

Gore Helex Septal Occluder for Percutaneous Closure of Patent Foramen Ovale Associated With Atrial Septal Aneurysm: Short- and Mid-Term Clinical and Echocardiographic Outcomes
Abstract: Objectives. To evaluate the short- and mid-term clinical and echocardiographic outcome of HELEX Septal Occluder (HSO) implantation in patients with patent foramen ovale (PFO) and atrial septal aneurysm (ASA). Background. Percutaneous closure of PFO and ASA with HSO device has not been systematically studied. Methods. We studied 90 patients with PFO and ASA with documented paradoxical embolic events. The procedural and clinical results of 30 consecutive patients treated with HSO were compared with those obtained in 30 consecutive patients treated with the Amplatzer PFO (APO) and with those of a further 30 consecutive patients treated with the Amplatzer Cribriform (AMF). Primary endpoint was the persistence of moderate to severe residual right-to-left shunting (rRLS) at 6-month follow-up. The incidence of death or recurrent embolic events (REE) at 1-year follow-up were also investigated. Results. The procedure was successfully completed in all patients. There was one HSO device embolization. Immediate moderate RLS was significantly higher in the HSO group compared to APO and AMF groups (20% vs 3% vs 0%, respectively; P=.008). The incidence of moderate rRLS decreased but was still significant at 6-month follow-up (17% in the HSO group vs 3% in the APO group; P=.02). At 1-year follow-up, moderate rRLS persisted only in the HSO group (7%). No deaths or REE were observed during hospitalization or at 1-year follow-up. Conclusion. HSO device seems to be a second-line device as compared to Amplatzer occluders for the treatment of PFO and ASA.
J INVASIVE CARDIOL 2012;24(10):510-514
Key words: atrial septal aneurysm, atrial septal aneurysm, HSO device, patent foramen ovale
_______________________________________________________
The association of patent foramen ovale (PFO) and atrial septal aneurysm (ASA) identifies a population at high risk of paradoxical embolism. These patients have a three- to five-fold greater risk of recurrent embolic events (REE) as compared to patients with PFO alone1,2 despite anticoagulant or antiplatelet therapy.3-5 Several devices for percutaneous closure of PFO have been developed with a reported incidence of REE of 1%/year; lower than results obtained from medical treatment alone.6-8 Transcatheter closure of PFO in the presence of ASA requires a thorough analysis of interatrial septal morphology in order to select the most appropriate device to achieve maximum effectiveness and minimum device-related complications. The Gore Helex Septal Occluder (HSO) is an approved device for PFO closure, and has not been systematically studied in patients with PFO and associated ASA. The aim of the present study is to investigate the short- and mid-term outcome of this device in a consecutive series of patients with PFO and ASA.
Methods
The study population included 90 patients with PFO with associated ASA and a positive history of paradoxical embolic event who had previously undergone elective closure of the PFO at our institution. From February 2007 to December 2007, 30 consecutive patients were treated by means of an HSO implantation. Their results were compared with those of 30 consecutive patients treated with Amplatzer PFO (APO) device between January 2008 and January 2009 and 30 consecutive patients treated with Amplatzer Cribriform septal occluder (AMF) device between February 2009 and March 2010. The choice of device was made independently from septal morphology or physician preference. Patient demographic and procedural data were prospectively collected. An embolic event was considered to be due to paradoxical embolism when the following criteria were fulfilled: (1) presence of PFO with spontaneous or provoked right-to-left shunting (RLS) during contrast transesophageal echocardiography (TEE); (2) clinically and/or radiographically confirmed ischemic stroke, transient ischemic attack, or peripheral embolism; and (3) exclusion of any other identifiable cardiac, aortic, or cerebrovascular causes. Depending on the case, patient work-ups included neurological examination, brain computed tomography or magnetic resonance imaging (MRI), extracranial Doppler ultrasonography, 12-lead electrocardiogram (ECG), 24-hour blood pressure and ECG monitoring, transthoracic echocardiogram (TTE) with bubble test with and without the Valsalva maneuver, TEE, venous Doppler of lower extremities and hypercoagulable work-ups (including protein C and S, antithrombin III, anticardiolipin antibodies, homocysteine, factor V Leiden, and lupus anticoagulant).
