

Gender Differences in Long-Term Clinical Outcomes After Percutaneous Coronary Intervention of Chronic Total Occlusions
Abstract: Introduction. Little is known about gender differences among patients undergoing percutaneous coronary intervention (PCI) for chronic total occlusion (CTO). Methods. A total of 1791 patients with 1852 CTOs underwent PCI at 3 centers in the United States, Italy, and South Korea between 1998 and 2007. We compared baseline characteristics, procedural success rates (residual stenosis <50%), and 5-year clinical event rates in male and female patients. Results. A total of 1534 men (86%) and 248 women (14%) were treated. After multivariate adjustment, procedural success rates were similar in men and women. The median follow-up duration was 2.9 years (interquartile range, 1.5-4.6 years). Successful CTO PCI was associated with reduced mortality (5.7% vs 9.2%; P<.01) and a reduced need for coronary artery bypass graft (CABG) surgery (3.1% vs 14.1%; P<.01) in male patients. In female patients, there was a trend toward a lower need for CABG after successful CTO PCI (4.0% vs 6.9%; P=.09). Rates of major adverse cardiac events (MACE; death, myocardial infarction, and CABG) were lower after successful PCI in both men and women (men, 13.1% vs 24.4% and P<.01; women, 12.3% vs 15.5% and P=.04). There was a significant interaction between gender and procedural success in terms of MACE (P<.01), indicating men had a greater reduction in MACE rate after successful CTO PCI compared with women. Conclusion. Our study suggested a greater benefit of a successful CTO intervention in men compared with women. A minority of patients (14%) were women. CTO PCI in women is safe and feasible and should probably be considered more often. A randomized controlled trial is needed to accurately investigate the impact of CTO PCI in both men and women.
J INVASIVE CARDIOL 2012;24(10):484-488
Key words: chronic total occlusion, gender
___________________________________________________
Coronary chronic total occlusion (CTO) is detected on diagnostic coronary angiography in approximately 30% of patients.1,2 However, only an estimated 15% of patients with a CTO undergo an attempt to revascularize a CTO by percutaneous coronary intervention (PCI) and patients are often referred for bypass surgery.1 A number of advances in guidewire, microcatheter and drug-eluting stent (DES) technology have made these notoriously complex lesions realistic targets for PCI. Recent meta-analyses and large registries have shown that successful CTO PCI is associated with symptom relief, a reduction in long-term mortality, and a lower need for coronary artery bypass graft (CABG) surgery.3,4
Currently, there are no studies investigating the impact of gender on clinical outcomes after PCI of CTOs. Results of clinical studies investigating differences in outcomes after PCI in male and female patients have yielded inconclusive results.5-9 Therefore, we investigated the impact of gender on long-term clinical outcomes after CTO PCI in the large Multinational CTO Registry.
Methods
All patients who underwent PCI for at least one CTO at three tertiary care hospitals between 1998 and 2007 were included in this study. CTO was defined as a coronary artery obstruction with a Thrombolysis in Myocardial Infarction (TIMI) flow grade 0. All patients included had a native vessel occlusion estimated to be at least 3 months in duration based on either a history of sudden chest pain, a previous myocardial infarction in the same target vessel territory, or the time between diagnosis made on coronary angiography and PCI. All patients had symptomatic angina and/or a positive functional ischemia study.
PCI and stent implantation were performed in a standard manner. Heparin was administered to maintain an activated clotting time >250 seconds. The use of bare-metal stents (BMS) or DES as well as the use of glycoprotein IIb/IIIa inhibitors was left to the discretion of the treating physician. CTO PCI was performed using contemporary techniques such as bilateral injection, specialized hydrophilic, tapered tip and stiff wires, parallel wires, microcatheters, and retrograde approach when they became available. After PCI, all patients were prescribed lifelong aspirin. In addition, clopidogrel was prescribed for at least 3 months after DES implantation in Italy and South Korea and for at least 12 months in the United States, and for at least 1 month after BMS implantation in all participating sites.
