

A High Dose of Adenosine to Induce Transient Asystole for Valvuloplasty in Patients Undergoing Transcatheter Aortic Valve Implantation (TAVI): Is it a Valid Alternative to Rapid Pacing? A Prospective Pilot Study
Abstract: Background. Rapid right ventricular pacing (RRVP) at rates above 200 beats/minute is used to suppress cardiac output during balloon aortic valvuloplasty (BAV) in transcatheter aortic valve replacement (TAVI) patients. A risk of inducing myocardial ischemia with RRVP remains, especially in patients with left ventricular dysfunction. Alternatively, a transient cardiac arrest can be achieved with administration of adenosine. Methods. The primary endpoint was successful valvuloplasty defined by complete balloon inflation and deflation across aortic valve during the transient asystole induced by adenosine. Secondary endpoints were defined as the failure of adenosine to induce asystole, the incidence of ventricular ectopic beats (VEB) during balloon inflation or deflation, and balloon displacement. Results. From November 2010 to January 2011, twenty consecutive patients who underwent TAVI were included. A balloon for valvuloplasty was positioned across the aortic valve. A low-dose (24 mg, n = 10) or high-dose (36 mg, n = 10) bolus of adenosine was administrated. A single bolus of adenosine-induced atrioventricular (AV) block (mean duration, 18.6 ± 6.6 seconds) followed by cardiac asystole in 16 patients (80%) (low-dose, n = 9). A successful BAV was achieved in 12 patients (60%) (low-dose, n = 8). Adenosine induced only bradycardia in 4 patients (20%) (low-dose, n = 1). A burst of VEB during BAV occurred in all patients. Balloon displacement occurred in 6 patients (37.5%). Conclusion. BAV after administration of adenosine is feasible, safe, and may represent an option for high-risk TAVI patients in whom RRVP might not be well tolerated. The occurrence of ventricular ectopic contractions triggered by balloon inflation and deflations accounts for balloon displacement and crossover to RRVP.
J INVASIVE CARDIOL 2011;23(11):467-471
Key words: adenosine, valvuloplasty, TAVI
___________________________________
Recently, balloon aortic valvuloplasty (BAV) has regained interest as an integral part of transcatheter aortic valve implantation (TAVI) playing a major role in preparing the aortic valve (AoV) for the implantation in selected patients with calcific stenosis. Since its introduction in 1986,1 the technical aspect of BAV has been modified. For example, rapid right ventricular pacing (RRVP) is commonly used to ensure balloon stability during inflation. By reducing cardiac filling, ejection time, and therefore cardiac output, it effectively eliminates the transaortic gradient and induces a transient state of hypotension. Transient sufficiently long cardiac activity suppression is needed to allow balloon inflation across stenotic AoV followed by quick recovery to normal electrical cardiac cycle activity and systemic blood pressure. Nevertheless, myocardial ischemia and/or ventricular arrhythmias following RRVP have been reported, especially in patients with LV dysfunction and coronary artery disease.
Alternatively, a transient cardiac arrest can also be achieved with the administration of adenosine. It is unclear which dosage of adenosine can trigger an asystolic period of sufficient length to accomplish valvuloplasty, and if adenosine can be safely used instead of RRVP during BAV.
Therefore, the aim of our study was to assess safety and feasibility of high-dose (36 mg) versus low-dose (24 mg) adenosine administration during BAV as an alternative to RRVP during TAVI.
Methods
The primary endpoint was successful valvuloplasty, defined as complete balloon inflation and deflation across the AoV during the transient asystole induced by a single bolus of adenosine. Secondary endpoints were defined as the failure of adenosine to induce asystole, the incidence of ventricular ectopic beats during balloon inflation or deflation, and balloon displacement requiring repositioning.
To evaluate a dose effect on the duration of atrioventricular block followed by cardiac asystole, patients were randomized in a 1:1 ratio into two groups according to the bolus dose of adenosine: low-dose (24 mg) versus high-dose (36 mg).
Inclusion criteria. Consecutive patients undergoing TAVI procedure due to calcific AoV stenosis.
Exclusion criteria. Contraindications to adenosine; existing permanent pacemaker; all patients signed an informed consent.
Procedure. TAVI was performed according to our current practice.2 A pigtail catheter was positioned in the ascending aorta just above the leaflets of the valve. After crossing the AoV with an extra stiff guidewire, a balloon catheter was advanced across the AoV.
