

Decrease in Coronary Flow After Consecutive Injections of Contrast Media During Coronary Angiography
Abstract: Background. TIMI frame count (TIMIfc) is widely used to assess coronary flow during angiography and there are studies showing the effects of contrast media on blood cells. In this study, we investigate changes in coronary flow and in red blood cells following contrast injections. Methods and Results. Coronary flow was assessed by TIMIfc in the left anterior descending and circumflex coronary arteries of patients undergoing elective angiography. Changes in the morphology of red blood cells and in the mean corpuscular volume (MCV) were evaluated by optical microscopy. We enrolled 24 patients with a mean age of 61.9 ± 12 years. In 45 coronary arteries, the mean baseline-corrected TIMIfc was 19.4 ± 3.46 frames and the final one was 24.3 ± 3.2 frames (P=.001) with a mean increase of 4.92 ± 0.25 frames (frame range, 0-10), indicating significant impairment of coronary flow. There was an increase in the number of crenated red cells per camp (4.3 ± 3.4%; P=.001). The MCV changed from 86.6 ± 4.7 fL to 86.8 ± 4.6 fL (P=.011). There was no association of the TIMIfc increase with changes in either crenated red cells (P=NS) or MCV (P=NS). Conclusion. There was significant impairment of coronary artery flow following contrast injections during angiography. These findings indicate that the TIMIfc is affected by the timing of assessment during angiography, with implications for clinical trial design and for the use of TIMIfc as a surrogate endpoint. In addition, this impairment of coronary flow may have implications for slow flow observed during coronary interventions.
J INVASIVE CARDIOL 2013;25(7):348-352
Key words: contrast media, coronary flow, red cells, coronary angiography
______________________________________
TIMI frame count (TIMIfc) score is widely used in medical practice and clinical trials, providing a quantitative, simple, and reproducible assessment of coronary blood flow during coronary angiography.1
There are several studies indicating that contrast media can affect blood red cells, white cells, endothelium, platelets, coagulation, and fibrinolysis system. These effects may be related to the chemical formula of contrast media, electric charge, viscosity, osmolality, and pH of a solution and may potentially impair blood flow.2
When in contact with contrast media, red cells change their discoid shape and shrink.3-5 These effects on morphology lead to a decrease in red cell plasticity, which may impact normal capillary flow.6,7 Contrast media also increase red cell aggregability, which may lead to capillary stasis.8-14 In an experimental study in dogs, a decrease in coronary flow after contrast medium injection was observed.15,16 In addition, contrast medium injections into the brachial artery of patients with coronary artery disease decreased capillary flow in the nail fold.17,18
Despite its widespread use, the impact of consecutive contrast medium injections on human coronary flow has not been established. We assessed changes in coronary flow after using contrast media in stable patients undergoing elective coronary angiography. We also observed changes in the morphology of red cells and in the MCV.
Methods
Stable patients between 18 and 75 years of age referred for elective coronary angiography were invited to join the study. The local Research Ethics Committee approved the study protocol and written informed consent was obtained for all patients.
Patients with separated ostium of the left anterior descending (LAD) and circumflex (CX) coronary arteries and with left main, LAD, or CX artery stenosis >30% were excluded from the study. Patients with a history of contrast medium allergies, valve or cardiac structural disease, myocardial infarction, coronary bypass surgery, renal or hepatic failure, or any terminal disease were also excluded.
