

Carotid Artery Stenting in a Community Hospital: A Success Story
Download a PDF of this article.
Abstract: Background. Carotid endarterectomy (CEA) is an effective procedure for reducing the risk of stroke in patients with carotid artery atherosclerosis. The evolution of carotid artery stenting (CAS) has made this a viable alternative to CEA in appropriate patient populations. We sought to evaluate the safety and efficacy of CAS in a high-risk population, in an effort to report such results in a medium-size community hospital. The data were then compared with the results published in the CREST and SAPPHIRE trials. Methods. The records of 280 consecutive patients undergoing carotid artery stenting between January 2005 and December 2011 were reviewed. A total of 271 patients were included in the final analysis. The clinical endpoints included cerebrovascular accident, myocardial infarction, and death in the perioperative period. Results. A total of 155 men (57.2%) and 116 women (42.8 %) underwent CAS. A total of 259 carotid interventions (95.6%) were successful. Two of 271 patients (0.7%) experienced a minor neurologic event post procedure, with 1 patient death (0.35%) recorded. No perioperative myocardial infarctions were encountered. Conclusion. Our findings indicate that our institution has been able to safely and effectively introduce and carry out CAS as a substitute to CEA in patients that are at high risk for surgery with results comparable to those published in large-scale clinical trials. Further studies are needed to verify whether these results can be generalized to other community hospitals, as well as to refine qualification criteria for performing physicians. Furthermore, the applicability of these results to normal-risk patients is currently being investigated.
J INVASIVE CARDIOL 2013;25(1):3–6
Key words: carotid atherosclerosis, carotid artery stenting
____________________________________________
Stroke is by far the most common neurological diagnosis that requires hospitalization,1 accounting for greater than half a million hospitalizations every year.2 In 2009, the estimated economic burden for the care of cerebrovascular disease patients was roughly $22.8 billion.3 Despite the large number of unreported cases, a stroke occurs every 40 seconds in the United States (US),4 with 1 death due to stroke every 4 minutes.5 Stroke is the fourth leading cause of mortality in the US, behind only heart disease, cancer, and respiratory disease,6 and is a major cause of serious long-term disability, leaving 15%-30% of its victims permanently disabled.7 Ischemic strokes are the most common type, accounting for 87% of all strokes. Of the remainder, 10% are due to intracerebral hemorrhage and 3% are secondary to subarachnoid hemorrhage.8 Carotid atherosclerosis is a significant cause of cerebrovascular disease, accounting for 7% of patients presenting with an initial stroke.9 The prevalence of more than 50% carotid stenosis was 9% among men and 7% in women between 66 and 93 years of age in the Framingham Heart Study population.10 Flow turbulence and shear stress reach their maximum at the bifurcation of the common carotid artery. Therefore, this is the most common location for plaque formation. Cerebral vascular accidents can develop with carotid atherosclerosis secondary to a reduction in vessel diameter induced by plaque burden. Furthermore, a thrombus can be superimposed on the atheroma, thereby increasing the degree of stenosis. Thus, an embolic phenomenon or low-flow state are the usual mechanisms of stroke. Carotid endarterectomy (CEA) has been established as an effective and reasonably safe procedure by multiple randomized trials for reducing the risk of stroke in symptomatic11-13 and asymptomatic14-16 patients with carotid artery atherosclerosis. However, the evolution of carotid artery stenting (CAS) and optimal medical therapy have made these viable alternatives to CEA in appropriate patient populations. Evidence in support of CAS versus CEA has come in the form of randomized controlled trials, such as the Study of Angioplasty with Protection in Patients at High Risk for Endarterectomy (SAPPHIRE) trial17 and the Carotid Revascularization Endarterectomy vs Stenting Trial (CREST).18 We sought to examine our carotid artery angioplasty and stenting data and evaluate the outcomes of patients undergoing this procedure in a medium-size, tertiary care, teaching community hospital. Our data were then compared with the results published in the CREST and SAPPHIRE trials.
Methods
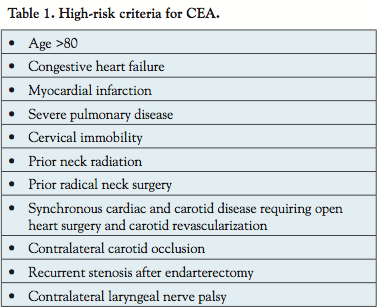 Patient population. The records of 280 consecutive patients undergoing CAS at Providence Hospital and Medical Center in Southfield, Michigan between January 2005 and December 2011 were reviewed. All patients were referred by either their primary care physician, cardiologist, or neurologist, and based on the evaluation, including detailed history, physical exam, carotid duplex ultrasound, computed tomography (CT) angiogram, and/or carotid angiogram, the decision was either to refer the patient to a vascular surgeon for evaluation and possible CEA or to perform carotid artery angioplasty and stenting if one or more high-risk variables were present, as outlined in Table 1.
