

Multicenter International Registry of Unprotected Left Main Coronary Artery Percutaneous Coronary Intervention with Everolimus-Eluting Stents
Abstract: Objective. The aim of this study was to assess the clinical outcomes of percutaneous coronary intervention (PCI) with everolimus-eluting stents (EES) for the treatment of unprotected left main coronary artery (ULMCA) disease. Background. The standard of care for the treatment of ULMCA disease is coronary artery bypass grafting (CABG). Data suggest that PCI with drug-eluting stents is a viable alternative to CABG for the treatment of ULMCA disease. Randomized trials demonstrated superior event-free survival with EES compared with paclitaxel-eluting stents in non-ULMCA lesions. However, data with ULMCA PCI with EES are limited. Methods. This multicenter international registry included 178 patients from the United States, South Korea, and Italy who underwent ULMCA PCI with EES from 2008 to 2010. The primary endpoint was freedom from target lesion failure (TLF), defined as cardiac death, myocardial infarction (MI), and ischemia-driven target lesion revascularization (TLR) at 1 year. Results. At 30 days, 4 patients (2.2%) died from cardiac causes, and no patient experienced MI or TLR. One-year freedom from TLF was 94.4%. One-year freedom from cardiac death, MI, and ischemia-driven TLR was 96.6%, 98.9%, and 98.3%, respectively. Two patients (1.1%) had definite or probable stent thrombosis. Conclusion. PCI with EES is safe and effective and may be a viable option for the treatment of ULMCA disease.
J INVASIVE CARDIOL 2012;24(7):316-319
Key words: drug-eluting stents, ULMCA PCI
_________________________________________________
Coronary artery bypass graft (CABG) surgery is the standard of care for the treatment of unprotected left main coronary artery (ULMCA) disease, and percutaneous coronary intervention (PCI) is reserved for patients who are poor surgical candidates.1 ULMCA PCI is a class IIa indication and may be considered in patients who are at low risk for procedural complications and are at increased risk of adverse surgical outcomes.2
The cobalt chromium everolimus-eluting stent (EES; XIENCE V; Abbott Vascular, also distributed as Promus; Boston Scientific) reduced the rates of angiographic and clinical restenosis, myocardial infarction (MI), and stent thrombosis compared with the paclitaxel-eluting stent (PES) in non-ULMCA lesions.3-9 We report the clinical outcomes of patients who underwent ULMCA PCI with EES in a multicenter international registry.
Methods
Baseline demographic, procedural, angiographic, and clinical outcomes data of 178 patients who underwent ULMCA PCI with EES from May 2008 to September 2010 were collected from 22 institutions. The data collected from the South Korean patients were a part of the prospective Efficacy of XIENCE/Promus versus Cypher to Reduce Late Loss after Stenting (EXCELLENT) registry (n = 139). The data collected from the University of Turin-San Giovanni Batista “Molinette” Hospital, Turin, Italy (n = 14), University of California, Los Angeles Medical Center (n = 8), and Santa Barbara Cottage Hospital (n = 8) were collected in a prospective manner. The data from the University of California, San Diego Medical Center (n = 9) were collected retrospectively. Institutional review board approval was obtained at each institution to obtain patient data.
ULMCA PCI was performed using standard techniques. All patients received at least 300 mg of aspirin and a 300-600 mg loading dose of clopidogrel. Heparin or bivalirudin was administered per local practice. Use of intra-aortic balloon pump counterpulsation and intravascular ultrasound was at the discretion of the operator. All patients were maintained on at least 80 mg of aspirin daily and 75 mg of clopidogrel for a minimum of 12 months after PCI.
The primary endpoint was 1-year target lesion failure (TLF), defined as the composite of cardiac death, MI, or ischemia-driven target lesion revascularization (TLR). Deaths were classified as either cardiac or non-cardiac. Death was considered cardiac unless an undisputed non-cardiac cause was identified. Myocardial infarction was diagnosed by the presence of ischemic symptoms or signs plus new significant Q waves on the electrocardiogram and/or elevation of cardiac enzymes (creatine kinase-MB elevation >3x or creatine kinase elevation >2x the upper limit of normal). Ischemia-driven TLR was defined as repeat revascularization with either PCI or CABG because of restenosis within the stent or in the 5 mm distal or proximal segments because of clinical or functional ischemia. Stent thrombosis was defined according to Academic Research Consortium criteria.21 Definite stent thrombosis occurred if angiographic or pathologic evidence of stent thrombosis occurred. Probable stent thrombosis occurred if death within 30 days of PCI or MI at any time attributable to the target vessel occurred.
