

Exclusion of Infected Pseudoaneurysm of Modified Blalock Taussig Shunt Using a Covered Stent
View the video clip from this article in the multimedia section at https://invasivecardiology.com/content/exclusion-infected-pseudoaneurysm-modified-blalock-taussig-shunt-using-covered-stent.
ABSTRACT: A pseudoaneurysm due to infection after a modified Blalock-Taussig shunt is a rare but potentially fatal complication that can rupture, compress mediastinal structures, produce shunt occlusion, and bacteremia. In these patients, medical management of endocarditis is often incomplete because of the presence of prosthetic material and requires the take down of the shunt, most often by surgery, which can be technically challenging. We outline the use of a covered stent to exclude pseudoaneurysm from circulation.
J INVASIVE CARDIOL 2012;24(5):E93-E95
Key words: percutaneous closure, covered stent, false aneurysm
_____________________________________________
Modified Blalock-Taussig (BT) shunt is a palliative surgical procedure that can get complicated due to an infected pseudoaneurysm. This case highlights that successful non-surgical exclusion of a pseudoaneurysm is possible with favorable results.
 Case report. A 6-year-old female patient underwent a left modified BT shunt 1 year prior and presented with recurrent fever for the last 6 months. She was febrile, cyanotic (saturating 66% in room air) with ascites, bilateral pedal edema, and mild icterus. 2D echocardiogram revealed situs solitus, dextrocardia, double outlet right ventricle, multiple ventricular septal defects, severe infundibular stenosis, no atrioventricular valve regurgitation, and 2 cm mobile vegetation on pulmonary valve with a patent BT shunt, confluent
Case report. A 6-year-old female patient underwent a left modified BT shunt 1 year prior and presented with recurrent fever for the last 6 months. She was febrile, cyanotic (saturating 66% in room air) with ascites, bilateral pedal edema, and mild icterus. 2D echocardiogram revealed situs solitus, dextrocardia, double outlet right ventricle, multiple ventricular septal defects, severe infundibular stenosis, no atrioventricular valve regurgitation, and 2 cm mobile vegetation on pulmonary valve with a patent BT shunt, confluent  pulmonary arteries, dilated proximal subclavian artery, circumferential pericardial effusion, and normal ventricular function. Computed tomographic (CT) angiogram was performed to delineate the BT shunt and pseudoaneurysm, which showed multiple heterogeneous densities in the BT shunt along with aneurysmal dilatation of proximal left subclavian artery. She had anemia, leukocytosis, and bacteremia. She was stabilized with inhaled oxygen, inotropes, and diuretics. Her blood cultures were taken, which grew Pneumococci. Her presumed source of infection was thought to be pneumonia, but could not be identified clearly as it was an overseas patient.
pulmonary arteries, dilated proximal subclavian artery, circumferential pericardial effusion, and normal ventricular function. Computed tomographic (CT) angiogram was performed to delineate the BT shunt and pseudoaneurysm, which showed multiple heterogeneous densities in the BT shunt along with aneurysmal dilatation of proximal left subclavian artery. She had anemia, leukocytosis, and bacteremia. She was stabilized with inhaled oxygen, inotropes, and diuretics. Her blood cultures were taken, which grew Pneumococci. Her presumed source of infection was thought to be pneumonia, but could not be identified clearly as it was an overseas patient.
She was treated with intravenous crystalline penicillin, gentamicin, and rifampicin but the fever and bacteremia persisted after 3 weeks of antibiotics. She was taken for cardiac catheterization to delineate the infected pseudoaneurysm, possibly exclude it from circulation, and assess the suitability for bidirectional Glenn operation.