Coronary angiography was performed in all patients by the same interventional cardiologist using standard techniques, with manual injection of contrast media through a 6 Fr left coronary Judkins diagnostic catheter. Contrast media were meglumine and sodium ioxitalamate (Telebrix 35; Guerbet). Coronary flow was assessed by the TIMIfc score in the baseline study with injection carried out immediately before the first diagnostic left coronary angiography; and in the final study, injection was carried out after completion of the fifth left coronary angiography.1 Intracoronary nitroglycerin (200 µg) was administrated before the baseline study angiography and before the final one if it was performed more than 15 minutes later. Study angiographies were performed in the right anterior oblique caudal view (20°/20°) to evaluate both the CX and LAD coronary arteries with a 9 inch (23 cm) lens and at an acquisition rate of 30 frames/second. TIMIfc was assessed offline by two interventional cardiologists blinded to the injection order. In case of disagreement, a consensus counting was performed. Changes in coronary artery flow were defined as the TIMIfc difference between the final and baseline injections (delta TIMIfc = final TIMIfc – baseline TIMIfc). Offline quantitative coronary angiography (Siemens, AcomPC 5.02) was performed to assess changes in coronary artery luminal diameter between the same study injections used to assess coronary flow.
Blood samples were drawn from the aortic root through the left coronary catheter at baseline and after all left coronary angiograms had been carried out. The blood samples were evaluated by optic microscopy (Sysmex SE 9500 ou Sysmex XT 2000i TOA Medical Electronics). Morphological changes of red cells were assessed by the percentage of crenated red cells per camp observed in glass slides stained with May-Grünwald-Giemsa, as delta %crenated red cells = final %crenated red cells – baseline %crenated red cells. Changes in the MCV were assessed as delta MCV = final MCV – baseline MCV. All assessments were performed by a hematologist blinded to the TIMIfc results and to the sample order.
Statistical analysis. Demographic and procedure variables are presented as percentage and mean ± standard deviation. Continuous variables were compared using Student’s t-test for paired samples. A bicaudal P-value <.05 was accepted as statistically significant. Correlations between TIMIfc and the percentage of crenated red cells and between TIMIfc and luminal diameter changes were assessed by Spearmann’s correlation test. TIMIfc changes in the circumflex and left descending coronary arteries were assessed by generalized estimating equations – Wald test.
equations – Wald test.
According to previous findings, sample size calculations indicated that 17 coronary TIMIfc assessments would be needed to demonstrate a change in the TIMIfc of 4 frames, assuming that the standard deviation was 3.9 frames with 90% power and P of 5% significance.1
Results
We enrolled 24 patients. A total 45 arteries comprised of 24 CX and 21 LAD coronary arteries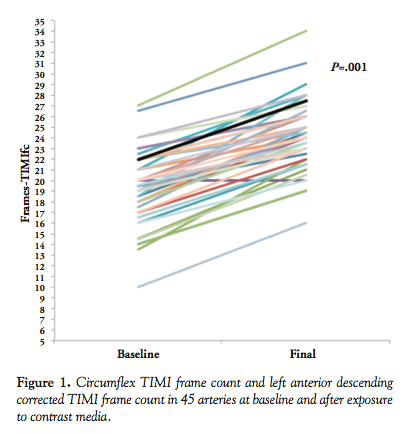 were examined. Three LADs were excluded because of >30% stenosis. Baseline characteristics are shown in Table 1. The mean age was 61.9 ± 12 years, 13 patients (54.2%) were male, 21% had diabetes, 71% had hypertension, and 50% took statins. The mean contrast medium volume used during the angiogram was 68.2 ± 19 mL. The mean time between the two study injections was 5.8 ± 0.7 minutes. The mean baseline cardiac frequency was 75.9 ± 10.4 beats/minutes and the final frequency was 76.25 ± 10.2 beats/minute (P=.44). None of the patients experienced any adverse reactions or complications.
were examined. Three LADs were excluded because of >30% stenosis. Baseline characteristics are shown in Table 1. The mean age was 61.9 ± 12 years, 13 patients (54.2%) were male, 21% had diabetes, 71% had hypertension, and 50% took statins. The mean contrast medium volume used during the angiogram was 68.2 ± 19 mL. The mean time between the two study injections was 5.8 ± 0.7 minutes. The mean baseline cardiac frequency was 75.9 ± 10.4 beats/minutes and the final frequency was 76.25 ± 10.2 beats/minute (P=.44). None of the patients experienced any adverse reactions or complications.
