

Initial Human Experience with the XIENCE Side-Branch Access Device
Abstract: The everolimus-eluting XIENCE side-branch access (SBA) stent has been the focus of numerous recent publications. Most of the information available on this device comes from the preclinical studies performed in ovine models as well as perfused synthetic heart models. It has now become available in Europe as part of a limited test launch.
Delivered via a low-profile, dual-lumen, single-tip catheter, a single inflation device deploys the stent in the main branch and expands a portal opening into the ostium of the side branch to allow for scaffolding and entry into the side branch. This case report describes the first-in-man experience with this novel device.
J INVASIVE CARDIOL 2012;24(6):298-303
Key words: XIENCE side-branch access stent, XIENCE SBA
_________________________________________
The everolimus-eluting XIENCE side-branch access stent (XIENCE SBA; Abbott Vascular) has been the focus of numerous preclinical studies. Delivered via a low-profile, dual-lumen, single-tip catheter, a single inflation device deploys the stent in the main branch (MB) and expands a portal into the ostium of the side branch (SB).
The earliest studies were carried out in bench-top perfused synthetic heart models. The encouraging results in synthetic heart model studies prompted evaluation of the XIENCE SBA stent in large-animal, ovine, beating heart models. There have been several recent published reports summarizing these preclinical data. Using widely available workhorse stents as a comparison device, implantation of XIENCE SBA in experimental coronary vessels with complex, branching geometry has been associated with a relative reduction is contrast usage, shorter fluoroscopy times, and fewer episodes of guidewire entanglement, more commonly referred to as ‘wire-wrap.’1,2 Total procedure time with the XIENCE SBA stent was either comparable to or shorter than with the standard stent. Novel imaging modalities, such as high-intensity 2-dimensional Faxitron radiographic imaging, have shown that the XIENCE SBA favorably conforms to the vessel carina and provides adequate SB access in these experimental models.
Following recent CE marking, the XIENCE SBA is now available in selected European centers as part of a “first-in-man” experience. While this represents a limited device launch in Europe at selected centers, initial human experience includes the XIENCE SBA used in a number of different bifurcation treatment strategies; provisional SB stenting and upfront 2-stent techniques (for more complex parent and daughter vessel disease) are two of the more common