An adenosine bolus was injected through a pigtail catheter to induce asystole; the tubular balloon was then inflated and deflated. In the event of balloon displacement, repositioning was attempted if adenosine-induced asystole was still present. RRVP was applied only when an additional balloon inflation was needed to optimize the valvuloplasty result, but adenosine-induced asystole was over.
BAV was defined as successful if it was accomplished after a single bolus of adenosine without RRVP. The aortic prosthesis was then implanted according to our current practice.2
Statistical analysis. The results are reported as mean ± standard deviation where appropriate. Categorical data are presented as counts and percentages. Clinical characteristics were compared between patients according to the adenosine bolus dose of 24 or 36 mg using the univariate t-test and chi-squared test. Significance was identified at P<.05 (two-sided). Systolic pressure prior to valvuloplasty and during ventricular ectopic beats was compared using the paired sample t-test.
Results
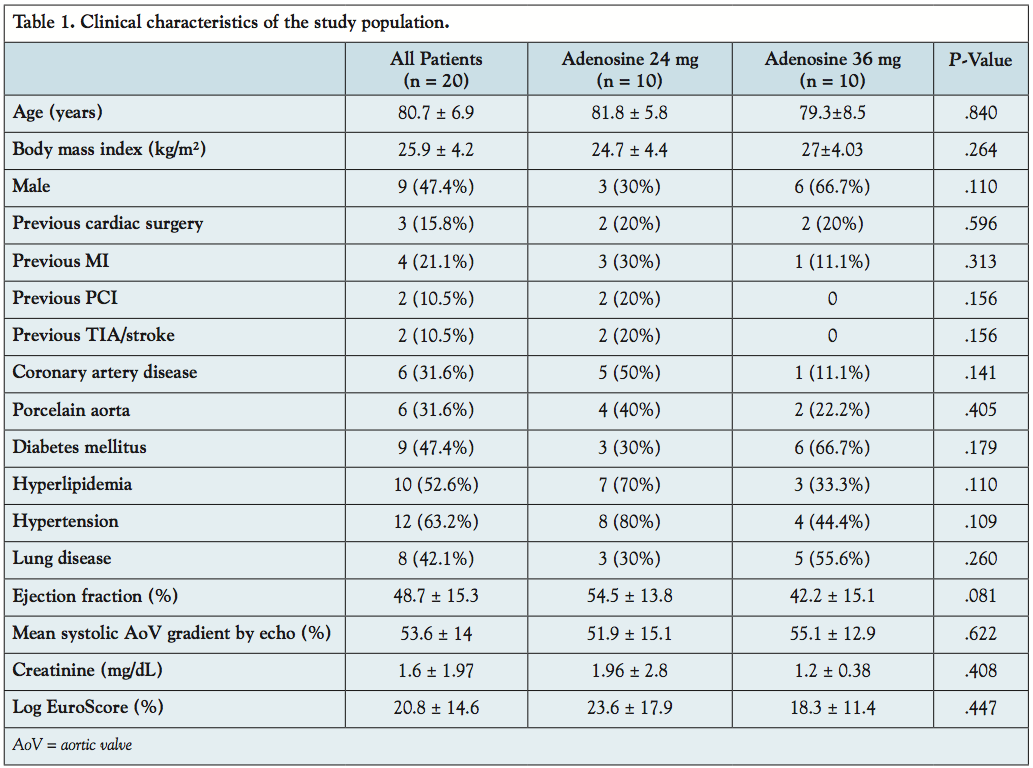 From November 2010 to January 2011, a total of 20 consecutive patients (45% men; mean age, 80.7 ± 6.9 years; mean systolic AoV gradient, 53.6 ± 14 mmHg; logistic EuroSCORE, 20.8 ± 14.6%) who underwent TAVI at our center were included. Patient’s clinical characteristics are illustrated in Table 1.
From November 2010 to January 2011, a total of 20 consecutive patients (45% men; mean age, 80.7 ± 6.9 years; mean systolic AoV gradient, 53.6 ± 14 mmHg; logistic EuroSCORE, 20.8 ± 14.6%) who underwent TAVI at our center were included. Patient’s clinical characteristics are illustrated in Table 1.