The mean baseline TIMIfc was 19.4 ± 3.46 and the final one was 24.3 ± 3.20 frames (P=.001). Coronary flow was significantly impaired between the baseline and the final contrast injections, with a mean TIMIfc increase of 4.9 ± 0.25 frames in the frame range 0-10 (Figure 1 and Table 2). None of the patients showed a TIMIfc reduction from the baseline up to the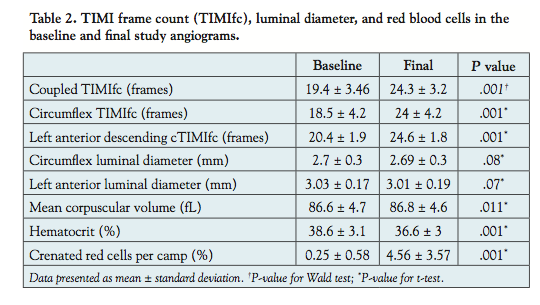 final contrast injection.
final contrast injection.
Contrast media administration was also associated with changes in the morphology of red cells and MCV (Table 2). The MCV changed from 86.6 ± 4.7 fL to 86.8 ± 4.6 fL (delta = 0.25 ± 0.4 fL; P=.011). The percentage of crenated red cells per camp rose from 0.25 ± 0.6% to 4.5 ± 3.6% (P=.001). However, there was no correlation between changes in the CX TIMIfc or in the LAD corrected TIMIfc and the percentage of crenated red cells (r2 = -0.174 and P=.41; r2 = 0.268 and P=.24, respectively) (Figures 2 and 3). No significant CX TIMIfc or LAD corrected TIMIfc variation was observed (5.5 ± 1.9 frames vs 5.6 ± 3.4 frames with P=.92; 4 ± 1.5 frames vs 4.6 ± 1.5 frames with P=.44, respectively) after comparing patients with no MCV changes to those with a one-unit increase in MCV.
Quantitative coronary angiography showed a minor non-significant reduction in coronary luminal diameter. The baseline luminal diameter of the proximal CX coronary artery was 2.70 ± 0.30 mm and the final luminal diameter was 2.69 ± 0.34 mm (P=.08). The LAD coronary artery showed a baseline luminal diameter of 3.03 ± 0.17 mm and the final luminal diameter of 3.01 ± 0.19 mm (P=.07). There was no correlation between the changes in the CX TIMIfc or LAD corrected TIMIfc and in the minimal luminal diameter (r2 = -0.128 and P=.55; r2 = -0.222 and P=.33, respectively) (Figures 4 and 5).
Discussion
To our knowledge, this is the first study that has specifically evaluated changes in coronary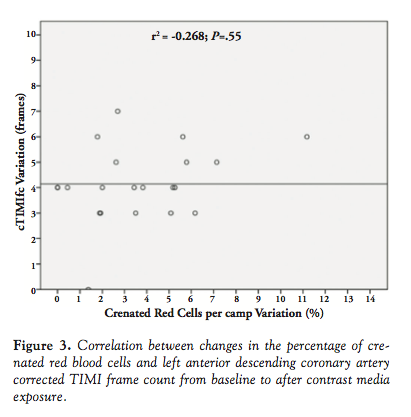 artery blood flow during coronary angiography in stable patients with no significant coronary artery stenosis and not undergoing percutaneous coronary intervention. We found that coronary artery flow decreases after successive contrast medium injections. This finding was not related to contrast-induced changes in the morphology of red blood cells or MCV.
artery blood flow during coronary angiography in stable patients with no significant coronary artery stenosis and not undergoing percutaneous coronary intervention. We found that coronary artery flow decreases after successive contrast medium injections. This finding was not related to contrast-induced changes in the morphology of red blood cells or MCV.