Demographic, angiographic, and procedural data regarding all patients undergoing PCI at the three participating centers (n = 1791) were prospectively entered into a dedicated database. Patients were followed prospectively by telephone interview or outpatient visit after 30 days, and yearly thereafter. Demographic, angiographic, procedural, and follow-up data were subsequently merged in the multinational CTO registry, containing all data contributed by the three participating centers. The following endpoints were analyzed in men and women with successful vs failed CTO PCI: all-cause mortality, myocardial infarction (MI), and need for CABG at 5-year follow-up. Additionally, we evaluated a composite endpoint of major adverse cardiovascular events (MACE), consisting of all-cause mortality, MI, and CABG. Endpoint definitions have been previously published in detail.4Multivessel disease was defined as the presence of at least 1 stenosis ≥70% by visual assessment in a major epicardial vessel or its side branches other than where the CTO was located. Procedural success was defined as successful recanalization and dilatation of at least 1 CTO per patient with or without stent implantation, residual stenosis of <50%, and TIMI flow >2.
Statistical analysis. Data are presented as mean ± standard deviation or percentages. Event rates were estimated using the Kaplan-Meier method. Follow-up was censored at date of last follow-up or at 5 years, whichever came first. Survival curves using all available follow-up data were constructed for time-to-event variables using Kaplan-Meier methodology. Event rates were compared by log-rank test. Multivariable logistic regression was performed to identify predictors of CTO PCI failure, with the following potential co-variables included: gender (women vs men); CTO length; CTO location; bridging collaterals; blunt stump; side branch proximal to CTO, and calcification. Formal interaction tests were performed to determine whether gender affected the relative risk of mortality or the need for CABG surgery after successful versus failed PCI. Statistical analyses were performed using SPSS version 17.0 (SPSS Inc).
Results
 Figure 1 shows the patient flow in the multinational CTO registry. Of 1791 patients, 248 were female (14%) and 1543 were male (86%). Table 1 shows baseline demographic, angiographic, and procedural characteristics of male and female patients undergoing attempted CTO PCI. Female patients were older, more often had hypertension and diabetes mellitus, and were less frequently smokers compared with male patients. Moreover, female patients less often had multivessel disease and more often had CTOs located in the left anterior descending (LAD) coronary artery. Procedural success was more frequent in female patients. On the other hand, they also had shorter CTO lengths, and less often blunt stumps and bridging collaterals. Table 2 shows independent predictors of CTO PCI failure. After multivariable adjustment for known predictors of CTO PCI failure, gender was not associated with CTO PCI failure.
Figure 1 shows the patient flow in the multinational CTO registry. Of 1791 patients, 248 were female (14%) and 1543 were male (86%). Table 1 shows baseline demographic, angiographic, and procedural characteristics of male and female patients undergoing attempted CTO PCI. Female patients were older, more often had hypertension and diabetes mellitus, and were less frequently smokers compared with male patients. Moreover, female patients less often had multivessel disease and more often had CTOs located in the left anterior descending (LAD) coronary artery. Procedural success was more frequent in female patients. On the other hand, they also had shorter CTO lengths, and less often blunt stumps and bridging collaterals. Table 2 shows independent predictors of CTO PCI failure. After multivariable adjustment for known predictors of CTO PCI failure, gender was not associated with CTO PCI failure.
 Baseline clinical, angiographic, and procedural characteristics of male and female patients stratified according to procedural success are shown in Table 1. Women with a successful procedure less often had prior CABG, multivessel disease, and coronary perforations compared to women with a failed procedure. The presence of a side branch proximal to the CTO was more common in women with a successful procedure. Men with a successful procedure were younger and were less likely to be smokers, have hypercholesterolemia, have multivessel disease, or have had a prior MI or prior CABG compared with men with a failed procedure. Furthermore, men with a successful procedure had a shorter CTO lesion length, more often a CTO located in the LAD coronary artery and less often in the right coronary artery, less often blunt stumps, bridging collaterals, dissections, and coronary perforations.
Baseline clinical, angiographic, and procedural characteristics of male and female patients stratified according to procedural success are shown in Table 1. Women with a successful procedure less often had prior CABG, multivessel disease, and coronary perforations compared to women with a failed procedure. The presence of a side branch proximal to the CTO was more common in women with a successful procedure. Men with a successful procedure were younger and were less likely to be smokers, have hypercholesterolemia, have multivessel disease, or have had a prior MI or prior CABG compared with men with a failed procedure. Furthermore, men with a successful procedure had a shorter CTO lesion length, more often a CTO located in the LAD coronary artery and less often in the right coronary artery, less often blunt stumps, bridging collaterals, dissections, and coronary perforations.