Quantitative analysis of coronary angiographic images was performed at a central core laboratory (Seoul National University Hospital Cardiovascular Clinical Research Center Angiographic Core Laboratory) by specialized technicians using the Cardiovascular Angiography Analysis System (CAAS) 5.7 QCA system (Pie Medical Imaging) for automated contour detection and quantification.
Continuous variables are presented as mean ± standard deviation. Categorical variables are presented as percentages. A P-value <.05 was considered statistically significant. The SAS software, version 9.1 (SAS Institute) was used for statistical analyses.
Results
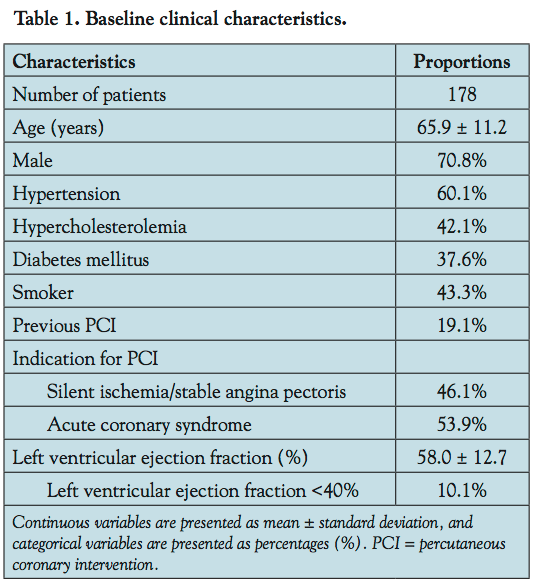
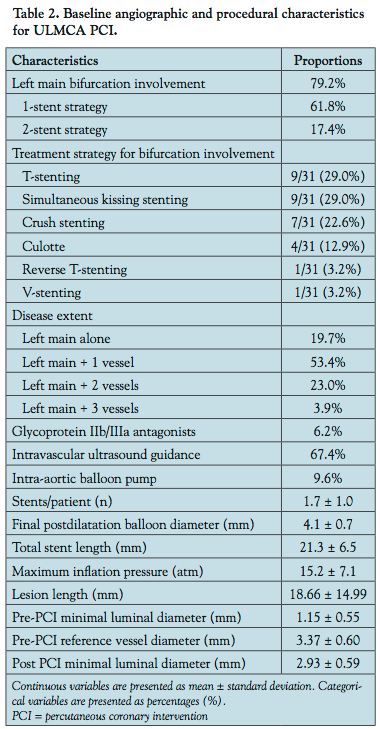
Baseline demographics of the 178 study patients are listed in Table 1. The mean age was 65.9 ± 11.2 years. Diabetes mellitus was present in 67 patients (37.6%). The distal bifurcation disease was observed in 126 patients (70.8%; Table 2). Intra-aortic balloon pump was used in 17 patients (9.6%) and intravascular ultrasound was used in 120 patients (67.4%).