Echocardiographic protocols and definitions. Diagnosis of PFO and ASA was made by a multiplane TEE probe. ASA was defined as the presence of a localized protrusion of the fossa ovalis, with a base width of 15 mm and mobile septum excursion of 10 mm between the two atria. The presence of spontaneous or provoked RLS was documented by contrast TEE with intravenous injection of 10 mL of agitated saline. Bubbles were counted in the left atrium within 3 cardiac cycles after right atrium opacification. Small RLS was defined as 1 to 9 bubbles, moderate RLS as 10 to 20 bubbles, and severe RLS as >20 bubbles passing into the left atrium through the interatrial septum. Moderate and severe RLS were regarded as significant shunts.
Device descriptions and closure protocol. The operators were all experienced with the PFO closure technique. Three devices were used in this study. The HSO device (W.L. Gore and Associates, Inc) is composed of a single piece of nitinol wire to which e-polytetrafluoroethylene (ePTFE) is attached along its entire length and a circular 2-umbrella which, at the time of deployment, bridges and occludes the PFO. An ePTFE retention suture anchored to the tip of the control catheter loops through the right atrial eyelet to hold the occluder on the catheter as it is exteriorized. The suture allows removal of the device, if necessary, after complete deployment and release from the delivery system. Available disc sizes range from 15 mm to 35 mm (5 mm increments). The Amplatzer PFO occluder (APO; AGA Medical) and Amplatzer Cribriform septal occluder (AMF; AGA Medical) are self-expandable devices made of nitinol wire mesh. The AMF is made from two equal-sized discs, whereas the left atrial APO occluder disc is slightly smaller than the right atrial disc. Discs of both devices are connected together by a bond bridge and are available in 18, 25, and 35 mm.
All procedures were carried out under local anesthesia and the size of device was selected using intracardiac echographic (ICE; AcuNav Diagnostic Ultrasound Catheter; Siemens Medical) guidance without balloon sizing. On the day of implantation, 250 mg of intravenous acetylsalicylic acid and a 300 mg loading dose of clopidogrel were administered. Following sheath placement in a femoral vein, 100 units/kg body weight of intravenous unfractionated heparin were administered. After device implantation, all patients received aspirin 100 mg daily and clopidogrel 75 mg daily for 3 months. Thereafter, clopidogrel was discontinued and aspirin therapy maintained for a further 9 months. Standard bacterial endocarditis prophylaxis was recommended for 12 months.
Follow-up. Patients were prospectively followed with clinical examination and transthoracic echocardiography (TTE) at 1, 3, 6, and 12 months after the procedure. Chest x-ray, for detection of fracture of the device, as well as bubble test during TTE, for detection of residual RLS at rest and after the Valsalva maneuver, were performed at 6-month follow-up. Residual RLS was graded according to the definition used for evaluation of the PFO before closure, as described above. In cases of 6-month persistent moderate-severe RLS, contrast TTE was repeated 6 months later. Six-month persistence of moderate-severe RLS was considered the primary endpoint. The incidence of death or REE at 1 year was registered. Patients with suspected cerebral REE were re-evaluated by a senior neurologist and brain MRI was repeated. The need for re-intervention in cases of significant residual RLS or device mal-alignment was also investigated.
Statistical analysis. Categorical variables were compared using a Chi-square or Fisher’s exact test when appropriate. Statistical significance was assumed with a P value <.05. Parametric variables were compared by one-way ANOVA analysis. Statistical analysis was performed using the SPSS (version 12) and SAS (Fisher’s exact test) software.