A balloon for valvuloplasty (median diameter, 23 mm [IQR, 20-23; min-max, 20-23], median length, 30 mm [IQR, 30-37.5; min-max, 20-60]) was positioned across the aortic valve. A low-dose (24 mg, n = 10) or high-dose (36 mg, n = 10) bolus of adenosine was administrated according to randomization.
A single bolus of adenosine-induced atrioventricular block (mean duration, 18.6 ± 6.6 seconds) followed by cardiac asystole in 16 patients (80%), 9 low-dose patients versus 7 high-dose patients.
The mean duration of AV block was significantly longer after high-dose bolus as compared to low-dose bolus (22.5 ± 7.5 seconds vs 15.6 ± 4.1 seconds, P=.034). Transient pacing was required because of prolonged AV block in 8 patients (40%; 5 high-dose group, P=NS). Conversely, no patient required inotropic support for hemodynamic instability.
A successful BAV (primary study endpoint) was achieved in 12 patients (60%). No difference was observed between high- versus low-dose groups (4 versus 8 patients, respectively).
Adenosine induced only bradycardia, but not asystole, in 4 patients (20%), only 1 in the low-dose group. In 2 out of 4 patients, AV block was replaced by idioventricular rhythm interrupting cardiac standstill. RRVP for BAV was used in all 4 patients.
A burst of VEB associated with balloon inflation and deflation occurred in all 16 patients (mean duration, 7.1 ± 4.1 seconds; min-max, 3-19 seconds).
Balloon displacement requiring repositioning occurred in 6 of the 16 patients (37.5%). The balloon was successfully repositioned and valvuloplasty accomplished without an additional dose of adenosine or RRVP in 2 patients (24 mg, n = 1). RRVP was necessary to accomplish valvuloplasty in the remaining 4 patients (36 mg, n = 3).
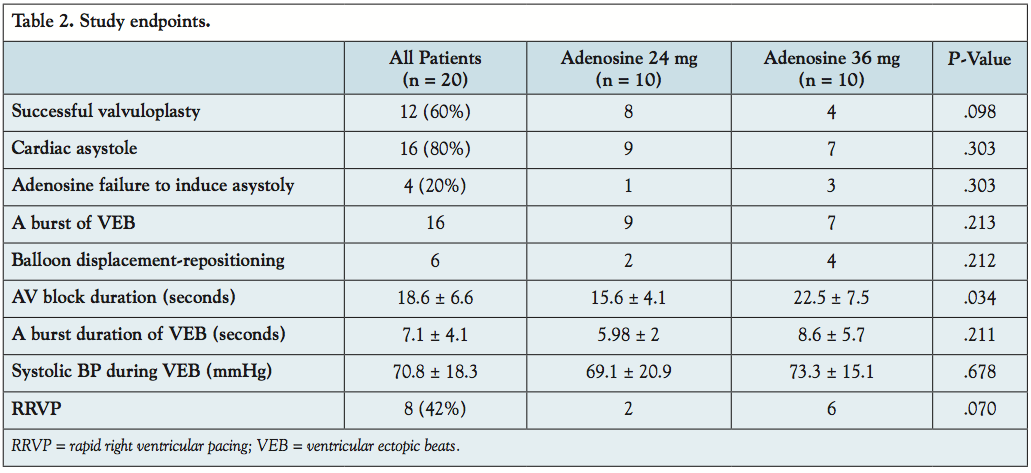 Study endpoints are reported in Table 2. Seventeen patients (85%) had an uneventful hospital outcome. No patients died or had a myocardial infarction during hospital stay. Two patients had cardiac tamponade related to TAVI procedure, which required urgent pericardiocentesis. In 1 case, pericardiocentesis was related to positioning of the pacing wire and in another to positioning a stiff guidewire into the cavity of the left ventricle. The last case required cardiac surgery management for bleeding control. Ischemic stroke was diagnosed in 1 patient after AoV implantation 12 hours later.
Study endpoints are reported in Table 2. Seventeen patients (85%) had an uneventful hospital outcome. No patients died or had a myocardial infarction during hospital stay. Two patients had cardiac tamponade related to TAVI procedure, which required urgent pericardiocentesis. In 1 case, pericardiocentesis was related to positioning of the pacing wire and in another to positioning a stiff guidewire into the cavity of the left ventricle. The last case required cardiac surgery management for bleeding control. Ischemic stroke was diagnosed in 1 patient after AoV implantation 12 hours later.