Patient population. The records of 280 consecutive patients undergoing CAS at Providence Hospital and Medical Center in Southfield, Michigan between January 2005 and December 2011 were reviewed. All patients were referred by either their primary care physician, cardiologist, or neurologist, and based on the evaluation, including detailed history, physical exam, carotid duplex ultrasound, computed tomography (CT) angiogram, and/or carotid angiogram, the decision was either to refer the patient to a vascular surgeon for evaluation and possible CEA or to perform carotid artery angioplasty and stenting if one or more high-risk variables were present, as outlined in Table 1.
Bilateral CAS was performed on 28 patients in a staged fashion; however, we included only the data from the initial procedure to ensure a homogenous patient population. The procedure was not completed in 9 patients due to technical difficulties involving anatomical challenges and lesion characteristics. Subsequently, 3 of these 9 patients underwent CEA. A total of 271 patients were included in the final analysis.
Patients were considered symptomatic if they were the victims of transischemic attack (TIA) or stroke involving the ipsilateral carotid artery distribution within the previous 6 months. CAS was recommended for symptomatic patients with more than 50% stenosis, and for asymptomatic patients with more than 80% stenosis, as commonly defined by most carotid registries.
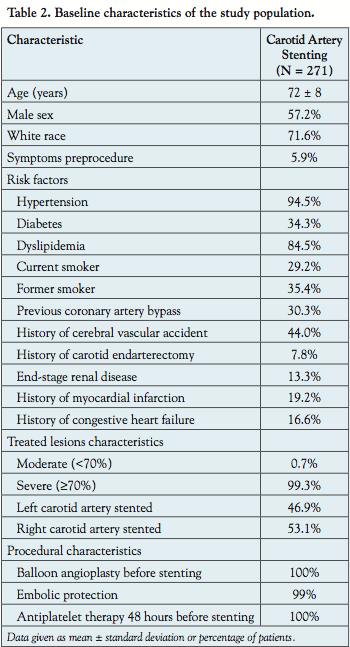 The mean age of the patients was 72 ± 8 years. A total of 155 men (57.2%) and 116 women (42.8%) underwent CAS. Patients’ baseline characteristics, medical history, and comorbidities are listed in Table 2. Sixteen patients (5.9%) had neurologic symptoms and a National Institutes of Health Stroke Scale (NIHSS)19 of >1 prior to the procedure. CAS was performed on 21 patients (7.8%) with prior CEA. The following comorbidities — prior myocardial infarction (52 patients, 19.2%) and congestive heart failure (45 patients, 16.6%) — classified patients as high-risk candidates for CEA, thereby allocating them to the CAS group.
The mean age of the patients was 72 ± 8 years. A total of 155 men (57.2%) and 116 women (42.8%) underwent CAS. Patients’ baseline characteristics, medical history, and comorbidities are listed in Table 2. Sixteen patients (5.9%) had neurologic symptoms and a National Institutes of Health Stroke Scale (NIHSS)19 of >1 prior to the procedure. CAS was performed on 21 patients (7.8%) with prior CEA. The following comorbidities — prior myocardial infarction (52 patients, 19.2%) and congestive heart failure (45 patients, 16.6%) — classified patients as high-risk candidates for CEA, thereby allocating them to the CAS group.
Baseline color duplex ultrasound and carotid angiograms were obtained prior to CAS. Every patient underwent a baseline neurological evaluation that included a NIHSS by a board-certified neurologist prior to CAS. Antiplatelet therapy in the form of aspirin 325 mg and clopidogrel 75 mg was initiated at least 48 hours prior to the CAS and continued for at least 4 weeks post procedure unless otherwise indicated. No documented allergy to aspirin or clopidogrel was encountered in our cohort.