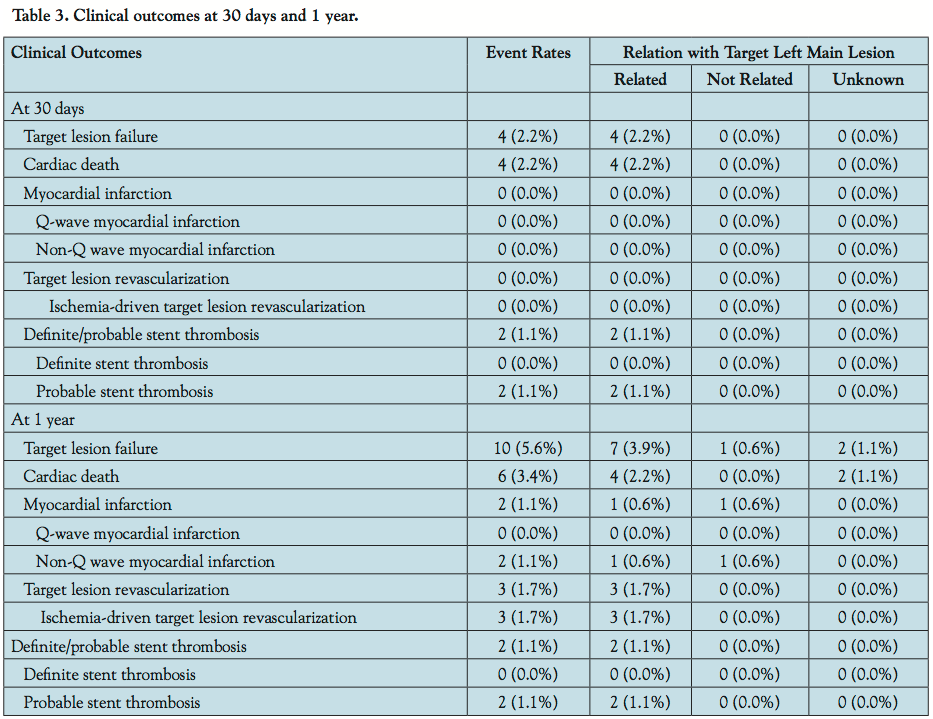
 At 30 days, TLF occurred in 4 patients (2.2%), all due to cardiac death. No patient experienced MI, ischemia-driven TLR, or stroke (Table 3). At 1 year, freedom from TLF was 94.4%. Freedom from cardiac death was 96.6%, with the majority of events occurring within the first week after PCI. Freedom from MI was 98.9%. Freedom from ischemia-driven TLR was 98.3%, with the majority of events occurring at 9 months. The 1-year rate of definite or probable stent thrombosis was 1.1%.
At 30 days, TLF occurred in 4 patients (2.2%), all due to cardiac death. No patient experienced MI, ischemia-driven TLR, or stroke (Table 3). At 1 year, freedom from TLF was 94.4%. Freedom from cardiac death was 96.6%, with the majority of events occurring within the first week after PCI. Freedom from MI was 98.9%. Freedom from ischemia-driven TLR was 98.3%, with the majority of events occurring at 9 months. The 1-year rate of definite or probable stent thrombosis was 1.1%.
 When stratified by left ventricular function, patients with left ventricular dysfunction (ejection fraction <40%) had a lower freedom from TLF at 1 year compared with patients who had left ventricular ejection fraction of ≥40% (72.2% vs 96.6%; log-rank P<.001). Patients who had a total stent length of >23 mm had a lower freedom from TLF at 1 year compared with patients with a total stent length of ≤23 mm (87.0% vs 97.0%; log-rank P=.015). Patients who had ostial or mid-shaft disease had excellent outcomes, with no TLF at 1 year. Patients with bifurcation disease who underwent PCI with a 2-stent strategy had a lower freedom from TLF compared with those who underwent PCI with a 1-stent strategy (80.7% vs 96.4%; log-rank P=.003).
When stratified by left ventricular function, patients with left ventricular dysfunction (ejection fraction <40%) had a lower freedom from TLF at 1 year compared with patients who had left ventricular ejection fraction of ≥40% (72.2% vs 96.6%; log-rank P<.001). Patients who had a total stent length of >23 mm had a lower freedom from TLF at 1 year compared with patients with a total stent length of ≤23 mm (87.0% vs 97.0%; log-rank P=.015). Patients who had ostial or mid-shaft disease had excellent outcomes, with no TLF at 1 year. Patients with bifurcation disease who underwent PCI with a 2-stent strategy had a lower freedom from TLF compared with those who underwent PCI with a 1-stent strategy (80.7% vs 96.4%; log-rank P=.003).
Cox regression analyses. Independent predictors of 1-year TLF were left ventricular ejection fraction <40% (odds ratio [OR], 9.71; 95% confidence interval [CI], 1.44-65.47; P=.02) and bifurcation stenting with 2 stents (OR, 6.34; 95% CI, 1.27-31.71; P=.03).