Results
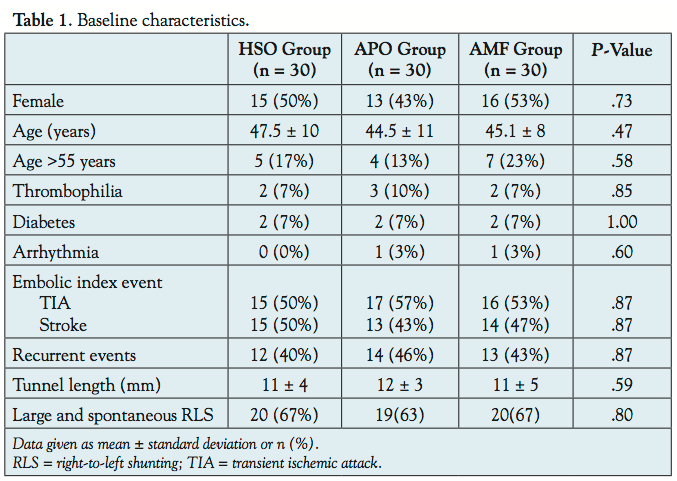 Patient population. Baseline characteristics of patients in each group are outlined in Table 1. No significant differences in terms of embolic risk profile and echocardiographic parameters were observed among the 3 groups. The study population showed high-risk characteristics for REE since all patients had PFO with ASA, the vast majority had large and spontaneous RLS, 43% had >1 embolic events, 18% were older than 55 years, and 8% had a thrombophilic state.
Patient population. Baseline characteristics of patients in each group are outlined in Table 1. No significant differences in terms of embolic risk profile and echocardiographic parameters were observed among the 3 groups. The study population showed high-risk characteristics for REE since all patients had PFO with ASA, the vast majority had large and spontaneous RLS, 43% had >1 embolic events, 18% were older than 55 years, and 8% had a thrombophilic state.
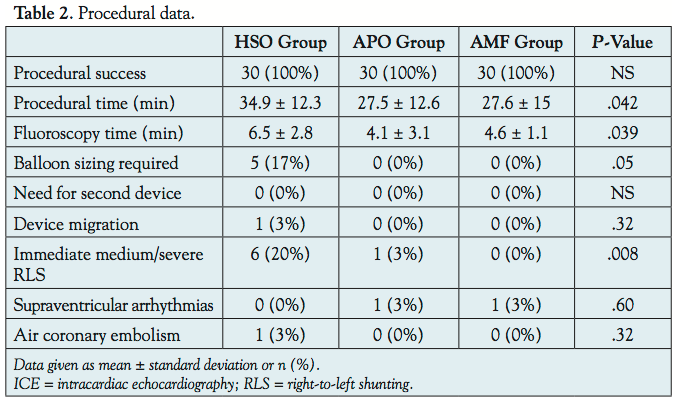 Procedural and in-hospital outcomes. Procedural data are outlined in Table 2. Procedural and fluoroscopy times were significantly higher in the HSO group than in the APO or AMF groups (P=.042 and P=.039, respectively). The procedure was successful in all patients and none needed more than 1 device. In the HSO group, a 25 mm device was implanted in all patients except in 2 who received 30 mm devices. All patients in the AMF group received a 25 mm device except 1 patient in which a 35 mm was used. The APO device size was 25 mm
Procedural and in-hospital outcomes. Procedural data are outlined in Table 2. Procedural and fluoroscopy times were significantly higher in the HSO group than in the APO or AMF groups (P=.042 and P=.039, respectively). The procedure was successful in all patients and none needed more than 1 device. In the HSO group, a 25 mm device was implanted in all patients except in 2 who received 30 mm devices. All patients in the AMF group received a 25 mm device except 1 patient in which a 35 mm was used. The APO device size was 25 mm  in 27 patients and 35 mm in 3 patients. In the HSO group, a 25 mm device migrated to the abdominal aorta 24 hours after the procedure (Figure 1A). This was easily retrieved using a 20 mm snare catheter and removed via a 10 Fr sheath without any complications (Figure 1B). An attempt to implant a 25 mm AMF device was unsuccessful because of its persistent unstable position in the interatrial septum. Thereafter, PFO balloon sizing was performed and a 35 mm AMF was eventually implanted successfully (Figures 1C and 1D). In the HSO group, 4 occluders were retrieved prior to release because of their unsatisfactory constitution and the PFO was subsequently closed using a second HSO device. Immediate moderate-to-severe RLS was more frequent in the HSO group than in the Amplatzer groups (20% vs 3% vs 0%; P=.008). No deaths, REE, cardiac tamponade, or retroperitoneal hematoma were observed during hospitalization. One patient in the APO group and 1 in the AMF group showed a supraventricular arrhythmia that spontaneously converted to a sinus rhythm and 1 patient in the HSO group showed transitory ST-elevation in leads DII, DIII, and aVF caused by air embolism in the right coronary artery, which spontaneously resolved within a few minutes.
