

Medical Treatment Versus Angioplasty for Isolated Ostial Diagonal Stenoses: A Comparative Clinical Follow-up
Abstract: Objectives. Angioplasty of a stenosis at the ostium of a diagonal branch of the left anterior descending artery as an isolated lesion often poses a dilemma due to the risk involved in treating the lesion in comparison to the potential benefit. Therefore, we sought to investigate our experience with this issue. Methods. Between 1995 and 2010, we retrospectively analyzed 39,300 patients who underwent invasive coronary angiography in our institution. Of these, a total of 22 had an isolated diagonal stenosis. The patients were either treated conservatively or underwent angioplasty and were followed for several years. Clinical and angiographic data were compared between the two groups. Results. Thirteen of the patients were treated conservatively and 9 underwent successful PCI. Baseline characteristics did not differ between the groups. The severity of the stenosis was also similar in the two groups, but in the angioplasty group, the diameter of the vessel was significantly larger (P<.01). More patients were recatheterized during the follow-up period in the conservative arm, although this did not reach statistical difference. There was no difference in mortality between the two groups. Conclusions. Initial conservative medical approach is a reasonable approach in treating isolated diagonal ostial stenosis.
J INVASIVE CARDIOL 2012;24(5):222-223
Key words: diagonal stenosis, ostium, angioplasty, medical treatment
_________________________________________________
In patients with a significant stenosis at the origin of the diagonal branch of the left anterior descending artery (LAD), there is often deliberation as to the best mode of therapy, ie, continuing medical therapy as opposed to percutaneous coronary intervention (PCI). This has only been addressed in one previous study,1 with a relatively short period of follow-up. In addition, the patients in their study included those with non-significant coronary disease (<50% stenosis) in other vessels. We examined a group of patients with severe ostial diagonal disease as an isolated pathology in the coronary tree (entirely normal vessels apart from the diagonal lesion), and a prolonged period of follow-up.
Methods
We examined retrospectively from our database all patients undergoing coronary angiography in our department from 1995 to the present time, numbering 39,300. Of these, we identified 22 patients with a severe stenosis (≥70%) at the origin of the diagonal branch of the LAD as an isolated finding, and a diameter of above 1.5 mm. These patients constituted the study group. It should be stressed that the rest of the coronary vessels were normal. The decision as to whether to perform PCI or to continue medical therapy was made by the operator. However, patients catheterized in the context of acute myocardial infarction who were found to have single ostial diagonal disease were excluded from our assessment, as they underwent obligatory primary angioplasty.
We analyzed the background data of the patients, including demographics, clinical presentation, and angiographic findings. Follow-up was performed using our computerized database and telephone questionnaires with the family physician. Data on recatheterization were analyzed regarding the status of the disease in the diagonal and the development of new coronary lesions.
Angiography and PCI were performed using standard techniques. The assessment of degree of stenosis was based on angiographic appearance alone and as no doubt existed regarding the severity, other methods such as intravascular ultrasound (IVUS) and fractional flow reserve (FFR) were not used.
Statistical analysis. Continuous variables were analyzed with independent samples t-test. Categorical variables were analyzed using the chi-square test. A P-value less than 0.05 was defined as statistically significant. The statistical analysis was performed using an SPSS 18 statistical program.
Results
 Of the 22 patients, a total of 13 were treated conservatively (group 1) and 9 underwent successful PCI (group 2). In group 2, six patients underwent stent implantation (5 bare-metal stents and 1 drug-eluting stent) and the remaining 3 had a cutting balloon dilatation. All patients in group 2 had Thrombolysis in Myocardial Infarction (TIMI) flow grade 3 pre- and postprocedure. No patients had postprocedural residual stenosis, except for a single patient who underwent cutting balloon angioplasty, in whom a residual 10% stenosis was observed.
Of the 22 patients, a total of 13 were treated conservatively (group 1) and 9 underwent successful PCI (group 2). In group 2, six patients underwent stent implantation (5 bare-metal stents and 1 drug-eluting stent) and the remaining 3 had a cutting balloon dilatation. All patients in group 2 had Thrombolysis in Myocardial Infarction (TIMI) flow grade 3 pre- and postprocedure. No patients had postprocedural residual stenosis, except for a single patient who underwent cutting balloon angioplasty, in whom a residual 10% stenosis was observed.