Effects of contrast media on blood cells and endothelium. Several investigators using a myriad of contrast agents demonstrated the effects of contrast media on blood rheology, erythrocytes, and platelet aggregation.19-22 In an in vitro study, iopromide, ioxaglate, and gadolinium-DOTA increased blood viscosity at a high shear rate in a dose-dependent manner. In addition, they decreased the mean erythrocyte volume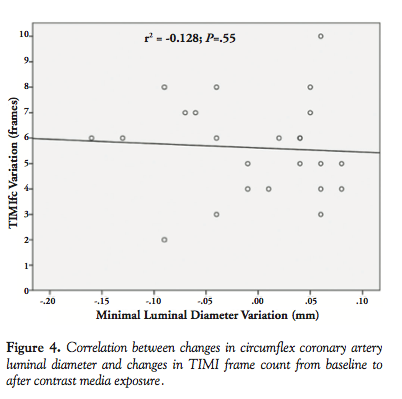 and platelet aggregation. Iopromide induced echinocytic shape transformation of erythrocytes. Iopromide and ioxaglate caused an ex vivo decrease in hematocrit and, therefore, decreased the whole blood viscosity.23
and platelet aggregation. Iopromide induced echinocytic shape transformation of erythrocytes. Iopromide and ioxaglate caused an ex vivo decrease in hematocrit and, therefore, decreased the whole blood viscosity.23
It has been reported that changes in the morphology of blood cells associated with exposure to contrast media can embolize the microvasculature, impairing blood flow.24-26 In 60 patients undergoing coronary angiography, 4 different contrast media caused a significant decrease in hematocrit, erythrocyte aggregation, platelet reactivity index, and plasma viscosity.27
Factors that alter viscosity may have important consequences during angiography. Effects on the viscosity of erythrocyte-plasma suspensions of different concentrations of 5 kinds of contrast media were tested and the changes in viscosity differed markedly among the various
types of contrast media. The conventional high-osmolar ionic monomers caused most disturbances to blood viscosity. The ionic dimer ioxaglate was least disturbing to the viscometric characteristics of blood, and the non-ionic monomers were intermediate in their effects.14
disturbances to blood viscosity. The ionic dimer ioxaglate was least disturbing to the viscometric characteristics of blood, and the non-ionic monomers were intermediate in their effects.14
Contrast media can also affect endothelial cells. Iomeprol and iodixanol determined morphologic changes in human umbilical vein endothelial cells with an increase in cell circumference length, the number of dissolved cell contacts, and the number of denuded subendothelial matrix areas.28 In another study, iohexol and iodixanol did not affect endothelial cell height after short-term incubation, whereas after incubation in iopromide and iomeprol there was strong buckling and increased endothelial height.29
It is not well established how long these changes last. The reversibility of echinocytes found in red cells after contrast media contact apparently is kind- and concentration-dependent. A study with iodixanol, iohexol, iomeprol, and iopromide showed a reversal of changes in red cells after resuspension in autologous plasma for 5 minutes.30
We observed an increase in MCV and in the percentage of crenated red cells showing the effect of contrast media as reported in previous studies in spite of the small clinical magnitude and the fact that it was not correlated with TIMIfc changes.22 The use of contrast media has been associated with coronary vasoconstriction and changes in coronary diameter after contrast medium injection could mislead the TIMIfc evaluation.31In this study, intracoronary nitroglycerin was given before the baseline angiogram. The non-significant change in luminal diameter during contrast medium administration was not correlated with TIMIfc changes.
Effect of contrast media on coronary flow. The side effects of contrast media on blood cells and rheology could potentially impair coronary flow. The effect of intracoronary injection of contrast medium on flow has already been studied in a dog model and the observed decrease in coronary flow was closely related to the contrast medium dose and infusion rate.15 The intracoronary injection of contrast media in dogs caused a 45% decrease of flow observed at 1.9 seconds.32Angiographic measures taken in the first seconds after injection should take into account these characteristics.