 The femoral artery and vein were percutaneously cannulated. Unfractionated heparin (100 units/kg) was administered after vascular access was obtained. Her mean pulmonary artery (PA) pressure was 17 mm Hg; pulmonary vascular resistance (indexed to body surface area) was 2.2 Wood units • m2; and left ventricular end diastolic pressure was 12 mm Hg. PA angiogram in anteroposterior view and left anterior oblique 30⁰with 10⁰cranial angulation showed good sized confluent PAs (right pulmonary artery: 11 mm; left pulmonary artery:
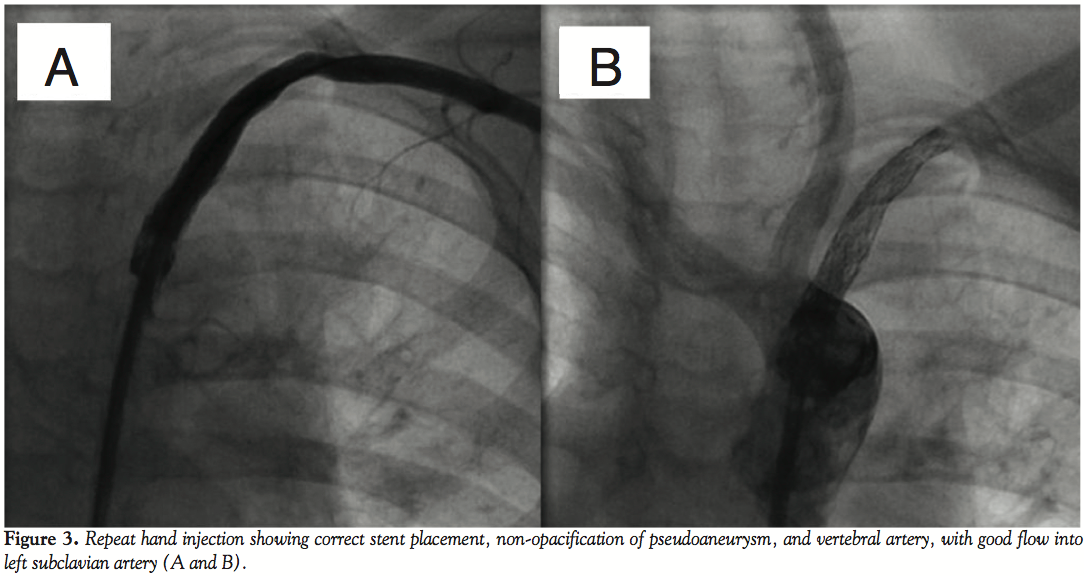
The femoral artery and vein were percutaneously cannulated. Unfractionated heparin (100 units/kg) was administered after vascular access was obtained. Her mean pulmonary artery (PA) pressure was 17 mm Hg; pulmonary vascular resistance (indexed to body surface area) was 2.2 Wood units • m2; and left ventricular end diastolic pressure was 12 mm Hg. PA angiogram in anteroposterior view and left anterior oblique 30⁰with 10⁰cranial angulation showed good sized confluent PAs (right pulmonary artery: 11 mm; left pulmonary artery:  11 mm) without any distortion. A 5 Fr multipurpose catheter was introduced through right femoral artery to aorta to left subclavian artery (LSA). Hand injection in anteroposterior view showed corrugated and irregular luminal surface of BT shunt with pseudoaneurysm at the origin of LSA (Figure 1, Video 1). We performed a 4-vessel angiogram to ascertain the patency of the carotid and vertebral arteries. We introduced a 0.035” extrastiff wire through the multipurpose catheter, which was lodged in the LSA, and tracked a 7 Fr sheath over it. A 6 mm x 16 mm Advanta V12 balloon expandable covered stent (Atrium Medical) was introduced through the long sheath to occlude the mouth of the pseudoaneurysm, but it was not correctly deployed. A longer balloon expandable covered stent (Advanta V12 6 mm x 38 mm, Atrium Medical) was deployed to exclude the pseudoaneurysm (Figure 2, Video 2). Repeat hand injection showed correct stent placement with good flow into LSA, nonopacification of vertebral artery and the pseudoaneurysm (Figures 3A and 3B, Video 3). Chest radiograph and CT scan showed good stent position (Figure 4). Antibiotics were continued for 2 more weeks. Patient showed dramatic clinical improvement and was taken for bilateral bidirectional Glenn operation, main pulmonary artery interruption, and excision of the pulmonary valve with vegetation. She recovered well and was discharged.
11 mm) without any distortion. A 5 Fr multipurpose catheter was introduced through right femoral artery to aorta to left subclavian artery (LSA). Hand injection in anteroposterior view showed corrugated and irregular luminal surface of BT shunt with pseudoaneurysm at the origin of LSA (Figure 1, Video 1). We performed a 4-vessel angiogram to ascertain the patency of the carotid and vertebral arteries. We introduced a 0.035” extrastiff wire through the multipurpose catheter, which was lodged in the LSA, and tracked a 7 Fr sheath over it. A 6 mm x 16 mm Advanta V12 balloon expandable covered stent (Atrium Medical) was introduced through the long sheath to occlude the mouth of the pseudoaneurysm, but it was not correctly deployed. A longer balloon expandable covered stent (Advanta V12 6 mm x 38 mm, Atrium Medical) was deployed to exclude the pseudoaneurysm (Figure 2, Video 2). Repeat hand injection showed correct stent placement with good flow into LSA, nonopacification of vertebral artery and the pseudoaneurysm (Figures 3A and 3B, Video 3). Chest radiograph and CT scan showed good stent position (Figure 4). Antibiotics were continued for 2 more weeks. Patient showed dramatic clinical improvement and was taken for bilateral bidirectional Glenn operation, main pulmonary artery interruption, and excision of the pulmonary valve with vegetation. She recovered well and was discharged.