clinical scenarios for which this device has been implanted. In addition, a number of operators have used this device simply as a means of “SB preservation” in Medina class 1,1,0 and 0,1,0 coronary anatomy. As such, this confers operator versatility, allowing for modification of the treatment algorithm as needed. The aim of this first-in-man limited European program is to build a database of practical, clinically meaningful device experience. In this article, we report the results of several recently completed cases in which the XIENCE SBA was used in a variety of anatomic subsets.
XIENCE SBA Stent
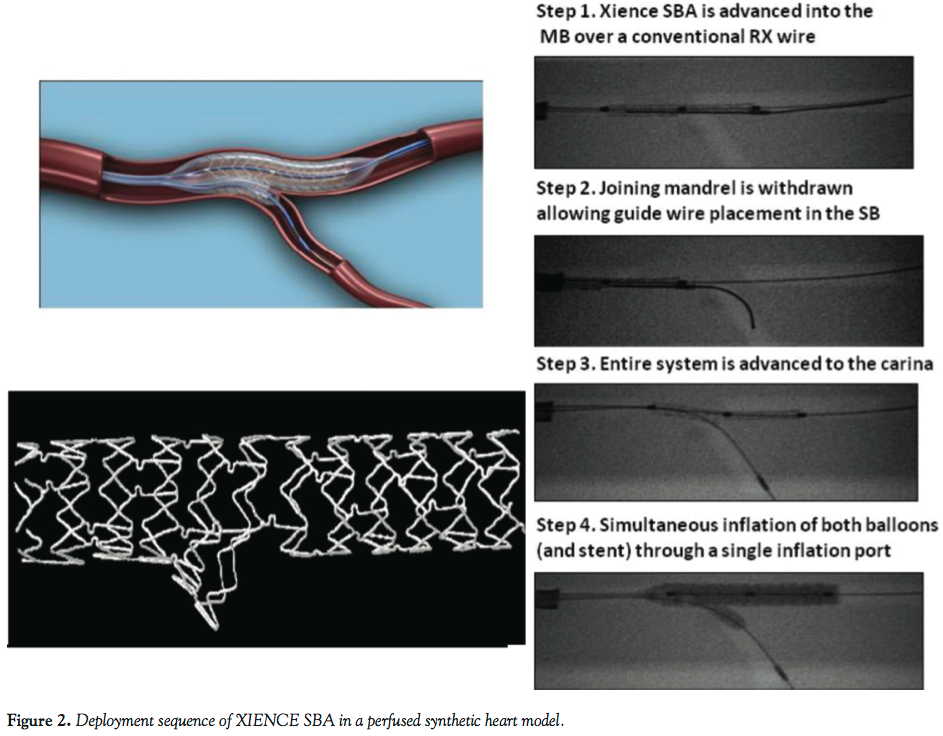
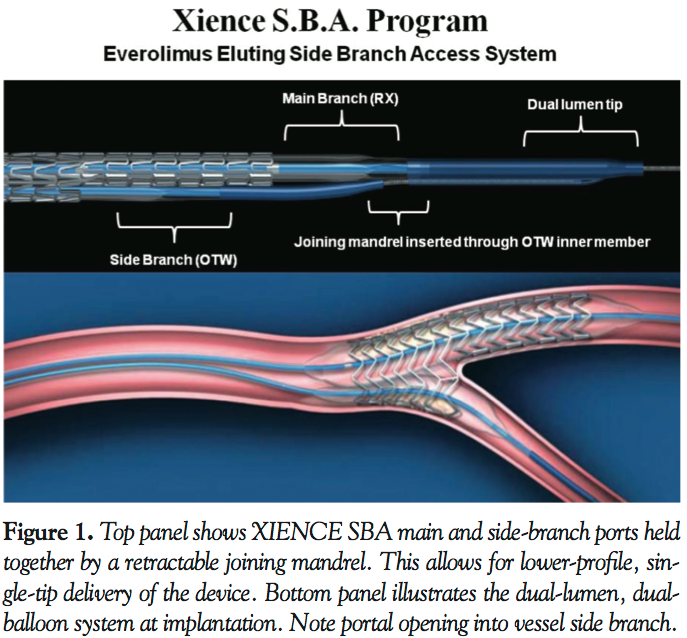 The XIENCE SBA stent is an everolimus-eluting stent that uses the drug, polymer, and scaffolding technology of the XIENCE V everolimus-eluting coronary stent system. The cobalt chromium stent is composed of 0.0034˝ struts and coated with a biocompatible fluoropolymer that releases everolimus at a controlled rate. The stent is delivered via a 7 Fr dual-lumen catheter containing an MB balloon attached to the rapid-exchange lumen and an SB balloon attached to the over-the-wire (OTW) lumen (Figure 1). The stent is crimped on both balloons to allow the SB balloon to exit through a portal opening located in the center of the stent. Proximal to the balloons, the two lumens converge into a single common inflation lumen that can be pressurized with a single inflation device. Of note, the catheter contains a unique joining mandrel that holds the MB and SB tips together to avoid guidewire entanglement before stent placement. The joining mandrel exits from the SB balloon tip and immediately enters a pocket alongside the extended MB balloon tip. This configuration effectively joins the two tips together, allowing easy single-tip delivery over only one wire (Figure 1). The device is engineered to self-rotate into proper alignment at the SB, thereby adding to its ease of use and predictability. The catheter is advanced to a point just proximal to the target bifurcation, and then the joining mandrel is unlocked (retracted) at the proximal adapter hub and withdrawn from the OTW lumen (Figure 2). A new wire is then introduced into the OTW lumen and placed into the SB. The system is then advanced into the bifurcation, and a single kissing-balloon inflation is used to deploy the MB stent and open a portal into the SB. This minimizes any plaque shifting from the MB or carina into the SB ostium, a common event during deployment of a conventional stent in the MB.3