In humans, the influence of direct intraarterial administration of contrast media on capillary perfusion was evaluated with iso-osmolar, non-ionic iodixanol and low-osmolar, non-ionic iopentol. Right-hand nail fold perfusion was monitored before and after 20 mL of contrast medium was injected into the right axilar artery. There was a 60.8% decrease in red cell velocity with iodixanol that was observed 10 seconds after infusion and lasted until the end of the 6-minute observation period. The changes in arterial blood flow were not significant with the same volume and at the same iopentol infusion rate.33,34
In the TIMI 14 trial, clinical and angiographic outcomes in diagnostic and interventional procedures were studied after use of the contrast media at 90 minutes after thrombolytic administration. There was no relationship between contrast agent type and overall patency, rate of TIMI grade 3 flow, or corrected TIMIfc when ionic and non-ionic contrast media were compared. While there was no difference in epicardial blood flow, ionic contrast agent use was associated with poorer ST-segment resolution, longer chest pain duration, and lower ejection fractions, perhaps as a result of microvascular dysfunction.35
Previous studies did not take into account the impact of several consecutive contrast medium injections on coronary flow evaluation. Gibson et al reported in two consecutive hand coronary injections with 1-2 minute intervals a mean absolute difference of 4.7 ± 3.9 frames in the acute myocardial infarction culprit artery after thrombolysis.1 Thrombotic burden and microvasculature status might have had an important contribution in that setting and it was uncertain how those findings would translate in stable patients.
TIMIfc variability. In previous studies, it was observed that catheter size, gender, contrast infusion rate, and image acquisition rate did not influence TIMIfc.31 Conversely, intraobserver variability, degree of selective catheterization, heart rate variability, phase of cardiac cycle injected, and intracoronary nitrate use have been reported to impact TIMIfc. A 20 beat/minute increase in heart rate was associated with a 5-frame decrease in TIMIfc.36 The contrast injection during diastole reduces 3 frames in right coronary artery and 6 frames in left coronary artery when compared to systole injections. Intracoronary nitrate infusion caused a 4-frame increase in TIMIfc when compared to basal status.36 TIMIfc standard deviation for normal coronary arteries under optimal study conditions remained at ±3.1 frames.37
Study limitations. This study has limitations that deserve consideration. We assessed the effect of successive contrast medium injections on a small sample of stable patients. It is uncertain whether these findings apply to different clinical settings. Although all contrast media are associated with some degree of untoward effects, it is unknown whether our findings can be replicated with other contrast agents.38 Finally, we did not study how long the observed changes in coronary flow lasted.
Conclusion
The main finding of this study was a decrease in coronary flow associated with successive contrast medium injections. The contrast medium administration increased the percentage of crenated red cells per camp and MCV, but these changes were not correlated with TIMIfc changes.
This study brings an important contribution considering the importance of coronary flow evaluation in the clinical setting and the use of TIMIfc score in clinical trials. These findings indicate that TIMIfc is affected by the timing of an assessment during coronary angiography with implications for clinical trial design and for the use of TIMIfc as a surrogate endpoint. In addition, contrast-media associated impairment of coronary flow may have implications for slow-flow mechanisms during coronary interventions. The findings presented herein deserve further study.
References
- Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation.1996;93(5):879-888.
- Hardeman MR, Goedhart P, Koen IY. The effect of low-osmolar ionic and nonionic contrast media on human blood viscosity, erythrocyte morphology, and aggregation behavior. Invest Radiol.1991;26(9):810-819.
- Aspelin P, Schmid-Schonbein H. Effect of ionic and non-ionic contrast media on red cell aggregation in vitro. Acta Radiol Diagn (Stockh).1978;19(5):766-784.
- Aspelin P, Birk A, Almen T, et al. Effect of iohexol on human erythrocytes. II. Red cell aggregation in vitro. Acta Radiol Suppl.1980;362:123-126.
- Aspelin P, Stohr-Liessen M, Almen T. Effect of iohexol on human erythrocytes. I. Changes of red cell morphology in vitro. Acta Radiol Suppl. 1980;362:117-122.