Carotid angioplasty and stenting protocol. All CAS procedures were performed in the cardiac catheterization laboratory at Providence Hospital and Medical Center in Southfield, Michigan. All procedures were performed by two experienced, board-certified interventional cardiologists. Antihypertensive medications were discontinued for 36 hours prior to intervention. Intravenous sedation was minimized and frequent neurological assessments were performed during the procedure according to established protocols. Intravenous heparin was used as needed for anticoagulation to maintain an activated clotting time (ACT) >275 seconds throughout the duration of the procedure. Femoral access was used in all patients with a 6 Fr sheath inserted in the femoral artery and a 7 Fr sheath inserted in the femoral vein. Venous access was used for fluid hydration and standby RV pacing as necessary. Selective access to the common carotid artery was obtained with a 6 Fr Shuttle Select sheath (Terumo Medical Corporation). An embolic protection device (EPD) was used in 269 cases (≈99%). Only 2 cases (≈1%) were performed without EPDs due to anatomical challenges. The Rx Accunet (Abbott Vascular) embolic protection system was used in 258 patients (95.2%). The self-expanding Acculink Stent (Abbott Vascular) was used in 258 patients (95.2%). Postdilatation was performed after stent deployment on the majority of lesions to further optimize apposition of the stent struts. Final angiograms including cerebral angiograms were obtained. Intravenous atropine (1 mg) was given at the discretion of the operator, prior to balloon inflation or stenting, to prevent severe bradycardia.
All patients were admitted to a telemetry unit post intervention. Procedural success was defined by <30% residual stenosis determined by post-stent placement angiography using The North American Symptomatic Carotid Endarterectomy Trial (NASCET)20 criteria. The hospital outcomes that were assessed included access-site complications requiring blood transfusion or surgical intervention, and bradycardia requiring temporary pacing. The clinical endpoints included cerebrovascular accident, myocardial infarction, and death in the perioperative period. Cardiac biomarkers were collected only if signs or symptoms of myocardial ischemia/infarction were noted. A detailed neurologic assessment was performed on all patients by a board-certified neurologist 24 hours after the procedure, prior to discharge, and at 30-day follow-up exam.
Results
A total of 259 carotid interventions (95.6%) met the criteria for angiographic success, with 112 patients (41.3%) having 0% residual stenosis. Two minor neurologic (presumably embolic) events (0.7%) were encountered.
One patient, a 57-year-old Caucasian male with a medical history significant for advanced coronary artery disease and ischemic cardiomyopathy, experienced a TIA. He developed right lower-extremity paresthesia less than 24 hours after stenting of an 80% ostial left internal carotid artery stenosis. He improved significantly within 48 hours and was discharged home. His 30-day NIH scale was 0.
A second patient — a 66-year-old female with history of tobacco abuse, established history of peripheral vascular disease, and previous left carotid endarterectomy— developed a minor stroke. She had undergone stenting of a 90% left CEA restenosis. Although her neurologic evaluation was unremarkable 24 hours after CAS, two days later she complained of right-side vision loss and was diagnosed with an embolic event. Her 30-day NIH scale was 1 due to her visual defect.
The only mortality (0.4%) occurred in a 66-year-old Caucasian male with a medical history remarkable for advanced peripheral artery disease and coronary artery disease who underwent a successful stenting of a 95% right internal carotid artery stenosis. The initial stenosis was reduced to less than 10% residual and the patient was subsequently discharged home in a stable condition. The patient’s wife stated that he sustained a fall one week after the procedure and was transferred to the hospital. CT of the brain demonstrated intracranial hemorrhage, which ultimately led to the patient’s demise. It is unknown whether the patient’s fall resulted in the intracranial hemorrhage or whether an intracranial bleed may have led to his fall, especially in light of the patient’s use of dual antiplatelet therapy.
There were no major access-site complications that required surgical intervention, blood transfusion, or prevented discharge within 24 hours of stent placement. No perioperative myocardial infarctions were encountered. There were no prolonged episodes of bradycardia that required transvenous pacing.
Discussion
Our report is a case series from a medium-size, tertiary care teaching community hospital. Our intent was to evaluate the efficacy and safety of performing CAS in such a setting in a high-risk population. The periprocedural myocardial infarction, TIA, stroke, and death were measured during the first 30 days and compared to those of previous large-scale trials, specifically the widely referenced SAPPHIRE and CREST trials.17,18
Two of 271 patients (0.7%) experienced a minor neurologic (presumably embolic) event post procedure. One (0.35%) was an ipsilateral TIA, and the second (0.35%) was a small contra-lateral stroke. In the SAPPHIRE trial, the percentage of minor ipsilateral stroke and minor non-ipsilateral stroke was 2.5% and 0.6%, respectively, in the actual treatment analysis arm at 30 days. The percentage of major non-ipsilateral stroke was 0.6% at 30 days.
In the CREST trial, the percentage of minor ipsilateral stroke and minor non-ipsilateral stroke was 2.9 ± 0.5% and 0.3 ± 0.2%, respectively, with 0.9 ± 0.3% experiencing a major ipsilateral stroke (data given as percentage ± standard error of mean).