in 27 patients and 35 mm in 3 patients. In the HSO group, a 25 mm device migrated to the abdominal aorta 24 hours after the procedure (Figure 1A). This was easily retrieved using a 20 mm snare catheter and removed via a 10 Fr sheath without any complications (Figure 1B). An attempt to implant a 25 mm AMF device was unsuccessful because of its persistent unstable position in the interatrial septum. Thereafter, PFO balloon sizing was performed and a 35 mm AMF was eventually implanted successfully (Figures 1C and 1D). In the HSO group, 4 occluders were retrieved prior to release because of their unsatisfactory constitution and the PFO was subsequently closed using a second HSO device. Immediate moderate-to-severe RLS was more frequent in the HSO group than in the Amplatzer groups (20% vs 3% vs 0%; P=.008). No deaths, REE, cardiac tamponade, or retroperitoneal hematoma were observed during hospitalization. One patient in the APO group and 1 in the AMF group showed a supraventricular arrhythmia that spontaneously converted to a sinus rhythm and 1 patient in the HSO group showed transitory ST-elevation in leads DII, DIII, and aVF caused by air embolism in the right coronary artery, which spontaneously resolved within a few minutes.
 Follow-up. After discharge, all patients were clinically followed for 1 year. No deaths or REEs were recorded among the 3 groups. At 6-month follow-up, no cases of severe RLS were observed, whereas 5 patients (17%) and 1 patient (3%) presented with moderate RLS in the HSO and APO groups, respectively (P=.02; Table 3). At 1-year follow-up, moderate RLS persisted in 2 of the 5 patients from the HSO group, whereas it was no longer present in the patient belonging to the APO group. Minor complaints, including chest discomfort, palpitations, and dyspnea, were present at 1-month follow-up in each group but had disappeared, in most patients, at 6-month follow-up. No device fractures were detected 6 months after the procedure. No patient required re-intervention for significant RLS or device mal-alignment.
Follow-up. After discharge, all patients were clinically followed for 1 year. No deaths or REEs were recorded among the 3 groups. At 6-month follow-up, no cases of severe RLS were observed, whereas 5 patients (17%) and 1 patient (3%) presented with moderate RLS in the HSO and APO groups, respectively (P=.02; Table 3). At 1-year follow-up, moderate RLS persisted in 2 of the 5 patients from the HSO group, whereas it was no longer present in the patient belonging to the APO group. Minor complaints, including chest discomfort, palpitations, and dyspnea, were present at 1-month follow-up in each group but had disappeared, in most patients, at 6-month follow-up. No device fractures were detected 6 months after the procedure. No patient required re-intervention for significant RLS or device mal-alignment.
Discussion
The present investigation compares 3 different PFO closure devices for the treatment of symptomatic patients with PFO and ASA. It demonstrates that the HSO device is burdened by greater incidence of 6-month RLS, requires more time to achieve definitive PFO occlusion, and is technically more difficult to implant than Amplatzer devices.
The combination of PFO and ASA can facilitate paradoxical embolism through several mechanisms: (1) by redirecting the flow from the inferior vena cava toward the PFO; (2) by representing itself an embolic source;9 and (3) by determining mechanical atrial dysfunction as occurs in atrial fibrillation.10 These features make transcatheter closure of PFO a valuable option. However, only a few studies have systematically investigated the percutaneous treatment of PFO with associated ASA6,7 and no dedicated occluder device has been developed. Moreover, the incidence of residual RLS after closure of PFO and ASA is higher in comparison with PFO closure alone,11,12 whichever implantation technique is employed (covering and stabilizing the entire septum or using a malleable device conforming to the anatomy of ASA). In our series of consecutive patients with PFO and ASA, we found that the clinical results of HSO compare favorably with those of Amplatzer devices: the HSO was successfully deployed in all patients and no deaths or REEs were registered at 1-year follow-up.