The XIENCE SBA stent is an everolimus-eluting stent that uses the drug, polymer, and scaffolding technology of the XIENCE V everolimus-eluting coronary stent system. The cobalt chromium stent is composed of 0.0034˝ struts and coated with a biocompatible fluoropolymer that releases everolimus at a controlled rate. The stent is delivered via a 7 Fr dual-lumen catheter containing an MB balloon attached to the rapid-exchange lumen and an SB balloon attached to the over-the-wire (OTW) lumen (Figure 1). The stent is crimped on both balloons to allow the SB balloon to exit through a portal opening located in the center of the stent. Proximal to the balloons, the two lumens converge into a single common inflation lumen that can be pressurized with a single inflation device. Of note, the catheter contains a unique joining mandrel that holds the MB and SB tips together to avoid guidewire entanglement before stent placement. The joining mandrel exits from the SB balloon tip and immediately enters a pocket alongside the extended MB balloon tip. This configuration effectively joins the two tips together, allowing easy single-tip delivery over only one wire (Figure 1). The device is engineered to self-rotate into proper alignment at the SB, thereby adding to its ease of use and predictability. The catheter is advanced to a point just proximal to the target bifurcation, and then the joining mandrel is unlocked (retracted) at the proximal adapter hub and withdrawn from the OTW lumen (Figure 2). A new wire is then introduced into the OTW lumen and placed into the SB. The system is then advanced into the bifurcation, and a single kissing-balloon inflation is used to deploy the MB stent and open a portal into the SB. This minimizes any plaque shifting from the MB or carina into the SB ostium, a common event during deployment of a conventional stent in the MB.3
 For the purposes of the present European experience, all cases to date have utilized a XIENCE SBA system with a 3.0 mm everolimus-eluting stent identical in strut thickness, polymer, and drug-elution kinetics to the widely used Xience V everolimus-eluting coronary stent platform. In addition, all cases thus far have utilized the stent mounted on a 3.0 mm MB balloon and a 2.5 mm SB balloon for portal deployment into the SB ostium (Figure 1).
For the purposes of the present European experience, all cases to date have utilized a XIENCE SBA system with a 3.0 mm everolimus-eluting stent identical in strut thickness, polymer, and drug-elution kinetics to the widely used Xience V everolimus-eluting coronary stent platform. In addition, all cases thus far have utilized the stent mounted on a 3.0 mm MB balloon and a 2.5 mm SB balloon for portal deployment into the SB ostium (Figure 1).
