodilatation.
Some studies have found that addition of intra-arterial diltiazem to nitroglycerin after TRA showed lower incidence of RAS,9,11 but our study did not show the advantage of adding diltiazem (5% vs 7%; P=1.000). We believe that minimal number of attempts at radial artery puncture, use of hydrophilic guidewire, use of universal catheter with fewer catheter exchanges, and short procedure duration may be responsible for a reduced tendency to develop RAS in our population, and hence no added benefit of diltiazem. When the incidence of RAS is expected to be higher, such as during the early part of the operator’s and institution’s earning curve, with an unusually anxious patient, with procedures requiring multiple catheter exchanges, or with longer procedure duration due to adverse anatomy, a calcium-channel blocker may be needed in addition to nitroglycerin.
Incidence of RAS decreases with increasing operator experience;7,18-20 procedures performed by experienced operators may be successfully completed with adequate RAS prevention provided by nitroglycerin alone.
Study limitations. Diagnosis of clinical RAS was made by the presence of resistance during catheter movement, inability to freely manipulate the catheter, and/or difficulty in removing the catheter with the presence of forearm pain during the procedure, which was subjective. To decrease the subjectivity bias, the operators were blinded to the treatment group. This sign and symptom could also be encountered with other conditions increasing resistance to catheter movement, such as atherosclerosis, vessel tortuosity, or small-caliber of the radial artery; hence, radial angiogram was performed when these problems were encountered to eliminate these anatomic reasons for resistance and pain, and angiographic presence of stenotic segments suggestive of spasm were observed. The operators in this trial were very experienced in the transradial technique and hence results of this study may not be applicable to less experienced operators.
Conclusion
Diltiazem plus nitroglycerin showed no significant advantage compared to nitroglycerin alone, as a vasodilator to prevent RAS in patients undergoing coronary procedures performed by operators with experience in the transradial approach.
Acknowledgments. We would like to acknowledge and thank Keith Fonseca, Biren Gandhi, and Yash Soni for their excellent support of the study.
References
- Hamon M, Coutance G. Transradial intervention for minimizing bleeding complications in percutaneous coronary intervention. Am J Cardiol. 2009;104(5 Suppl):55C-59C.
- Rao SV, Cohen MG, Kandzari DE, et al. The transradial approach to percutaneous coronary intervention: historical perspective, current concepts, and future directions. J Am Coll Cardiol. 2010;55(20):2187-2195.
- Rao SV, Ou FS, Wang TY, Roe MT, Brindis R, Rumsfeld JS, Peterson ED. Trends in the prevalence and outcomes of radial and femoral approaches to percutaneous coronary intervention: a report from the National Cardiovascular Data Registry. JACC Cardiovasc Interv. 2008;1(4):379-386.
- Cooper CJ, El-Shiekh RA, Cohen DJ, et al. Effect of transradial access on quality of life and cost of cardiac catheterization: a randomized comparison. Am Heart J. 1999;138(3 Pt 1):430-436.
- Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377(9775):1409-1420.
- Philippe F, Larrazet F, Meziane T, Dibie A. Comparison of transradial vs transfemoral approach in the treatment of acute myocardial infarction with primary angioplasty and abciximab. Catheter Cardiovasc Interv. 2004;61(1):67-73.
- Kiemeneij F. Prevention and management of radial artery spasm. J Invasive Cardiol. 2006;18(4):159-160.
- Hildick-Smith DJ, Lowe MD, Walsh JT, et al. Coronary angiography from the radial artery — experience, complications and limitations. Int J Cardiol. 1998;64(3):231-239.
- Kiemeneij F, Vajifdar BU, Eccleshall SC, et al. Evaluation of a spasmolytic cocktail to prevent radial artery spasm during coronary procedures. Catheter Cardiovasc Intervent. 2003;58(3):281-284.
- Coppola J, Patel T, Kwan T, et al. Nitroglycerin, nitroprusside, or both, in preventing radial artery spasm during coronary procedures. J Invasive Cardiol. 2006;18(4):155-158.
- Jia D, Zhou YJ, Shi DM, et al. Incidence and predictors of radial artery spasm during transradial coronary angiography and intervention. Chinese Med J (Engl). 2010;123(7):843-847.
- Chen CW, Lin CL, Lin TK, et al. A simple and effective regimen for prevention of radial artery spasm during coronary catheterization. Cardiology. 2006;105(1):43-47.
- Opie LH. Drugs for the Heart. Fourth ed. WB Saunders Company, Philadelphia, PA; 1997;50-79.
- Opie LH. Drugs for the Heart. Fourth ed. WB Saunders Company, Philadelphia, PA; 1997;31-46.
- McMinn RMH, Hutchings RT. A Colour Atlas of Human Anatomy. English Language Book Society/Wolfe Medical Publications Ltd, London; 1985;126-146.
- Honma S, Tokiyoshi A, Kawai K, Koizumi M, Kodama K. Radial artery running beneath the biceps tendon and its interrelation between the radial recurrent arteries. Anat Sci Intl. 2008;83(4):232-238.
- He GW, Yang CQ. Radial artery has higher receptor-mediated contractility but similar endothelial function compared with mammary artery. Ann Thorac Surg. 1997:63(5):1346-1352.
- Goldberg SL, Renslo R, Sinow R, French WJ. Learning curve in the use of the radial artery as vascular access in the performance of percutaneous transluminal coronary angioplasty. Cathet Cardiovasc Diagn. 1998;44(2):147-152.
- Louvard Y, Pezzano M, Scheers L, et al. Coronary angiography by a radial artery approach: feasibility, learning curve. One operator’s experience. Arch Mal Coeur Vaiss. 1998;91(2):209-215.
- Fukuda N, Iwahara S, Harada A, et al. Vasospasms of the radial artery after the transradial approach for coronary angiography and angioplasty. Jpn Heart J. 2004;45(5):723-731.
_________________________________________________
From the Department of Cardiovascular Sciences, Smt. N.H.L. Municipal Medical College, Sheth K.M. School of Post Graduate Medicine and Research, Sheth V.S. General Hospital and SAL Hospital and Medical Institute, TCVS Pvt. Ltd., Ahmedabad, Gujarat, India, and †Wright Center for Graduate Medical Education and the Commonwealth Medical College, Scranton, Pennsylvania.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted December 8, 2011, provisional acceptance given December 20, 2011, final version accepted January 20, 2012.
Address for correspondence: Surya Dharma, MD, Department of Cardiovascular Sciences, Smt. N.H.L. Municipal Medical College, Sheth K.M. School of Post Graduate Medicine and Research, Sheth V.S. General Hospital and SAL Hospital and Medical Institute, TCVS Pvt. Ltd., Ahmedabad, Gujarat, India. Email: drsuryadharma@yahoo.com