We confirm that the presence of ASA is associated with higher rates of RLS after transcatheter PFO occlusion, this finding being more notable after HSO than after Amplatzer device implantation. In the HSO group, 20% of patients had significant immediate residual RLS, which decreased to 17% at 6 months and to 7% at 1-year follow-up. In the Amplatzer groups, moderate residual RLS was present in 1.6% of patients at 6 months and remained unchanged at 12-month follow-up. Accordingly, PFO occlusion after HSO device implantation appears not to be instantaneous but progressive and the difference in residual RLS rates between HSO and Amplatzer occluders may decrease with time. The reasons for the differences in definite occlusion time after device implantation are unclear. The best hypothesis is that the endothelialization process may be faster in more rigid occluders due to their ability to “button” and oppose the septum primum more closely. This process might be delayed with softer devices such as the HSO, because of the increased separation of the discs, particularly in the presence of hypermobile interatrial septum, such as in patients with ASA. However, the hypothesis of an increased risk of re-events due to a residual RLS has not been established.13,14 We did not find any differences in terms of REE rates at 1-year follow-up among the 3 groups of patients despite the higher persistence of residual RLS in the HSO group.
In accordance with a previous investigation,15 we found that the HSO device is implanted with greater difficulty than Amplatzer devices. In fact, the fluoroscopy and procedural times were significantly higher in the HSO group. Only in the HSO patients did the occluder require removal due to its incorrect position on the interatrial septum and subsequent implantation of another occluder. The most frequent technical difficulty was that the right atrial hook did not grasp the eyelet. Moreover, the only case of device embolization in our series was recorded in the HSO group, but this was easily and uneventfully retrieved. It is unlikely that the mechanism of embolization was entirely device-related, because the PFO balloon sizing disclosed a tunnel width larger than measured at baseline and therefore a larger device was successfully implanted. We did not find any cases of HSO wire frame fracture, but it should be noted that this has more often been associated with larger devices.16 In conclusion, the HSO is a very flexible device designed to conform to the contours of the septum without bulky protrusion into the atria. These features may increase the possibility of device embolization, but at the same time reduce the risks of cardiac or vascular erosion and perforation while allowing for safe and easy device retrieval.
As the combination of PFO and ASA identifies a high-risk population for REE, appropriate device selection through an accurate morphological evaluation of the interatrial septum is very important. It is mandatory that the interventional cardiology team has a thorough knowledge of TEE or ICE findings in order to choose devices according to septum anatomy and, as a consequence, to minimize device-related complications.
Study limitations. The results of the present study have some limitations. First, it is a small and non-randomized study, although it is a comparison of “real life” consecutive clinical series of 3 different devices whose choice was operator-independent. Second, the study follow-up was limited to 1 year. However, most studies indicate that REE occurred early after percutaneous treatment.17 Third, although we found no differences in the rates of REE, the study does not have sufficient power to show any differences in clinical events. Fourth, the work studied a consecutive series of patients with PFO and ASA treated with 3 different devices independent of anatomical characteristics of the interatrial septum. Conversely, the most appropriate management should be tailored according to the anatomic characteristics of the individual patient.
Conclusion
HSO device seems to be the second-line device as compared to the Amplatzer occluders for the treatment of PFO and ASA, although device- and procedure-related complications are rare and mid-term clinical results are reassuring. HSO is more technically difficult to manage, there is a greater presence of moderate RLS during the follow-up, and more time is required to complete PFO occlusion than with Amplatzer devices. Large, randomized trials are needed in the future to determine the safety and the efficacy of the HSO device.
References
- Agmon Y, Khandheria BK, Meissner I, et al. Frequency of atrial septal aneurysms in patients with cerebral ischemic events. Circulation. 1999;99(15):1942-1944.