 Using high-intensity 2-dimensional Faxitron imaging in perfused synthetic heart models, Figure 3 (left panel) demonstrates one of the commonly encountered shortcomings of bifurcation stenting: slotted-tube stents may be associated with a gap in stent coverage at the SB ostium. The panel to the right demonstrates one potential benefit of the XIENCE SBA configuration when encountering ostial SB disease. With the XIENCE SBA superimposed over the vessel carina (Figure 3, right panel), its SB portal opening can minimize this gap in stent coverage as has been demonstrated in previous published reports.4,5
Using high-intensity 2-dimensional Faxitron imaging in perfused synthetic heart models, Figure 3 (left panel) demonstrates one of the commonly encountered shortcomings of bifurcation stenting: slotted-tube stents may be associated with a gap in stent coverage at the SB ostium. The panel to the right demonstrates one potential benefit of the XIENCE SBA configuration when encountering ostial SB disease. With the XIENCE SBA superimposed over the vessel carina (Figure 3, right panel), its SB portal opening can minimize this gap in stent coverage as has been demonstrated in previous published reports.4,5
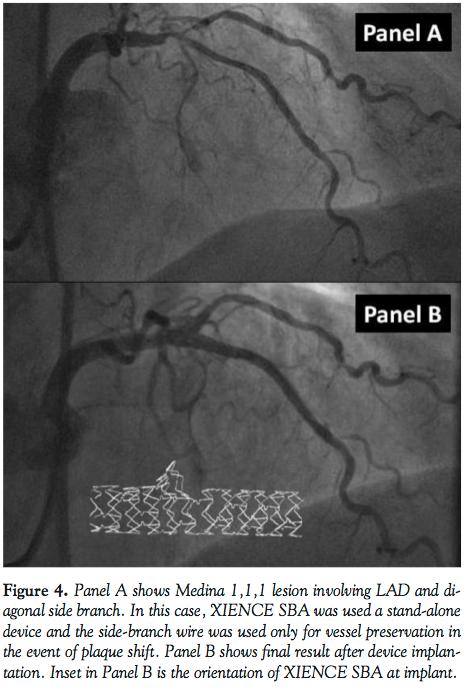 Figures 4 and 5 represent a case in which XIENCE SBA was used as part of a treatment strategy in which only the main branch left anterior descending (LAD) coronary artery was stented and the SB wire was used solely as a means of preserving the daughter vessel in the event of plaque shift or of a suboptimal angiographic outcome. Superimposed into Figure 4 (Panel B) is an image of XIENCE SBA and the orientation of its portal opening at the level of the vessel carina. The recommended deployment sequence for XIENCE SBA used in this
Figures 4 and 5 represent a case in which XIENCE SBA was used as part of a treatment strategy in which only the main branch left anterior descending (LAD) coronary artery was stented and the SB wire was used solely as a means of preserving the daughter vessel in the event of plaque shift or of a suboptimal angiographic outcome. Superimposed into Figure 4 (Panel B) is an image of XIENCE SBA and the orientation of its portal opening at the level of the vessel carina. The recommended deployment sequence for XIENCE SBA used in this 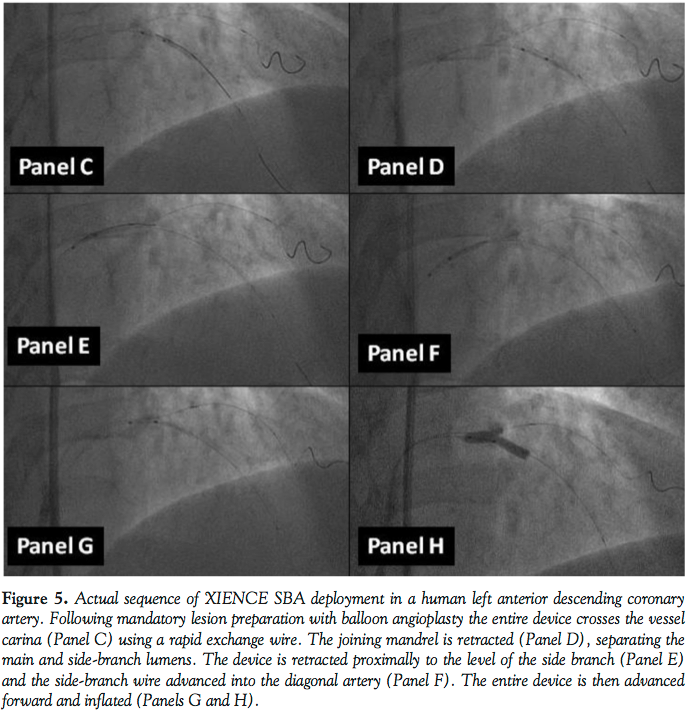 case is shown in Figure 5. After adequate vessel preparation with standard balloon angioplasty, the entire device is advanced beyond the vessel carina (Panel C). The joining mandrel is then retracted, thus separating the MB and SB ports (Panel D). The entire device is then retracted proximal to the carina, exposing the XIENCE SBA SB portal opening to the SB ostium (Panel E). Next, the SB wire is advanced into the daughter vessel (Panel F) and, following deployment of the SB wire, the entire device is advanced forward to envelop the carina (Panel G). It merits discussion that once the MB and SB wires have been advanced into their respective positions, they may be used to rotate the device into proper orientation. Finally, the MB and SB balloons onto which the stent is mounted can be inflated through a single inflation port. Figure 5 (Panel H) demonstrates both MB balloon inflation and expansion of the SB portal.