Discussion
The principal findings are that in patients undergoing PCI of the ULMCA, treatment with EES is safe, with low rates of cardiac death, MI, and stent thrombosis. In addition, it is effective, with low rates of ischemia-driven TLR.
The use of the EES is superior to first-generation drug-eluting stents (DESs) in non-ULMCA lesions. In the ISAR-TEST 4 substudy, which compared the EES with the sirolimus-eluting stent (SES) in non-ULMCA lesions, EES was associated with a lower binary restenosis (12.7% vs 16.9%; P=.03) and a trend toward lower TLR (9.9% vs 13.5%; relative risk, 0.73; 95% CI, 0.52-1.01; P=.06) and definite stent thrombosis (0.6% vs 1.4%; P=.17) at 2 years.10 However, it may be difficult to demonstrate a difference in restenosis between the EES and first-generation DESs because of the large-caliber vessel of the ULMCA, which requires significantly more neointimal hyperplasia compared to non-ULMCA to cause ischemia and subsequent revascularization.11
Our data compare favorably with previous studies reporting outcomes with ULMCA PCI with first-generation DESs. In the ISAR-LEFT-MAIN trial, which excluded patients with ST-elevation MI, the 1-year TLR with the SES was 7.8% and 6.5% with the PES.12 The 1-year freedom from ischemia-driven TLR was 98.3% in our study with the EES. In the DELFT registry, which is more similar to our patient population because it included patients with acute coronary syndrome who underwent urgent and emergent ULMCA PCI with PES and SES, the 1-year rates of cardiac death, MI, TLR, and major adverse cardiac events were 6.7%, 7.2%, 3.9%, and 24.3%, respectively.13 In our study, freedom from cardiac death was 96.5% and freedom from TLF was 90.7%.
Stent thrombosis in the ULMCA is likely to be catastrophic and is universally associated with death or MI given the large territory of myocardium that it supplies. Two patients (1.1%) experienced definite or probable stent thrombosis. In the ISAR-LEFT-MAIN trial, the definite stent thrombosis rate at 1 year was 0.3% with the PES and 0.7% with the SES.12 The SPIRIT IV trial reported a lower 1-year definite or probable stent thrombosis rate with the EES compared with the PES (0.3% vs 1.1%; P=.004).6 Whether this translates into lower stent thrombosis with the EES as compared with the PES in ULMCA lesions and represents a safer option remains to be seen. However, our data support the excellent safety profile with the EES after ULMCA PCI.
Study limitations. The limitations of this study included the nonrandomized design with only 1 year of follow-up. Serial troponin and creatine kinase-MB levels were not routinely drawn post PCI. Therefore, the true rate of MI is unknown. Follow-up coronary angiography was not performed in all patients. A comparative analysis with other DESs as well as CABG was not performed.
Conclusion
PCI with the EES is safe and effective and may be a viable option for the treatment of ULMCA disease.
References
- Eagle KA, Guyton RA, Davidoff R, et al; for the American College of Cardiology; American Heart Association Task Force on Practice Guidelines; American Society for Thoracic Surgery and the Society of Thoracic Surgeons. ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery). Circulation 2004;110(9):1168-1176.
- Levine GN, Bates ER, Blankenship JC, et al; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines; Society for Cardiovascular Angiography and Interventions. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58(24):E44-E122.
- Serruys PW, Ruygrok P, Neuzner J, et al. A randomized comparison of an everolimus-eluting coronary stent with a paclitaxel-eluting coronary stent: the SPIRIT II trial. EuroIntervention. 2006:2(3):286-294.
- Stone GW, Midei M, Newman W, et al; SPIRIT III Investigators. Comparison of an everolimus-eluting stent and a paclitaxel-eluting stent in patients with coronary artery disease: a randomised trial. JAMA. 2008:299(16):1903-1913.
- Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N Engl J Med. 2007;356(10):998-1008.
- Stone GW, Rizvi A, Newman W, et al; SPIRIT IV Investigators. Everolimus-eluting versus paclitaxel-eluting stents in coronary artery disease. N Engl J Med. 2010;362(18):1663-1674.