Discussion
The main findings of this pilot study are: 1) adenosine bolus administration was associated to a successful BAV in 60% of the patients (primary study endpoint) and could therefore represent a possible alternative during TAVI to RRVP in selected patients; 2) no further advantage was reported with higher adenosine dosages (36 versus 24 mg); 3) adenosine bolus during BAV is safe and not associated with harmful complications; and 4) the frequent occurrence of ventricular ectopic beats during transient asystole makes this approach unsuitable for valve positioning.
It has already been reported that in order to induce cardiac asystole lasting 8-10 seconds, the adenosine dose should be within the range of 6-90 mg.3-5 Kahn et al reported that adenosine doses ranged from 24-90 mg to induce at least 10 seconds of asystole.3 The authors studied 98 patients in whom balloon-deployed stent-graft was used for endovascular abdominal aortic aneurysm repair. It was not reported how many patients needed an increased dose of adenosine over 24 mg. Other authors showed that sustained ventricular asystole of 11-23 seconds duration was achieved with 60 mg of adenosine-triphosphate (ATP) in 71% of patients, and in 92% receiving 100 mg of ATP.6
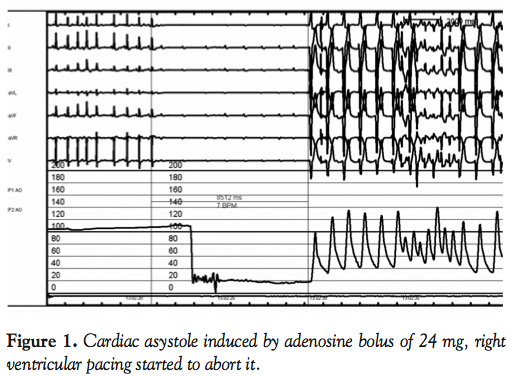 In our study, a dose of 24 mg was sufficient in 90% of the cases to induce transient AV block lasting around 15 seconds. A typical example of the action of adenosine is presented in Figure 1. Therefore, an additional clinical benefit from a higher dose of adenosine is unlikely, and simply prolongs the duration of the transient AV block without improving the overall success of valvuloplasty.
In our study, a dose of 24 mg was sufficient in 90% of the cases to induce transient AV block lasting around 15 seconds. A typical example of the action of adenosine is presented in Figure 1. Therefore, an additional clinical benefit from a higher dose of adenosine is unlikely, and simply prolongs the duration of the transient AV block without improving the overall success of valvuloplasty.
Although adenosine induced atrioventricular block followed by asystole in 16 cases (80%), in the remaining 4 patients RRVP was used to accomplish valvuloplasty.
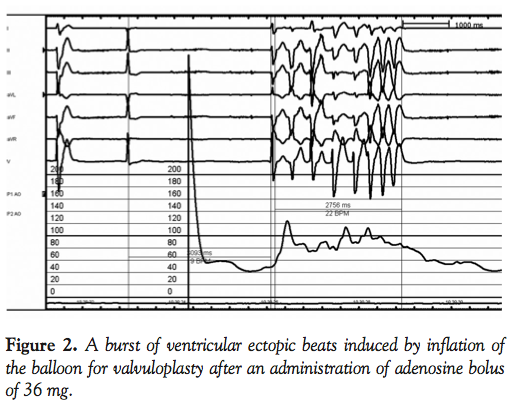 It is interesting to note that in all cases of valvuloplasty, adenosine cardiac standstill was interrupted by VEB during balloon inflation and deflation (Figures 2 and 3). This phenomenon may be related to mechanical irritation of the left ventricular outflow tract endocardium by the surface of the expanding balloon, or the movement of the stiff guidewire during inflation and deflation. The systolic pressure generated by ectopic cardiac contractions was significantly lower in comparison to baseline prior to valvuloplasty (72.6 ± 18.8 mmHg versus 140.5 ± 34.1 mmHg, P<.05) but was sufficient to push the inflated balloon back into the aorta.
It is interesting to note that in all cases of valvuloplasty, adenosine cardiac standstill was interrupted by VEB during balloon inflation and deflation (Figures 2 and 3). This phenomenon may be related to mechanical irritation of the left ventricular outflow tract endocardium by the surface of the expanding balloon, or the movement of the stiff guidewire during inflation and deflation. The systolic pressure generated by ectopic cardiac contractions was significantly lower in comparison to baseline prior to valvuloplasty (72.6 ± 18.8 mmHg versus 140.5 ± 34.1 mmHg, P<.05) but was sufficient to push the inflated balloon back into the aorta.