Discussion. False aneurysms develop due to thrombosed prosthetic grafts, which become a site of chronic infection. The patient with infected pseudoaneurysms of BT shunt usually presents with fever owing to bacteremia and hemoptysis due to rupture of the aneurysm into the lung, which can even result in death. Rarely, manifestations of tracheal and superior vena caval compression can be presenting symptoms.1-4 Echocardiography is helpful to diagnose pseudoaneurysms and blood cultures can detect the possible organisms growing in it. Bacteria such as Pseudomonas and fungi such as Candida have been reported in the pseudoaneurysms.5 Cardiac catheterization and CT are necessary for accurate localization of the lesion and are essential for correct decisions regarding treatment.6
Previously, the immediate radical resection of all infected tissue and the graft was preferred to prevent catastrophic bleeding and sepsis. In addition, reconstruction of the systemic-pulmonary artery shunt or a single-stage definitive repair was performed according to the underlying cardiac conditions. However, both procedures pose a risk of recurrent infection of the prosthetic materials, which is responsible for a fatal outcome. For a chronically formed pseudoaneurysm, combination of antibiotic therapy with exclusion of infected pseudoaneurysm offers a better treatment outcome as compared to radical surgical excision alone.1,5,7,8
The pseudoaneurysm can be excluded both surgically and percutaneously. Surgical approach has the advantages of removal of all the infected tissue and prosthetic material as well as having an opportunity to rectify the underlying disease by replacing the shunt or complete repair, wherever feasible. However, percutaneous approach for exclusion of pseudoaneurysm can be preferred as a bridge to surgery in patients who are critically ill or in whom surgery is deferred due to other unavoidable reasons.
Endovascular grafts have been used for many indications, including aortopulmonary fistulas and aortic, iliac, and femoral aneurysms as well as lethal and mycotic pulmonary artery pseudoaneurysms.9-11 In our case, we planned to seclude the pseudoaneurysm from circulation to prevent bacteremia. Endovascular prosthesis was placed after treating the patient with appropriate antibiotics for a long duration and the antibiotics were continued after the procedure and after the palliative surgery as well. This is probably the first case highlighting an alternate use of covered stent in the treatment of infected pseudoaneurysm of modified BT shunt.
Conclusion
We describe a new application of covered stent wherein we used a 6 mm x 38 mm covered stent to exclude a pseudoaneurysm of the LSA. This simplified the management of a patient with chronically infected BT shunt.
References
- Matsuhisa H, Yoshimura N, Kitahara J, et al. An infected pseudoaneurysm following a modified Blalock-Taussig shunt. Interact CardioVasc Thorac Surg. 2009;8(1):108-110.
- Valliattu J, Jairaj P, Delamie T, Subramanyam R, Menon S, Vyas H. False aneurysm following modified Blalock-Taussig shunt. Thorax. 1994;49(4):383-384.
- Sethia B, Pollock JC. False aneurysm formation: a complication following the modified Blalock-Taussig shunt. Ann Thorac Surg. 1986;41(6):667-668.
- Caffarena JM, Llamas P, Otero-Coto E. False aneurysm of a palliative shunt producing massive hemoptysis. Chest. 1982;81(1):110-112.
- Carvalho JS, Belcher P, Knight WB. Infection of modified Blalock shunts. Br Heart J. 1987;58(3):287-290.
- Turner SW, Wyllie JP, Hamilton JR, Bain HH. Diagnosis of infected modified Blalock-Taussig shunt by computed tomography. Ann Thorac Surg. 1995;59(5):1216-1217.
- Parvathy U, Balakrishnan KR, Ranjith MS, Moorthy JS. False aneurysm following modified Blalock-Taussig shunt. Pediatr Cardiol. 2002;23(2):178-181.
- Ootaki Y, Yamaguchi M, Yoshimura N. Successful surgical management of infected modified Blalock-Taussig shunts. Cardiol Young. 2004;14(2):219-221.
- Chou MC, Liang HL, Pan HB, Yang CF. Percutaneous stent-graft repair of a mycotic pulmonary artery pseudoaneurysm. Cardiovasc Intervent Radiol. 2006;29(5):890-892.
- Hannan RL, Miyaji K, Burke RP, Zahn EM. Endovascular stent graft treatment of a pulmonary artery pseudoaneurysm. Ann Thorac Surg. 2001;71(2):727-729.
- Kannan BR, Jain AK, Qureshi SA, Rothman MT, Rosenthal E, Mathur A. Successful exclusion of large post-surgical pseudoaneurysm of the ascending aorta by a percutaneous approach. Ann Thorac Surg. 2009;87(4):1281-1284.
_____________________________________________
From the Department of Pediatric Cardiology, Apollo Health City, Jubilee Hills, Hyderabad, India.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 18, 2011, provisional acceptance given December 1, 2011, final version accepted January 16, 2012.
Address for correspondence: Dr. Anurakti Srivastava, Department of Pediatric Cardiology, Apollo Health City, Jubilee Hills, Hyderabad, India. Email: anurakti07@yahoo.co.in