case is shown in Figure 5. After adequate vessel preparation with standard balloon angioplasty, the entire device is advanced beyond the vessel carina (Panel C). The joining mandrel is then retracted, thus separating the MB and SB ports (Panel D). The entire device is then retracted proximal to the carina, exposing the XIENCE SBA SB portal opening to the SB ostium (Panel E). Next, the SB wire is advanced into the daughter vessel (Panel F) and, following deployment of the SB wire, the entire device is advanced forward to envelop the carina (Panel G). It merits discussion that once the MB and SB wires have been advanced into their respective positions, they may be used to rotate the device into proper orientation. Finally, the MB and SB balloons onto which the stent is mounted can be inflated through a single inflation port. Figure 5 (Panel H) demonstrates both MB balloon inflation and expansion of the SB portal.
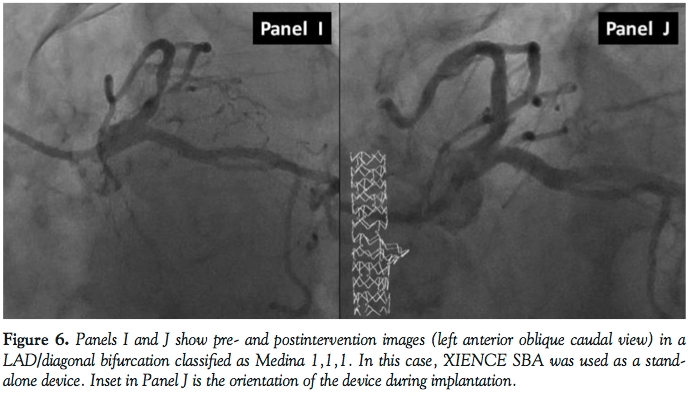 Figure 6 (Panels I and J) demonstrates XIENCE SBA used as a stand-alone device in a LAD lesion with wire preservation of the diagonal artery. In this case, the operator chose to use final alternating balloon inflations in the MB (3.0 NC balloon) and SB (2.5 NC balloon). The final angiographic result as well as the orientation of the device during deployment are shown in Panel J.
Figure 6 (Panels I and J) demonstrates XIENCE SBA used as a stand-alone device in a LAD lesion with wire preservation of the diagonal artery. In this case, the operator chose to use final alternating balloon inflations in the MB (3.0 NC balloon) and SB (2.5 NC balloon). The final angiographic result as well as the orientation of the device during deployment are shown in Panel J.
Figure 7 demonstrates the potential of this device to be utilized as part of a  provisional SB approach in the event of a suboptimal result. Panel K demonstrates the lesion prior to balloon predilation. Following mandatory balloon angioplasty of MB and SB in this case, a dissection is noted in the SB vessel (Panel L). After XIENCE SBA is implanted, an additional stent (2.5 mm XIENCE V everolimus-eluting stent) is advanced through the expanded SB portal opening (OTW) to cover the SB dissection. It can be aligned with the SB portal so as to adequately cover the vessel ostium in order to ameliorate the potential for gaps in ostial SB coverage. Additional stents may be placed in the MB and/or SB while maintaining wire position in both branches. The far right image (Panel M) shows the final result following deployment of XIENCE SBA, the additional 2.5 mm XIENCE stent in the SB and final kissing-balloon angioplasty with a 2.5 mm non-compliant SB balloon and a 3.0 non-compliant MB balloon.