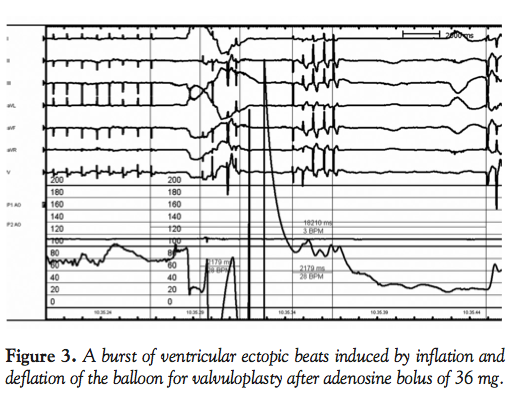 It has already been reported by McKay et al that premature ventricular contractions occur during the period of balloon inflation in all patients who underwent balloon valvuloplasty for treatment of aortic stenosis.7 While the administration of adenosine is effective in creating a sufficiently long period of AV block followed by cardiac asystole, it does not prevent the occurrence of ventricular ectopic beats induced by a mechanical trigger.
It has already been reported by McKay et al that premature ventricular contractions occur during the period of balloon inflation in all patients who underwent balloon valvuloplasty for treatment of aortic stenosis.7 While the administration of adenosine is effective in creating a sufficiently long period of AV block followed by cardiac asystole, it does not prevent the occurrence of ventricular ectopic beats induced by a mechanical trigger.
We have attempted to overcome this problem of balloon displacement by ventricular ectopic beats utilizing longer balloons. Therefore, in 2 cases we selected a balloon length of 60 mm. However, in both cases displacement of the balloon occurred and RRVP was performed.
Adenosine-induced cardiac standstill might be a valid technique for extra cardiac applications, such as facilitating the precise deployment of stent endografts in the thoracic or abdominal aorta,3,8 enhancing three-dimensional rotational imaging during cardiac ablation procedures9 or facilitating treatment of cerebral arteriovenous malformations.10 De Giovanni et al have suggested applying the technique to patients with congenital heart disease to maintain balloon stability during valvuloplasty.11
Adenosine has been reported to play a role during percutaneous mitral valve clip positioning.12
In our study, a successful BAV was achieved following adenosine administration in 60% of the patients. In the patients where BAV was unsuccessful, RRVP was then immediately successfully applied. No harmful complication was reported following adenosine administration. There were no in-hospital deaths or myocardial infarctions after the TAVI procedure. A patient who had a stroke after TAVI implantation had a full recovery, with no residual functional deficit. An urgent pericardiocentesis was performed in 2 patients due to cardiac tamponade related to the positioning of the pacing wire and stiff guidewire. In both cases, complication occurred prior to valvuloplasty; therefore, it is not related to adenosine administration.
Therefore, adenosine could represent an acceptable alternative to RRVP in selected patients, such as low left ventricular ejection fraction and severe coronary artery disease who may not tolerate the pacing maneuver. The incidence of associated coronary artery disease was about 45% in patients with aortic stenosis who were aged ≥60 years.13 In these patients, RRVP might be not well-tolerated, as it aggravates myocardial ischemia or causes life-threatening arrhythmias requiring direct current cardioversion complicating and delaying aortic valve implantation. The threshold for inducible myocardial ischemia is very low in patients with AoV stenosis because of severe left ventricular hypertrophy and an existing missmatch between the density of coronary microcirculation and supplied myocytes. Therefore, a risk of inducing myocardial ischemia and ventricular arrhythmias with RRVP remains, especially in patients with severe left ventricular dysfunction and coronary artery disease.
In summary, adenosine-induced cardiac standstill could represent a viable alternative in patients undergoing balloon valvuloplasty who may not tolerate RRVP. Given the frequency of VEB during balloon inflation and deflation, adenosine cannot be recommended as a safe and effective means of stabilization during balloon expandable aortic valve implantation. It might be argued that adenosine should be reserved for the small niche of patients undergoing valvuloplasty alone. A bolus of 24 mg of adenosine is effective in inducing sufficiently long cardiac asystole and could be used to facilitate selected catheterization procedures.