- Mas JL, Arquizan C, Lamy C, et al. Recurrent cerebrovascular events associated with patent foramen ovale, atrial septal aneurysm, or both. N Engl J Med. 2001;345(24):1740-1746.
- Di Tullio MR, Sacco RL, Sciacca RR, et al. Patent foramen ovale and risk of ischemic stroke in a multiethnic population. J Am Coll Cardiol. 2007;49(7):797-802.
- Mas JL, Zuber M. Recurrent cerebrovascular events in patients with patent foramen ovale, atrial septal aneurysm, or both and cryptogenic stroke or transient ischemic attack. French Study Group on Patent Foramen Ovale and Atrial Septal Aneurysm. Am Heart J. 1995;130(5):1083-1088.
- Messe SR, Silverman IE, Kizer JR, et al. Practice parameter: recurrent stroke with patent foramen ovale and atrial septal aneurysm: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2004;62(7):1042-1050.
- Musto C, Cifarelli A, Pandolfi C, et al. Transcatheter closure of patent foramen ovale associated with atrial septal aneurysm with Amplatzer cribiform septal occluder. J Invasive Cardiol. 2009;21(6):290-293.
- Wahl A, Krumsdorf U, Meier B, et al. Transcatheter treatment of atrial septal aneurysm associated with patent foramen ovale for prevention of recurrent paradoxical embolism in high-risk patients. J Am Coll Cardiol. 2005;45(3):377-380.
- Bruch L, Parsi A, Grad MO, et al. Transcatheter closure of interatrial communications for secondary prevention of paradoxical embolism: single-center experience. Circulation. 2002;105(24):2845-2848.
- De Castro S, Cartoni D, Fiorelli M, et al. Morphological and functional characteristics of patent foramen ovale and their embolic implications. Stroke. 2000;31(10):2407-2413.
- Rigatelli G, Aggio S, Cardaioli P, et al. Left atrial dysfunction in patients with patent foramen ovale and atrial septal aneurysm. An alternative concurrent mechanism for arterial embolism? JACC Cardiovasc Interv. 2009;2(7):655-662.
- Windecker S, Wahl A, Chatterjee T, et al. Percutaneous closure of patent foramen ovale in patients with paradoxical embolism: long-term risk of recurrent thromboembolic events. Circulation. 2000;101(8):893-898.
- Thaman R, Faganello G, Gimeno JR, et al. Efficacy of percutaneous closure of patent foramen ovale: comparison among three commonly used occluders. Heart. 2011;97(5):394-399.
- von Bardeleben RS, Richter C, Otto G, et al. Long-term follow-up after percutaneous closure of PFO in 357 patients with paradoxical embolism: difference in occlusion systems and influence of atrial septum aneurysm. Int J Cardiol. 2009;134(1):33-41.
- Windecker S, Wahl A, Nedelchev K, et al. Comparison of medical treatment with percutaneous closure of patent foramen ovale in patients with cryptogenic stroke. J Am Coll Cardiol. 2004;44(4):750-758.
- Taaffe M, Fisher E, Baranowsky A, et al. Comparison of three patent foramen ovale closure devices in a randomized trial (Amplatzer versus CardioSEAL-STARflex versus Helex occluder). Am J Cardiol. 2008;101(9):1353-1358.
- Fagan T, Dreher D, Cutright W, et al. GORE HELEX Septal Occluder Working group. Fracture of the GORE HELEX Septal Occluder: associated factors and clinical outcomes. Catheter Cardiovasc Interv. 2009;73(7):941-948.
- Martin F, Sanchez PL, Doherty E, et al. Percutaneous transcatheter closure of patent foramen ovale in patients with paradoxical embolism. Circulation. 2002;106(9):1121-1126.
_______________________________________________________
From the Interventional Cardiology Unit, San Camillo Hospital, Rome, Italy.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted February 15, 2012, provisional acceptance given March 29, 2012, final version accepted May 10, 2012.
Address for correspondence: Carmine Musto MD, PhD, San Camillo Hospital Interventional cardiology, Via circonvallazione gianicolense, 87, 00152 Rome, Italy. Email: cmusto@hotmail.it