provisional SB approach in the event of a suboptimal result. Panel K demonstrates the lesion prior to balloon predilation. Following mandatory balloon angioplasty of MB and SB in this case, a dissection is noted in the SB vessel (Panel L). After XIENCE SBA is implanted, an additional stent (2.5 mm XIENCE V everolimus-eluting stent) is advanced through the expanded SB portal opening (OTW) to cover the SB dissection. It can be aligned with the SB portal so as to adequately cover the vessel ostium in order to ameliorate the potential for gaps in ostial SB coverage. Additional stents may be placed in the MB and/or SB while maintaining wire position in both branches. The far right image (Panel M) shows the final result following deployment of XIENCE SBA, the additional 2.5 mm XIENCE stent in the SB and final kissing-balloon angioplasty with a 2.5 mm non-compliant SB balloon and a 3.0 non-compliant MB balloon.
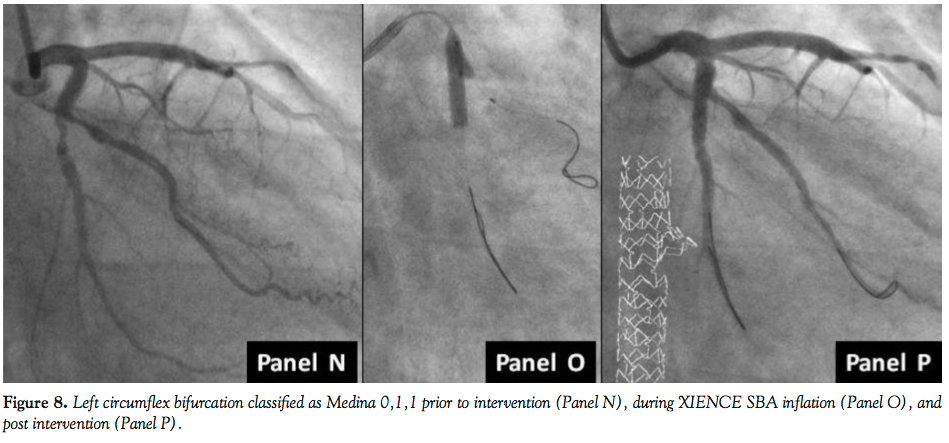 Figure 8 shows XIENCE SBA deployment as part of treating a Medina 0,1,1 lesion. Panel N represents the lesion prior to vessel balloon pretreatment. Following balloon angioplasty of the main branch, the device was inflated at pressures of 14 atm (Panel O) and the final result (Panel P) was achieved with no further postdeployment inflations.
Figure 8 shows XIENCE SBA deployment as part of treating a Medina 0,1,1 lesion. Panel N represents the lesion prior to vessel balloon pretreatment. Following balloon angioplasty of the main branch, the device was inflated at pressures of 14 atm (Panel O) and the final result (Panel P) was achieved with no further postdeployment inflations.