- Grabowski EF. Effects of contrast media on erythrocyte and platelet interactions with endothelial cell monolayers exposed to flowing blood. Invest Radiol. 1988;2(Suppl 2): S351-S358.
- Miyazawa T, Murayama C, Yamanaka T, et al. Cerebral embolization in rats induced by red blood cells treated with hypertonic X-ray contrast medium. Invest Radiol. 1993;28(9):831-837.
- Higashi S, Yasukochi H, Ishioka K, et al. [The effects of angiographic contrast media on the aggregation and morphology of red cells in vitro]. Nippon Igaku Hoshasen Gakkai Zasshi. 1989;49(6):748-757.
- Aspelin P, Schmid-Schonbein H. Effect of ionic and non-ionic contrast media on blood rheology. Bibl Anat.1977;(16 Pt 2):517-521.
- Aspelin P, Nilsson PE, Schmid-Schonbein H, et al. Effect of four non-ionic contrast media on red blood cells in vitro. I. Morphology. Acta Radiol Suppl.1987;370:79-83.
- Aspelin P, Nilsson PE, Schmid-Schonbein H, et al. Effect of four non-ionic contrast media on red blood cells in vitro. II. Aggregation. Acta Radiol Suppl.1987;370:85-97.
- Aspelin P, Nilsson PE, Schmid-Schonbein H, et al. Effect of four non-ionic contrast media on red blood cells in vitro. III. Deformability. Acta Radiol Suppl.1987;370:89-91.
- Aspelin P. Effect of ionic and non-ionic contrast media on red cell deformability in vitro. Acta Radiol Diagn (Stockh).1979;20(1):1-12.
- Strickland NH, Rampling MW, Dawson P, et al. Contrast media-induced effects on blood rheology and their importance in angiography. Clin Radiol.1992;45(4):240-242.
- Friedman HZ, DeBoe SF, McGillem MJ, et al. The immediate effects of iohexol on coronary blood flow and myocardial function in vivo. Circulation.1986;74(6):1416-1423.
- Friedman HZ, DeBoe SF, McGillem MJ, et al. Immediate effects of graded ionic and nonionic contrast injections on coronary blood flow and myocardial function. Implications for digital coronary angiography. Invest Radiol. 1987;22(9):722-727.
- Bach R, Jung F, Scheller B, et al. Influence of a non-ionic radiography contrast medium on the microcirculation. Acta Radiol.1996;37(2):214-217.
- Bach R, Gerk U, Mrowietz C, et al. Influence of a new monomeric nonionic radiographic contrast medium (iobitridol-350 versus NaCl) on cutaneous microcirculation: single-center, prospective, randomized, double-blind phase IV study in parallel group design. Microvasc Res.2000;60(3):193-200.
- Aspelin P, Stacul F, Thomsen HS, et al. Effects of iodinated contrast media on blood and endothelium. Eur Radiol.2006;16(5):1041-1049.
- Galtung HK, Sørlundsengen V, Sakariassen KS, et al. Effect of radiologic contrast media on cell volume regulatory mechanisms in human red blood cells. Acad Radiol. 2002;9(8):878-885.
- Bucherer C, Lacombe C, Lelievre JC. Effects of two low-osmolar contrast media, ioxaglate and iopamidol, on erythrocyte membrane elasticity. Invest Radiol. 1994;29(12):1026-1030.
- Aspelin P. Effect of ionic and non-ionic contrast media on whole blood viscosity, plasma viscosity and hematocrit in vitro. Acta Radiol Diagn (Stockh). 1978;19(6):977-989.
- Reinhart WH, Pleisch B, Harris LG, et al. Influence of contrast media (iopromide, ioxaglate, gadolinium-DOTA) on blood viscosity, erythrocyte morphology and platelet function. Clin Hemorheol Microcirc.2005;32(3):227-239.
- Schmid-Schonbein GW. Capillary plugging by granulocytes and the no-reflow phenomenon in the microcirculation. Fed Proc.1987;46(7):2397-2401.