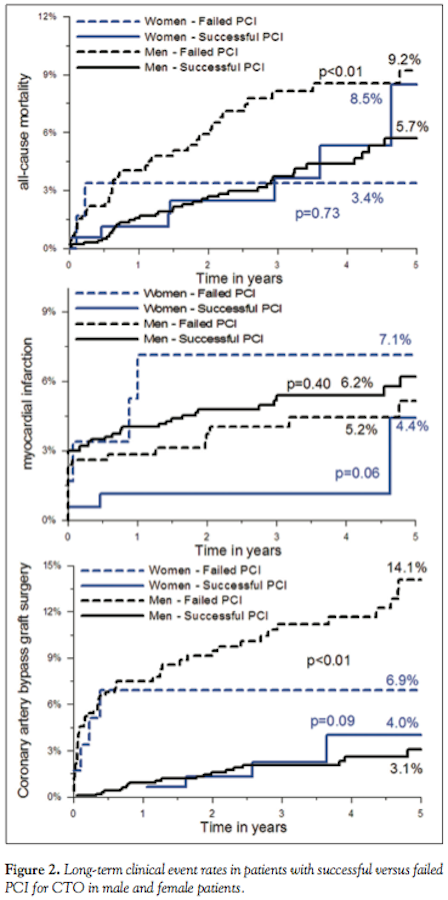
 Median follow-up in this cohort was 2.9 years (interquartile range, 1.5-4.6 years). Five-year mortality, MI, and CABG rates after failed and successful CTO PCI according to gender are shown in Figure 1. Mortality rates after failed and successful CTO PCI were similar in female patients. Among males, a successful CTO PCI was associated with reduced 5-year mortality. There were no differences in long-term MI rates in patients with failed compared with successful procedures in either gender. The need for CABG surgery was higher after a failed procedure in either gender, but this difference was only statistically significant in male patients. There was no significant interaction between gender and procedural success in terms of 5-year mortality (P=.63) or need for CABG (P=.42). Five-year MACE rates after successful vs unsuccessful CTO PCI in women were 12.3% vs 15.5% (P=.04). Five-year MACE rates in successful vs unsuccessful CTO PCI in men were 13.1% vs 24.4% (P<.01). There was a significant interaction between gender and procedural success in terms of MACE (P<.01), indicating men had a greater reduction in MACE after successful CTO PCI compared with women.
Median follow-up in this cohort was 2.9 years (interquartile range, 1.5-4.6 years). Five-year mortality, MI, and CABG rates after failed and successful CTO PCI according to gender are shown in Figure 1. Mortality rates after failed and successful CTO PCI were similar in female patients. Among males, a successful CTO PCI was associated with reduced 5-year mortality. There were no differences in long-term MI rates in patients with failed compared with successful procedures in either gender. The need for CABG surgery was higher after a failed procedure in either gender, but this difference was only statistically significant in male patients. There was no significant interaction between gender and procedural success in terms of 5-year mortality (P=.63) or need for CABG (P=.42). Five-year MACE rates after successful vs unsuccessful CTO PCI in women were 12.3% vs 15.5% (P=.04). Five-year MACE rates in successful vs unsuccessful CTO PCI in men were 13.1% vs 24.4% (P<.01). There was a significant interaction between gender and procedural success in terms of MACE (P<.01), indicating men had a greater reduction in MACE after successful CTO PCI compared with women.
Discussion
 This analysis from the large Multinational CTO Registry studied the largest cohort of female patients undergoing CTO PCI to date and showed that after multivariate adjustment, success rates of CTO PCI are similar in men and women. Moreover, successful CTO PCI was associated with reduced need for CABG and reduced mortality in male patients. In women, successful CTO PCI was associated with a statistical trend toward less CABG surgery. The long-term occurrence of MACE was reduced after successful PCI in both men and women. However, we observed a significant interaction between gender and procedural success in terms of MACE, indicating men may have greater benefit of successful percutaneous revascularization of a CTO.
This analysis from the large Multinational CTO Registry studied the largest cohort of female patients undergoing CTO PCI to date and showed that after multivariate adjustment, success rates of CTO PCI are similar in men and women. Moreover, successful CTO PCI was associated with reduced need for CABG and reduced mortality in male patients. In women, successful CTO PCI was associated with a statistical trend toward less CABG surgery. The long-term occurrence of MACE was reduced after successful PCI in both men and women. However, we observed a significant interaction between gender and procedural success in terms of MACE, indicating men may have greater benefit of successful percutaneous revascularization of a CTO.