Limitations. This is a pilot study and the limited number of patients is therefore too small to be powered to demonstrate any significant difference between the two adenosine dosages (high vs. low). The limited number of patients can also have played a role in the assessment of adenosine feasibility. It is difficult to calculate the real duration of asystole as it was interrupted by ventricular ectopic beats.
Conclusions
BAV after administration of adenosine is feasible and may represent an option for high-risk TAVI patients in whom RRVP might not be well tolerated. The occurrence of ventricular ectopic contractions triggered by balloon inflation and deflations, regardless of adenosine dose, accounts for balloon displacement and crossover to RRVP. A significantly longer period of asystole can be induced with an adenosine bolus of 36 mg, but without an increase in success of valvuloplasty.
Listen to a podcast based upon this research with Dr. Colombo at https://invasivecardiology.com/content/high-dose-adenosine.
References
- Cribier A, Savin T, Saoudi N, et al. Percutaneous transluminal aortic valvuloplasty using a balloon catheter. A new therapeutic option in aortic stenosis in the elderly. Arch Mal Coeur Vaiss. 1986;79(12):1678-1686.
- Godino C, Maisano F, Montorfano M, et al. Outcomes after transcatheter aortic valve implantation with both Edwards-SAPIEN and CoreValve devices in a single center: the Milan experience. JACC Cardiovasc Interv. 2010;3(11):1110-1121.
- Kahn RA, Moskowitz DM, Marin ML, et al. Safety and efficacy of high-dose adenosine-induced asystole during endovascular AAA repair. J Endovasc Ther. 2000;7(4):292-296.
- Hashimoto T, Young WL, Aagaard BD, Joshi S, Ostapkovich ND, Pile-Spellman J. Adenosine-induced ventricular asystole to induce transient profound systemic hypotension in patients undergoing endovascular therapy. Dose-response characteristics. Anesthesiology. 2000;93(4):998-1001.
- Qu L, Raithel D. Techniques for precise thoracic endograft placement. J Vasc Surg. 2009;49(4):1069-1072; discussion 72.
- Rankin AC, Oldroyd KG, Chong E, Dow JW, Rae AP, Cobbe SM. Adenosine or adenosine triphosphate for supraventricular tachycardias? Comparative double-blind randomized study in patients with spontaneous or inducible arrhythmias. Am Heart J. 1990;119(2 Pt 1):316-323.
- McKay RG, Safian RD, Lock JE, et al. Assessment of left ventricular and aortic valve function after aortic balloon valvuloplasty in adult patients with critical aortic stenosis. Circulation. 1987;75(1):192-203.
- Dorros G, Cohn JM. Adenosine-induced transient cardiac asystole enhances precise deployment of stent-grafts in the thoracic or abdominal aorta. J Endovasc Surg. 1996;3(3):270-272.
- Ector J, De Buck S, Nuyens D, et al. Adenosine-induced ventricular asystole or rapid ventricular pacing to enhance three-dimensional rotational imaging during cardiac ablation procedures. Europace. 2009;11(6):751-762.
- Hashimoto H, lida J, Hironaka Y, Sakaki T. Surgical management of cerebral arteriovenous malformations with intraoperative digital subtraction angiography. J Clin Neurosci. 2000;7(Suppl 1):33-35.
- De Giovanni JV, Edgar RA, Cranston A. Adenosine induced transient cardiac standstill in catheter interventional procedures for congenital heart disease. Heart. 1998;80(4):330-333.
- Borgia F, Di Mario C, Franzen O. Adenosine-induced asystole to facilitate MitraClip placement in a patient with adverse mitral valve morphology. Heart. 2011;97(10):864. Epub 2010 Oct 29.
- Rahimtoola SH. Perspective on valvular heart disease: an update. J Am Coll Cardiol. 1989;14(1):1-23.
___________________________________
From 1the Interventional Cardiology Unit, San Raffaele Scientific Institute, Milan, Italy, 2Vilnius University, Hospital ‘Santariskiu Klinikos,’ Vilnius, Lithuania, 3Interventional Cardiology Unit, EMO-GVM Centro Cuore Columbus, Milan, Italy.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted July 25, 2011, provisional acceptance given August 16, 2011, final version accepted September 8, 2011.
Address for correspondence: Antonio Colombo, MD, PhD, EMO-GVM Centro Cuore Columbus Hospital, via Buonarotti 48, 20145 Milan, Italy. Email: info@emocolumbus.it