- Liu S, Connor J, Peterson S, et al. Direct visualization of trapped erythrocytes in rat brain after focal ischemia and reperfusion. J Cereb Blood Flow Metab. 2002;22(10):1222-1230.
- Nygren A, Hellberg O, Hansell P. Red-cell trapping in the rat renal microcirculation induced by low-osmolar contrast media and mannitol. Invest Radiol. 1993;28(11):1033-1038.
- Scheller B, Hennen B, Thunenkotter T, et al. Effect of X-ray contrast media on blood flow properties after coronary angiography. Thromb Res. 1999;96(4):253-260.
- Franke RP, Fuhrmann R, Park JW, et al. The effect of radiographic contrast media on the morphology of human venous endothelial cells. Clin Hemorheol Microcirc. 2007;37(4):329-338.
- Franke RP, Fuhrmann R, Hiebl B, et al. Influence of various radiographic contrast media on the buckling of endothelial cells. Microvasc Res.2008;76(2):110-113.
- Mrowietz C, Hiebl B, Franke RP, et al. Reversibility of echinocyte formation after contact of erythrocytes with various radiographic contrast media. Clin Hemorheol Microcirc.2008;39(1-4):281-286.
- Vijayalakshmi K, Ashton VJ, Wright RA, et al. Corrected TIMI frame count: applicability in modern digital catheter laboratories when different frame acquisition rates are used. Catheter Cardiovasc Interv.2004;63(4):426-432.
- Hodgson JM, Mancini GB, Legrand V, et al. Characterization of changes in coronary blood flow during the first six seconds after intracoronary contrast injection. Invest Radiol.1985;20(3):246-252.
- Jung F, Spitzer S, Mrowietz C, et al. Influence of radiographic contrast media (Iomeprol 350 versus Iopentol 350) on cutaneous microcirculation: single-center prospective randomized double-blind phase IV study in parallel-group design. J Invasive Cardiol. 1999;11(1):2-8.
- Spitzer S, Munster W, Sternitzky R, Bach R, Jung F. Influence of Iodixanol-270 and Iopentol-150 on the microcirculation in man: influence of viscosity on capillary perfusion. Clin Hemorheol Microcirc.1999;20(1):49-55.
- Gibson CM, Kirtane AJ, Murphy SA, et al; the TIMI Study Group. Impact of contrast agent type (ionic versus nonionic) used for coronary angiography on angiographic, electrocardiographic, and clinical outcomes following thrombolytic administration in acute myocardial infarction. Catheter Cardiovasc Interv.2001;53(1):6-11.
- Abaci A, Oguzhan A, Eryol NK, et al. Effect of potential confounding factors on the thrombolysis in myocardial infarction (TIMI) trial frame count and its reproducibility. Circulation.1999;100(22):2219-2223.
- Kunadian V, Harrigan C, Zorkun C, et al. Use of the TIMI frame count in the assessment of coronary artery blood flow and microvascular function over the past 15 years. J Thromb Thrombolysis.2009;27(3):316-328.
- Kelly RV, Gillespie MJ, Cohen MG, et al. The contrast media iohexol causes vasoconstriction of the proximal left anterior descending coronary artery: implications for appropriate stent sizing. Angiology.2008;59(5):574-580.
________________________________
From the 1Department of Cardiology, Hospital de Clínicas de Porto Alegre, Porto Alegre, Rio Grande do Sul, Brazil, 2Department of Cardiology, Hospital Bruno Born, Lajeado, Rio Grande do Sul, Brazil, and 3Department of Interventional Cardiology, Hospital São Lucas, Porto Alegre, Rio Grande do Sul, Brazil.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted February 4, 2013, provisional acceptance given March 4, 2013, final version accepted April 3, 2013.
Address for correspondence: Dr Ana Maria Krepsky, Dario Pederneiras 328/501, Porto Alegre, Rio Grande do Sul, Brazil 90630-090. Email: anamariakrepsky@gmail.com