 Consistent with previous reports, women in the current study were older, presumably because of the protective effects against coronary atherosclerosis of estrogen until menopause.10 The current study showed that CTO PCI in women was safe and feasible, with similar success rates to men. However, only a small minority of patients (13.8%) in the current study were female. This observation is consistent with previous studies suggesting women are less likely to undergo treatment of coronary artery disease.11,12 For example, a recent study by Chan et al of over 140,000 PCI procedures in the United States using the National Cardiovascular Data Registry showed that about 1 in 3 overall PCIs were performed in women.13 In the present study, only 1 in 7 CTO PCIs were performed in women. The recent development of novel interventional techniques developed specifically for CTOs, such as the retrograde approach and novel devices, guidewires, and catheters, have led to a higher CTO PCI success rate. Several studies have shown a potential improvement in survival after CTO PCI and improvement of left ventricular function, freedom from angina, and less need for CABG after successful CTO PCI have been well established. Therefore, our data suggest that PCI should probably be considered more often in women with CTOs.3,14,15
Consistent with previous reports, women in the current study were older, presumably because of the protective effects against coronary atherosclerosis of estrogen until menopause.10 The current study showed that CTO PCI in women was safe and feasible, with similar success rates to men. However, only a small minority of patients (13.8%) in the current study were female. This observation is consistent with previous studies suggesting women are less likely to undergo treatment of coronary artery disease.11,12 For example, a recent study by Chan et al of over 140,000 PCI procedures in the United States using the National Cardiovascular Data Registry showed that about 1 in 3 overall PCIs were performed in women.13 In the present study, only 1 in 7 CTO PCIs were performed in women. The recent development of novel interventional techniques developed specifically for CTOs, such as the retrograde approach and novel devices, guidewires, and catheters, have led to a higher CTO PCI success rate. Several studies have shown a potential improvement in survival after CTO PCI and improvement of left ventricular function, freedom from angina, and less need for CABG after successful CTO PCI have been well established. Therefore, our data suggest that PCI should probably be considered more often in women with CTOs.3,14,15
Interestingly, the current analysis showed only a survival benefit after successful CTO PCI in male patients. One possible explanation may be the limited sample size of the female cohort in the current study. Moreover, gender has been entered as a covariate in multivariate Cox proportional hazards models for mortality in a previous publication from the Multinational CTO Registry, and turned out not to be independently associated with mortality.4
A number of well-designed, randomized, controlled trials have recently been initiated to investigate a potential benefit of CTO PCI, such as EXPLORE (Evaluating Xience V and Left Ventricular Function in Percutaneous Coronary Intervention on Occlusions after ST-Elevation Myocardial Infarction),16 DECISION-CTO (Drug-Eluting Stent Implantation Versus Optimal Medical Treatment in Patients with Chronic Total Occlusion), and the EURO-CTO trial (European Study on the Utilization of Revascularization versus Optimal Medical Therapy for the Treatment of Chronic Total Coronary Occlusions). Post hoc analyses of these studies will provide additional important insights into gender differences in CTO PCI.
Study limitations. Limitations of the Multinational CTO Registry have been previously published. Importantly, this study is limited by its observational nature and by the relatively low number of women included. Nonetheless, we studied the largest cohort of women undergoing CTO PCI to date. An adequately powered randomized controlled trial is warranted to investigate clinical outcomes after CTO PCI in both men and women. Until such a trial has been performed, the current study suggests CTO PCI is currently underutilized in women.
Conclusion
Our study suggested a greater benefit of a successful CTO intervention in men compared with women. A minority of patients (14%) were women. CTO PCI in women is safe and feasible and should probably be considered more often. A randomized controlled trial is needed to accurately investigate the impact of CTO PCI in both men and women.
References
- Grantham JA, Marso SP, Spertus J, et al. Chronic total occlusion angioplasty in the United States. JACC Cardiovasc Interv. 2009;2(6):479-486.
- Cohen HA, Williams DO, Holmes DR Jr, et al. Impact of age on procedural and 1-year outcome in percutaneous transluminal coronary angioplasty: a report from the NHLBI Dynamic Registry. Am Heart J. 2003;146(3):513-519.
- Joyal D, Afilalo J, Rinfret S. Effectiveness of recanalization of chronic total occlusions: a systematic review and meta-analysis. Am Heart J. 2010;160(1):179-187.
- Mehran R, Claessen BE, Godino C, et al. Long-term outcome of percutaneous coronary intervention for chronic total occlusions. JACC Cardiovasc Interv. 2011;4(9):952-961.
- Argulian E, Patel AD, Abramson JL, et al. Gender differences in short-term cardiovascular outcomes after percutaneous coronary interventions. Am J Cardiol. 2006;98(1):48-53.