The discrepancy between the reported results may be attributed in part to operator experience. The median number of procedures per operator in the SAPPHIRE trial was about 64. In the CREST trial, two operator categories were defined; the first included operators who performed more than 30 procedures and the second included operators who performed fewer than 30 procedures. For the first category, operators submitted their entire carotid stent experience for up to 50 consecutive patients including follow-up information beyond 30 days. Those operators then underwent further training on the use of both the EPD and the carotid stent systems. Those operators were then required to perform 20 CAS procedures at their institutions before participating in the randomized study or undergo further training. More strict criteria were applied for operators with fewer than 30 CAS procedures.21 In comparison, at PHMC we have performed 50-75 CAS annually over almost a decade.
Also, the difference in the results could be partly due to the usage of EPD systems. We used EPD systems in 99% of the cases. The embolic protection devices were used in 95.6% of the patients who underwent CAS in SAPPHIRE and 96.1% of patients in the CREST trial who were assigned to CAS arm.
The benefit of EPD systems was also noted in the experience reported by Halabi et al.22
In their series, 49 procedures (44%) were performed with distal protection devices. In this group, the in-hospital mortality was 0%; furthermore, no major or minor strokes were reported, but 1 retinal artery emboli (2%) was experienced. TIA was documented in 3 patients (6.1%) with a trend toward significant difference between de novo lesions in comparison with lesions in patients with prior CEA (0% vs 12.5%, respectively; P=.08). Kaplan-Meier curves for event-free survival (death/stroke) demonstrated that the initial benefit noted with the use of EPD systems was maintained during longer-term follow-up. In their experience, the 30-day outcomes were 0.9% for mortality rate, 0.9% for major strokes, 1.9% for minor strokes, 0.9% for retinal artery emboli, and 3.8% for TIAs.
During the follow-up period, 1 patient (0.35%) died. In comparison, the SAPPHIRE trial reported a 0.6% death rate at 30 days in the actual treatment analysis arm. The CREST trial reported a 0.7 ± 0.2% death rate in the periprocedural period. The only periprocedural death that occurred in our patient population was a 66-year-old male. His death appears to have been related to a fall sustained post procedure, resulting in an intracranial bleed. It is unknown whether a stroke prompted his fall or whether the dual antiplatelet therapy he was receiving contributed to the severity of his bleed.
In the SAPPHIRE trial, myocardial infarction was defined by a creatine kinase level more than twice the upper range of normal in addition to a positive MB fraction. The authors reported 0% and 1.9% for Q-wave and non-Q wave myocardial infarction, respectively, in the actual treatment analysis arm at 30 days.
The CREST trial defined myocardial infarction as a creatine kinase MB or troponin level equal to or greater than twice the upper limit of normal in addition to ischemic symptoms or ischemic electrocardiographic findings. They reported a 1.1 ± 0.3% rate of myocardial infarction in the periprocedural period (data given as percentage ± standard error of mean).
Our series revealed no incidence of periprocedural myocardial infarction. In our series, myocardial ischemia or infarctions were defined based on clinical criteria such as chest pain or ischemic symptoms. Although our definition of myocardial infarction has lower sensitivity than the SAPPHIRE and CREST trials, it has higher specificity, especially in the high-risk patients with many factors that could lead to supply-demand mismatch rather than plaque rupture as the cause for elevated biomarkers.
No vascular complications were seen (specifically in regard to the access site), despite 149 patients, or roughly 55% of the cohort, having a history of peripheral arterial disease. No patients undergoing CAS were noted to have periprocedural bradycardia or require temporary pacing. Our institution’s practice of empirically administering atropine prior to balloon inflation may have contributed to these findings. This is consistent with findings by the group of Cayne et al.23
Study limitations. Our results are based on a retrospective, nonrandomized, single-center registry that was conducted to assess the safety and efficacy of CAS in patients determined to be at high risk for CEA. Therefore, the results and the conclusion should be viewed within the context of such limitations.
Conclusions
This is a retrospective review of our carotid artery angioplasty and stenting program that was launched in 2005. Our findings indicate that, with adequate volumes and qualified operators and ancillary staff, our institution has been able to safely and effectively introduce and carry out CAS as an alternative to CEA in patients that are at high risk for surgery. We did not compare our patient population to the population studied in SAPPHIRE and CREST. However, we believe that our patient population is a good example and a reasonable reflection of other medium and even large hospitals that provide medical care to large metropolitan areas. More long-term follow-up and further retrospective review of the continually growing CAS population at our hospital and other similar community hospitals would likely provide added insight into currently demonstrated safety and efficacy.