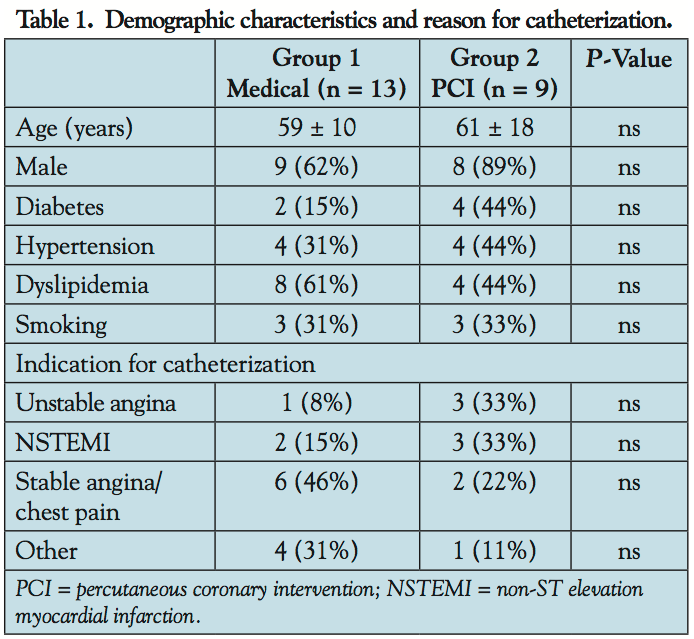
 The demographic data and the indications for catheterization did not differ between the groups (Table 1). Pre-catheterization stress testing was performed and found to be positive in 5 patients, all in group 1 (4 patients with thallium scanning and 1 with stress echocardiography).
The demographic data and the indications for catheterization did not differ between the groups (Table 1). Pre-catheterization stress testing was performed and found to be positive in 5 patients, all in group 1 (4 patients with thallium scanning and 1 with stress echocardiography).
At angiography, the culprit artery was more frequently the first diagonal (D1) in both groups (Table 2). The severity of the stenosis was also similar in the two groups, but in group 2, the diameter of the vessel was significantly larger (P<.01).
Follow-up was significantly longer in group 1 than in group 2 (6.9 ± 3.7 years vs 3.2 ± 2.1 years; P<.01; Table 3).
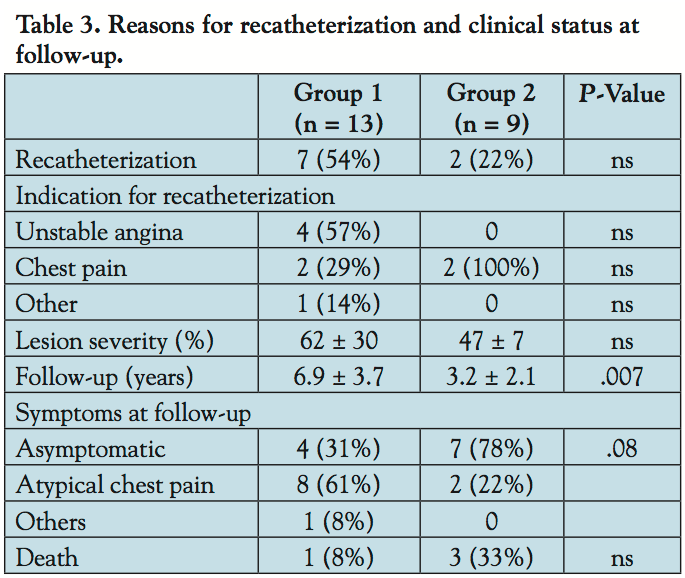 More patients were recatheterized during the follow-up period in group 1, mostly due to chest pain, although this did not reach statistical difference (Table 3). Interestingly, 3 of the patients who underwent repeat catheterization due to continuing chest pain, had a non-ischemic thallium stress test prior to the repeat catheterization. Of note, in the recatheterized patients in group 1, there was no disease progression. Of the 2 recatheterized patients in group 2, 1 had severe in-stent restenosis and this was successfully dilated with a drug-eluting stent.