Figure 9 is the first XIENCE SBA implantation to be performed as part of a live 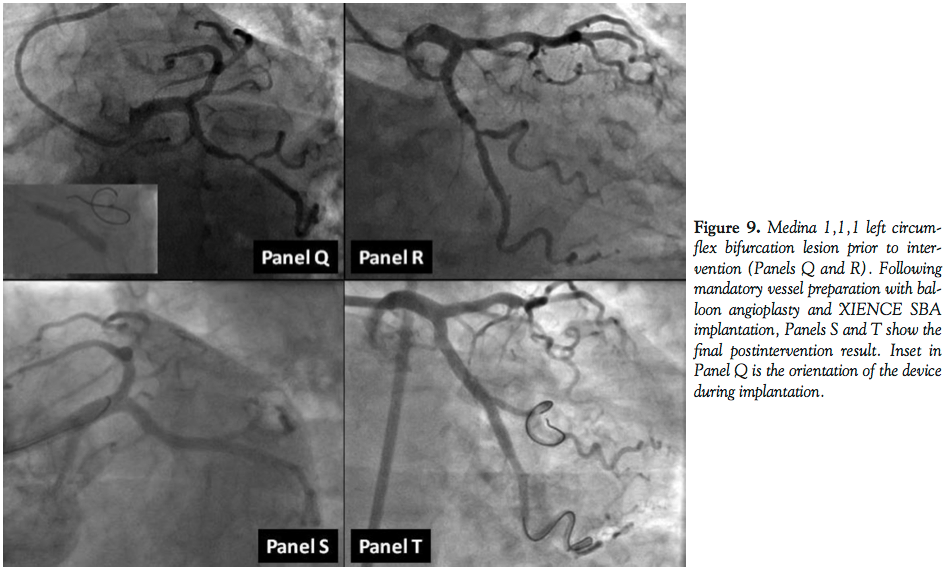 case demonstration course (The 16th Annual Warsaw Course on Cardiovascular Interventions). Panels Q and R illustrate not only the lesion severity at the level of the bifurcation in this right-angle takeoff left circumflex coronary artery, but also demonstrate the ability to negotiate the device around angulated vessel geometry, after thorough vessel preparation with balloon therapy has been performed. The left circumflex was designated as the MB for the purposes of this implant and the
case demonstration course (The 16th Annual Warsaw Course on Cardiovascular Interventions). Panels Q and R illustrate not only the lesion severity at the level of the bifurcation in this right-angle takeoff left circumflex coronary artery, but also demonstrate the ability to negotiate the device around angulated vessel geometry, after thorough vessel preparation with balloon therapy has been performed. The left circumflex was designated as the MB for the purposes of this implant and the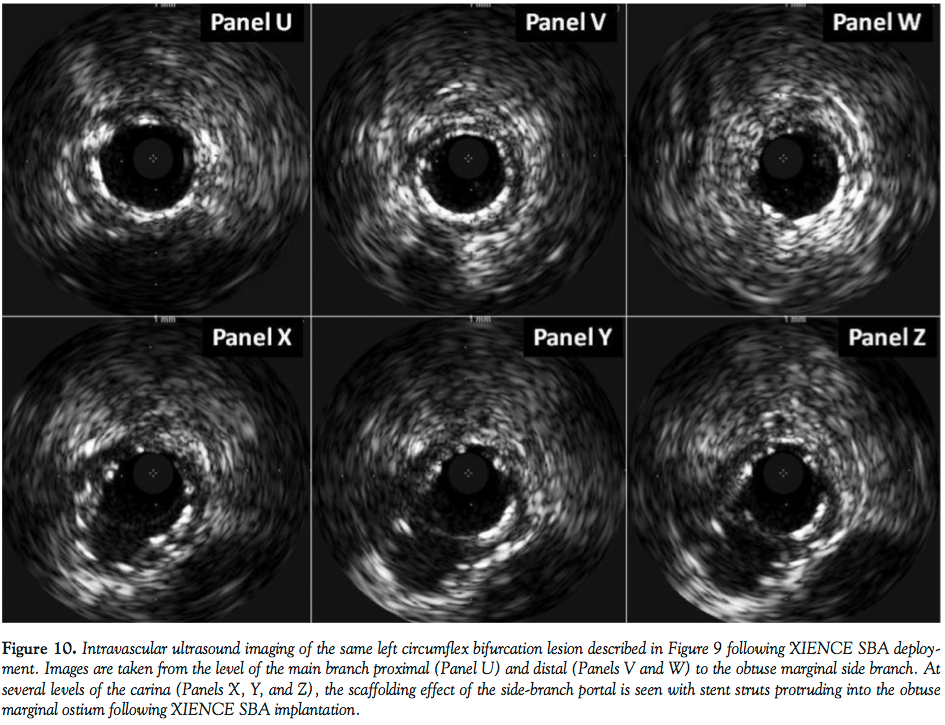 obtuse marginal considered the SB into which the portal opening was deployed. The orientation of XIENCE SBA during inflation is inset into Panel Q. Following high-pressure dilation, the final result is noted in both left anterior oblique caudal and anteroposterior caudal views (Panels S and T). Intravascular ultrasound (IVUS) assessment following final XIENCE SBA inflation is demonstrated in Figure 10, showing the MB proximal (Panel U) and distal (Panels V and W) to the obtuse marginal SB. The sonographic appearance of the portal opening into the SB is appreciated at various levels of the carina (Panels X, Y, and Z) demonstrating ostial SB coverage provided by this 1-2 mm aperture.