Acknowledgment. The authors would like to express their appreciation to Samuel Tekyi-Mensah, PhD and Fernando Alcocer, MD, and to Providence Hospital research lab staff for their assistance in data collection and statistical analyses.
References
- Wolf PA, Clagett GP, Easton JD, et al. Preventing ischemic stroke in patients with prior stroke and transient ischemic attack: a statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke. 1999;30(9):1991.
- Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statistics — 2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117(4):e25-e146.
- Medical Expenditure Panel Survey (MEPS) of the Agency for Healthcare Research and Quality (AHRQ). Household component summary data table. Available at: https://meps.ahrq.gov/mepsweb/data_stats/tables_compendia_hh_interactive.jsp?_SERVICE=MEPSSocket0&_PROGRAM=MEPSPGM.TC.SAS&File=HCFY2009&Table=HCFY2009%5FCNDXP%5FC&_Debug=. Accessed May 30, 2012.
- Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics — 2011 update: a report from the American Heart Association. Circulation. 2011;123(4):e18-e209. Epub 2010 Dec 15.
- Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: final data for 2007. Natl Vital Stat Rep. 2009;57(14):1-134.
- Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics — 2012 update: a report from the American Heart Association. Circulation. 2012;125(1):e2-e220.
- Asplund K, Stegmayr B, Peltonen M. From the twentieth to the twenty-first century: a public health perspective on stroke. Ginsberg MD, Bogousslavsky J, eds. Cerebrovascular Disease: Pathophysiology, Diagnosis, and Management. Malden, Massachusetts: Blackwell Science, 1998:901-918.
- Incidence and Prevalence: 2006 Chart Book on Cardiovascular and Lung Diseases. Bethesda, Maryland: National Heart, Lung, and Blood Institute; 2006.
- Liberato B, Chong K, Lee H, et al. Degree of carotid artery stenosis and potential eligibility for intervention: the Northern Manhattan Stroke Study (Abstr). Neurology. 2004;62(Suppl 5):A139.
- Fine-Edelstein JS, Wolf PA, O’Leary DH, et al. Precursors of extra-cranial carotid atherosclerosis in the Framingham Study. Neurology. 1994;44(6):1046-1050.
- Barnett HJM, Taylor DW, Haynes RB, et al. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991;325(7):445-453.
- Warlow C. MRC European Carotid Surgery Trial: interim results for symptomatic patients with severe (70-99%) or with mild (0-29%) carotid stenosis. Lancet. 1991;337(8752):1235-1243.
- Farrell B, Fraser A, Sandercock P, et al. Randomized trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351(9113)1379-1387.
- Hobson RW 2nd, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. N Engl J Med. 1993;328(4):221-227.
- Walker MD, Marler JR, Goldstein M, et al. Endarterectomy for asymptomatic carotid artery stenosis. JAMA. 1995;273(18):1421.
- Halliday A, Mansfield A, Marro J, et al. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet. 2004;363(9420):1491-1502.
- Yadav JS, Wholey MH, Kuntz RE, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Brott TG, Hobson RW 2nd, Howard G, et al. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med. 2010;363(1):11-23.
- www.ninds.nih.gov/doctors/NIH_Stroke_Scale.pdf
- Barnett HJM, Peerless SJ, Fox AJ, et al. North American Symptomatic Carotid Endarterectomy Trial. Methods, patient characteristics, and progress. Stroke. 1991;22(6):711-720.
- https://www.nejm.org/doi/suppl/10.1056/NEJMoa0912321/suppl_file/nejmoa0912321_appendix.pdf
- Halabi M, Gruberg L, Pitchersky S, et al. Carotid artery stenting in surgical high-risk patients. Catheter Cardiovasc Interv. 2006;67(4):513-518.
- Cayne NS, Faries PL, Trocciola SM, et al. Carotid angioplasty and stent-induced bradycardia and hypotension: impact of prophylactic atropine administration and prior carotid endarterectomy. J Vasc Surg. 2005;41(6):956-961.
___________________________________________
From the Division of Cardiology, Providence Hospital and Medical Center, Southfield, Michigan.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted May 31, 2012, provisional acceptance given July 1, 2012, final version accepted July 25, 2012.
Address for correspondence: Ghassan Dalloul, MD, 16001 W. 9 Mile Rd, Southfield, MI 48075. Email: gdalloul79@hotmail.com