- Cowley MJ, Mullin SM, Kelsey SF, et al. Sex differences in early and long-term results of coronary angioplasty in the NHLBI PTCA Registry. Circulation. 1985;71(1):90-97.
- Malenka DJ, O’Connor GT, Quinton H, et al. Differences in outcomes between women and men associated with percutaneous transluminal coronary angioplasty. A regional prospective study of 13,061 procedures. Northern New England Cardiovascular Disease Study Group. Circulation. 1996;94(9 Suppl):II99-II104.
- Lansky AJ, Mehran R, Cristea E, et al. Impact of gender and antithrombin strategy on early and late clinical outcomes in patients with non-ST-elevation acute coronary syndromes (from the ACUITY trial). Am J Cardiol. 2009;103(9):1196-1203.
- Parikh PB, Jeremias A, Naidu SS, et al. Effect of gender and race on outcomes in dialysis-dependent patients undergoing percutaneous coronary intervention. Am J Cardiol. 2011;107(9):1319-1323.
- Lansky AJ, Hochman JS, Ward PA, et al. Percutaneous coronary intervention and adjunctive pharmacotherapy in women: a statement for healthcare professionals from the American Heart Association. Circulation. 2005;111(7):940-953.
- Peterson ED, Shah BR, Parsons L, et al. Trends in quality of care for patients with acute myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am Heart J. 2008;156(6):1045-1055.
- Perez-Vizcayno MJ, Hernandez-Antolin RA, Alfonso F, et al. [Changes in percutaneous coronary intervention over the last 20 years: demographic, epidemiologic and clinical characteristics, techniques, and outcomes]. Rev Esp Cardiol. 2007;60(9):932-942.
- Chan PS, Patel MR, Klein LW, et al. Appropriateness of percutaneous coronary intervention. JAMA. 2011;306(1):53-61.
- Grantham JA, Jones PG, Cannon L, et al. Quantifying the early health status benefits of successful chronic total occlusion recanalization: results from the FlowCardia’s Approach to Chronic Total Occlusion Recanalization (FACTOR) Trial. Circ Cardiovasc Qual Outcomes. 2010;3(3):284-290.
- Sirnes PA, Myreng Y, Molstad P, et al. Improvement in left ventricular ejection fraction and wall motion after successful recanalization of chronic coronary occlusions. Eur Heart J. 1998;19(2):273-281.
- van der Schaaf RJ, Claessen BE, Hoebers LP, et al. Rationale and design of EXPLORE: a randomized, prospective, multicenter trial investigating the impact of recanalization of a chronic total occlusion on left ventricular function in patients after primary percutaneous coronary intervention for acute ST-elevation myocardial infarction. Trials. 2010;11:89.
___________________________________________________
From the 1Cardiovascular Research Foundation, New York, New York, 2Academic Medical Center – University of Amsterdam, the Netherlands, 3San Raffaele Scientific Institute, Milan, Italy, 4Mount Sinai Medical Center, New York, New York, 5Asan Medical Center, Seoul, South Korea, 6Columbia University Medical Center New York, New York, 7Royal Brompton Hospital & Imperial College, London, United Kingdom.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Moses is a consultant for Boston Scientific and Abbott Corporation. Dr Stone reports Consultant positions at Osprey, Reva, Merck, Boston Scientific, Abbott Vascular, Evalve, AstraZeneca, Eli-Lilly - Daiichi Sankyo partnership, Bristol-Myers Squibb Sanofi partnership, Otsuka, The Medicines Company, Ortho-McNeil, Gilead, InspireMD, TherOx, Atrium, Volcano, InfraReDx, Medtronic, Genentech, GlaxoSmithKlein, Miracor, MPP group, Lutonix, Velomedix, and CSI; honoraria from Edwards and Vascular Solutions; and stock and/or stock options with CoreValve, Savacor, Biostar I and II funds, MedFocus I, II and Accelerator funds, Caliber, FlowCardia, Ovalum, MediGuide, Guided Delivery Systems, Arstasis, Micardia, AccessClosure, Embrella, and VNT.
Manuscript submitted February 21, 2012, provisional acceptance given April 4, 2012, final version accepted May 30, 2012.
Address for correspondence: Roxana Mehran, MD, Cardiovascular Institute, Mount Sinai Medical Center, One Gustav L. Levy Place (Box 1030), New York, NY 10029. Email: rmehran@crf.org