- Stone GW, Rizvi A, Sudhir K, et al; SPIRIT IV Investigators. Randomized comparison of everolimus- and paclitaxel-eluting stents. 2-year follow-up from the SPIRIT (Clinical Evaluation of the XIENCE V Everolimus Eluting Coronary Stent System) IV trial. J Am Coll Cardiol. 2011;58(1):19-25.
- Kedhi E, Joesoef KS, McFadden E, et al. Second-generation everolimus-eluting and paclitaxel-eluting stents in real-life practice (COMPARE): a randomised trial. Lancet. 2010;375(9710):201-209.
- Smits PC, Kedhi E, Royaards KJ, et al. 2-year follow-up of a randomized controlled trial of everolimus- and paclitaxel-eluting stents for coronary revascularization in daily practice. COMPARE (comparison of the everolimus eluting XIENCE-V stent with the paclitaxel eluting TAXUS LIBERTÉ stent in all-comers: a randomized open label trial). J Am Coll Cardiol. 2011;58(1):11-18.
- Byrne R. ISAR TEST 4: two-year outcomes after everolimus- or sirolimus-eluting stents in patients with coronary artery disease. Presented at: Transcatheter Cardiovascular Therapeutics 2010: September 24, 2010; Washington, DC.
- Mauri L, Orav EJ, O’Malley AJ, et al. Relationship of late loss in lumen diameter to coronary restenosis in sirolimus-eluting stents. Circulation. 2005;111(3):321-327.
- Mehilli J, Kastrati A, Byrne R, et al; for the ISAR-LEFT MAIN (Intracoronary Stenting and Angiographic Results: Drug-Eluting Stents for Unprotected Coronary Left Main Lesions) Study Investigators. Paclitaxel- versus sirolimus-eluting stents for unprotected left main coronary artery disease. J Am Coll Cardiol. 2009;53(19):1760-1768.
- Meliga E, Garcia-Garcia HM, Valgimigli M, et al; for the DELFT (drug-eluting stent for left main) Registry. Longest available clinical outcomes after drug-eluting stent implantation for unprotected left main coronary artery disease: the DELFT (drug-eluting stent for left main) registry. J Am Coll Cardiol. 2008;51(1):2212-2229.
_________________________________________________
*Joint first authors.
From the 1UCLA Medical Center, Los Angeles, California, 2Seoul National University Hospital, Seoul, South Korea, 3University of Turin-San Giovanni Batista “Molinette” Hospital, Turin, Italy, 4Seoul National University Bundang Hospital, Seongnam, South Korea, 5St Carollo Hospital, Sunchon, South Korea, 6Samsung Medical Center, Seoul, South Korea, 7Soon Chun Hyang University Cheonan Hospital, Cheonan, South Korea, 8UC San Diego Medical Center, San Diego, California, 9Santa Barbara Cottage Hospital, Santa Barbara, California, 10Cardiovascular Research Foundation, New York, New York.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Mahmud holds a grant from Abbott Corporation. Dr Stone reports Consultant positions at Osprey, Reva, Merck, Boston Scientific, Abbott Vascular, Evalve, AstraZeneca, Eli-Lilly - Daiichi Sankyo partnership, Bristol-Meyers Squibb Sanofi partnership, Otsuka, The Medicines Company, Ortho-McNeil, Gilead, InspireMD, TherOx, Atrium, Volcano, InfraReDx, Medtronic, Genentech, GlaxoSmithKlein, Miracor, MPP group, Lutonix, Velomedix, and CSI; honoraria from Edwards and Vascular Solutions; and stock and/or stock options with CoreValve, Savacor, Biostar I and II funds, MedFocus I, II and Accelerator funds, Caliber, FlowCardia, Ovalum, MediGuide, Guided Delivery Systems, Arstasis, Micardia, AccessClosure, Embrella, and VNT.
Manuscript submitted February 14, 2012, provisional acceptance given February 27, 2012, final version accepted March 12, 2012.
Address for correspondence: Hyo-Soo Kim, MD, PhD, Department of Internal Medicine and Cardiovascular Center, Seoul National University Hospital, 28 Yongon-dong Chongno-gu, Seoul 110-744, Korea. Email: hyosoo@snu.ac.kr

