

A Case of Contrast-Induced Pancreatitis Following Cardiac Catheterization
ABSTRACT: Coronary heart disease remains the leading cause of death of men and women in the United States. Angiography and percutaneous coronary interventions (PCI) are an integral part in management of acute coronary syndromes. Well-defined complications of coronary angiography include allergic and anaphylactic reactions, vascular access complications, stroke, and contrast-induced kidney injury. Radiographic contrast agents (RCAs) are known to cause acute kidney injury. RCAs are also postulated to induce pancreatitis in experimental animal models. We present a patient with acute pancreatitis immediately following coronary angiography. Recent studies have described that the use of RCA is associated with worse prognosis in patients with ongoing pancreatitis. The pathophysiology of RCA-induced pancreatitis is poorly understood. Although extremely rare, RCA-induced pancreatitis should be considered in the appropriate clinical setting.
J INVASIVE CARDIOL 2013;25(10):E203-E204
Key words: radiographic contrast agent, PCI complications
_____________________________
The number of coronary angiography and percutaneous coronary intervention (PCI) procedures performed has increased significantly in recent years. Well-defined complications of coronary angiography include allergic and anaphylactic reactions, vascular access complications, stroke, and contrast-induced kidney injury. Radiographic contrast agents (RCAs) are known to cause acute kidney injury. RCAs are also postulated to induce pancreatitis in experimental animal models. The first reported case of fulminant pancreatitis attributed to a RCA was published in 1981 following ventriculography.1 We present a patient with acute pancreatitis immediately following coronary angiography.
Case Report. A 67-year-old female with hypertension presented as an outpatient for coronary angiography because of an abnormal stress test. Preprocedural evaluation demonstrated a diagnosis of diabetes mellitus with a hemoglobin-A1C level of 6.2%. This was still untreated at the time of angiography. She had only been on hydrochlorothiazide, taken for many years for hypertension, and it was held the day of the procedure. Percutaneous access was obtained through the right common femoral artery with a 6 Fr sheath. Angiography and ventriculography were performed with a total of 120 cc of iopamidol nonionic-hypertonic contrast. The patient was sedated with fentanyl and midazolam. Her cardiac catheterization demonstrated 3-vessel disease and was initially uncomplicated. The patient was discharged home on the same day with outpatient follow-up to discuss treatment options. Approximately 1 hour post discharge, she returned to the emergency department with complaints of sudden-onset epigastric pain, nausea, and vomiting. She denied any recent history of abdominal trauma, alcohol intake, smoking, or ingestion of any medications known to cause pancreatitis over the past 24 hours.
Upon presentation, the patient was afebrile, blood pressure was 135/90 mm Hg, and pulse of 128 beats/minute. Her physical exam was significant for moderate epigastric and left-upper quadrant tenderness. She was neurologically intact and no skin lesions were noted. Laboratory work-up is summarized in Table 1. Liver transaminases were mildly elevated. Triglyceride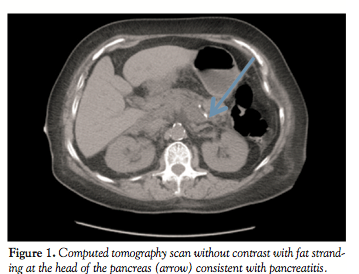 level was within the normal range at 62 mg/dL. Her creatinine was normal and remained unchanged during her hospitalization. An abdominal computed-tomography scan without contrast was consistent with acute pancreatitis (Figure 1) with no evidence of gallstones. The patient was managed with empiric antibiotics, intravenous fluids, nutritional support and mechanical ventilator support for the subsequent development of acute respiratory distress syndrome. The patient’s condition improved after the initial 48 hours. As part of the in-hospital work-up, common causes of acute pancreatitis, such as medication, alcohol, hypertriglyceridemia, and gallstones were dismissed. Other uncommon causes of pancreatitis, such as autoimmune pancreatitis, were ruled out by identifying a negative ANA and normal IgG1-4 titers. At discharge a few days later, she was asymptomatic and amylase and lipase levels were 65 U/L and 56 U/L, respectively.
level was within the normal range at 62 mg/dL. Her creatinine was normal and remained unchanged during her hospitalization. An abdominal computed-tomography scan without contrast was consistent with acute pancreatitis (Figure 1) with no evidence of gallstones. The patient was managed with empiric antibiotics, intravenous fluids, nutritional support and mechanical ventilator support for the subsequent development of acute respiratory distress syndrome. The patient’s condition improved after the initial 48 hours. As part of the in-hospital work-up, common causes of acute pancreatitis, such as medication, alcohol, hypertriglyceridemia, and gallstones were dismissed. Other uncommon causes of pancreatitis, such as autoimmune pancreatitis, were ruled out by identifying a negative ANA and normal IgG1-4 titers. At discharge a few days later, she was asymptomatic and amylase and lipase levels were 65 U/L and 56 U/L, respectively.