obtuse marginal considered the SB into which the portal opening was deployed. The orientation of XIENCE SBA during inflation is inset into Panel Q. Following high-pressure dilation, the final result is noted in both left anterior oblique caudal and anteroposterior caudal views (Panels S and T). Intravascular ultrasound (IVUS) assessment following final XIENCE SBA inflation is demonstrated in Figure 10, showing the MB proximal (Panel U) and distal (Panels V and W) to the obtuse marginal SB. The sonographic appearance of the portal opening into the SB is appreciated at various levels of the carina (Panels X, Y, and Z) demonstrating ostial SB coverage provided by this 1-2 mm aperture.
Conclusion
Initial human experience with XIENCE SBA continues in Europe as part of a limited operator program at prespecified centers. The results of these initial human implants in terms of device and procedural success will be the focus of future planned publications. Initial physician feedback is currently being assessed and operator observations appear promising thus far.
Given the heterogeneity of bifurcation coronary lesions, the XIENCE SBA may offer versatility in the treatment of anatomic variations of disease. The images above demonstrate use of the XIENCE SBA as part of complex 1- and 2-stent strategies. Device deployment as part of a provisional methodology or even as a simple SB preservation technique, while maintaining MB and SB wire position, may underscore the versatility of this novel device. While images shown here give cause for optimism, further studies to define the role of the XIENCE SBA in the treatment of bifurcation coronary disease and to validate device safety and efficacy are warranted.
References
- Rizik DG, Klag JM, Tenaglia A, et al. Evaluation of a bifurcation drug-eluting stent system versus provisional T-stenting in a perfused synthetic coronary artery model. J Interv Cardiol. 2009;22(6):537-546.
- Hermiller JB. Contemporary bifurcation treatment strategies: the role of currently available slotted tube stents. Rev Cardiovasc Med. 2010;11(Suppl 1):S17-S26.
- Koo BK, Waseda K, Kang HJ, et al. Anatomic and functional evaluation of bifurcation lesions undergoing percutaneous coronary intervention. Circ Cardiovasc Interv. 2010;3(2):113-119.
- Rizik DG, Klassen KJ. Dedicated bifurcation devices. Rev Cardiovasc Med. 2010;11(Suppl 1):S27-S37.
- Costa RA, Mintz GS, Carlier SG, et al. Bifurcation coronary lesions treated with the “crush” technique. An intravascular ultrasound analysis. J Am Coll Cardiol. 2005;46(4):599-605.
_________________________________________
From the 1Department of Heart & Vascular Medicine, Scottsdale Healthcare Hospitals, Scottsdale, Arizona, 2the David Geffen UCLA School of Medicine, Los Angeles, California, 3the Department of Clinical Engineering, Abbott Vascular, Santa Clara, California, and 4the Invasive Cardiology Department, Central Hospital of Internal Affairs and Administration Ministry, Institute of Experimental and Clinical Medicine, Polish Academy of Science, Warsaw, Poland.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 23, 2012 and accepted April 25, 2012.
Address for correspondence: David G. Rizik, MD, Scottsdale Heart Group, Scottsdale Healthcare Hospital, 10101 North 92th Street, Suite 101, Scottsdale, AZ 85258. Email: davidrizik@aol.com