More patients were recatheterized during the follow-up period in group 1, mostly due to chest pain, although this did not reach statistical difference (Table 3). Interestingly, 3 of the patients who underwent repeat catheterization due to continuing chest pain, had a non-ischemic thallium stress test prior to the repeat catheterization. Of note, in the recatheterized patients in group 1, there was no disease progression. Of the 2 recatheterized patients in group 2, 1 had severe in-stent restenosis and this was successfully dilated with a drug-eluting stent.
Updated clinical follow-up revealed that many of the patients in group 1 tended to have atypical chest pain, as opposed to patients in group 2, of whom most remained asymptomatic (P=.08). One patient in group 1 and 3 patients in group 2 died during the follow-up period (3 from non-cardiac causes and 1 of aortic stenosis leading to heart failure).
Discussion
Angioplasty to ostial lesions in branches of the main epicardial coronary arteries is a challenging procedure, due to the potential important complication of damaging the main vessel from which the branches arise.
Even in patients in whom the LAD has undergone angioplasty with resulting compromise of the ostium of a diagonal branch, there is debate regarding whether to treat the narrowed ostium. Ikeda et al2 recently described a benign course in such patients, who were left with a jailed diagonal origin following PCI to the LAD.
In the case of primary angioplasty to the ostium of a branch vessel with a reasonable diameter, however, the lesion should be dilated because of the clinical context of the patient.
Patients with ostial branch stenoses with severe anginal symptoms unresponsive to medical therapy constitute another group of patients in whom PCI should be performed despite the potential complications.
The only article in the literature addressing the dilemma of which approach to take in cases of ostial stenosis in diagonal branches, followed patients for only 1 year, and included patients with mild disease in other arteries.1
There are instances in which the angiographic severity of a stenotic lesion may be called in doubt, resulting in the use of other methods such as IVUS or FFR. In our study population, all the stenoses were angiographically clearly severe, so no use was made of these additional diagnostic techniques.
Our study is unique, as we included only patients with ostial stenoses of a diagonal branch, with otherwise entirely normal coronary arteries. In addition, we had a much longer period of follow-up compared to Brueck et al’s group of patients.1
We found that the arteries that were larger in diameter were more frequently dilated.
In contrast to Brueck’s findings,1 patients who underwent PCI in our group were more frequently asymptomatic following the procedure and underwent fewer repeat catheterizations. 54% of patients who were treated conservatively at initial catheterization underwent a repeat angiography during the period of follow-up. Surprisingly, the disease had not progressed in any patient and no patient needed an angioplasty to the lesion.
In all, 4 patients died during the follow-up period: 3 from non-cardiac causes and 1 of aortic stenosis leading to heart failure.
Study limitations. This is a retrospective, non-randomized, single-center study with a relatively small number of patients. The decision whether to adopt a conservative or invasive approach was taken by the operators at the time of the procedure and not according to any fixed departmental policy.
Conclusion
Although we have described a small group of stable patients with ostial diagonal stenoses, we recommend that a conservative medical approach is appropriate.
References
- Brueck M, Heidt M, Kramer W, Ludwig J. Comparison of interventional versus conservative treatment of isolated ostial lesions of coronary diagonal branch arteries. Am J Cardiol. 2004;93(9):1162-1164.
- Ikeda N, Yajima S, Asahara T, Sakai H. Intervention for jailed diagonal branch is not necessary while stenting the left anterior descending artery. J Intervent Cardiol. 2009;22(3):252-256.
_________________________________________________
From the Cardiology Department, Soroka Medical Center and Ben-Gurion University of the Negev, Beer-Sheva, Israel.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 21, 2011, provisional acceptance given November 22, 2011, final version accepted December 9, 2011.
Address for correspondence: Prof. Reuben Ilia, MD, Director, Cardiology Department, Soroka University Medical Center, POB 151, Beer-Sheva, Israel. Email: iliar@bgu.ac.il