Discussion. Acute pancreatitis is commonly caused by alcohol intake and gallstones. Other etiologies are rare and include drugs, infectious causes, vascular complications, and autoimmune-related causes. The etiology remains unclear in up to 15%-25% of cases.
Medication-induced pancreatitis has an incidence rate of 0.3%-1.4%. Our patient had been taking hydrochlorothiazide (known to possibly cause pancreatitis); however, she had been on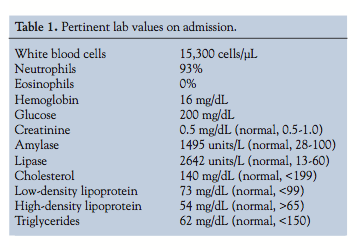 it for many years without complication, and it was held 24 hours prior to her procedure. The proposed mechanisms of hydrochlorothiazide-induced pancreatitis include secondary hypercalcemia and hypophosphotemia, hypertriglyceridemia, and hypotension,2 all effectively ruled out on admission. She has since been restarted on hydrochlorothiazide without issue.
it for many years without complication, and it was held 24 hours prior to her procedure. The proposed mechanisms of hydrochlorothiazide-induced pancreatitis include secondary hypercalcemia and hypophosphotemia, hypertriglyceridemia, and hypotension,2 all effectively ruled out on admission. She has since been restarted on hydrochlorothiazide without issue.
RCAs have been reported to induce pancreatitis in experimental animal studies. Recent studies have described that the use of RCA is associated with worse prognosis in patients with ongoing pancreatitis. A small study showed a correlation between pancreatitis and RCAs in hemodialysis patients.3
Pancreatitis after coronary catheterization is a complication that has only been described in a rare patient.4 Our hypothesis is that the pathogenesis of contrast-induced pancreatitis may be related to decreased oxygenation and impaired circulation of the pancreas.5 The RCA used in our patient (iopamidol) has a viscosity of 9.4 cP at 37 degrees centigrade versus human plasma of 1.72 cP at Hct of 43%. A similar pathophysiologic process has been proposed in contrast-induced kidney injury.
Another possibility is cholesterol crystal embolization (CCE). Flory first described CCE in 1945 with dislodgment of cholesterol crystals resulting in occlusion of small arteries.6 CCE usually demonstrates systemic involvement. Retinal emboli, blue toe syndrome, transient eosinophilia, renal failure, and hypertension have all been described in CCE. Our patient only had clinical and diagnostic findings of acute pancreatitis, making CCE highly unlikely. She neither developed renal failure acutely nor throughout her hospitalization. Our patient did not have signs of significant aortic atherosclerotic disease on physical examination or imaging. A case series (Orvar et al)7 of pancreatitis due to embolization showed necrotizing pancreatitis on autopsy in all patients in the series. Our patient did not have radiological or clinical evidence of necrosis. However, although CCE is a clinical diagnosis, biopsy is the gold standard to establish the diagnosis and was not performed on our patient.
Conclusion. Acute pancreatitis is an extremely rare complication of cardiac catheterization. We suggest that contrast-induced pancreatitis should remain in the differential diagnosis of patients presenting with pancreatitis following catheter-based procedures.
Acknowledgment. The authors wish to thank Marc Zughaib for his significant contributions to this case report.
References
- Chin WS, Ng R. Acute fulminant pancreatitis following ventriculography. Cardiovasc Intervent Radiol. 1981;4(2):108-109.
- Tisdale JE, Miller DA, eds. Drug-induced diseases: prevention, detection, and managements. Bethesda, Maryland: American Society of Health-System Pharmacists: 2010.
- Kheda M, Brenner L, Riggans D, Kota V, Szerlip HM. Pancreatitis following administration of iodixanol in patients on hemodialysis: a pilot study. Clin Nephrol. 2010;73(5):381-384.
- Wang LX, Fu WG, Guo DQ, et al. [Analysis of contrast medium induced pancreatitis]. Zhonghua Yi Xue Za Zhi. 2010;90(17):1159-1161.
- Plock JA, Schmidt J, Anderson SE, Sarr MG, Roggo A. Contrast-enhanced computed tomography in acute pancreatitis: does contrast medium worsen its course due to impaired microcirculation? Langenbecks Arch Surg. 2005;390(2):156-163.
- Flory CM. Arterial occlusions produced by emboli from eroded atheromatous plaques. Am J Pathol. 1945;21:549-565.
- Orvar K, Johlin FC. Atheromatous embolization resulting in acute pancreatitis after cardiac catheterization and angiographic studies. Arch Intern Med. 1994;154(15):1755-1761.
From St John Providence Health System, Providence Hospital Heart Institute, Southfield, Michigan.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 2, 2013, provisional acceptance given April 12, 2013, final version accepted June 4, 2013.
Address for correspondence: Wael Ghalayini, MD, Providence Hospital, GME, 16001 W Mile 9 Road, Southfield, MI 48075. Email: ghalayinimd@gmail.com



