

Balloon-Assisted Sheathless Transradial Intervention (BASTI) Using 5 Fr Guiding Catheters
Abstract: Background. The sheathless approach to transradial percutaneous coronary intervention (PCI) has recently gained popularity among interventionalists. However, technical problems and lack of approved equipment in the United States has limited its applicability. We describe a new approach, balloon-assisted sheathless transradial intervention (BASTI) that can ease the use of 5 Fr sheathless guiding catheters and decrease complication rates. Methods. Twenty-seven consecutive patients undergoing staged elective PCI were enrolled. Radial artery access was obtained using the BASTI method — inflation of a compliant coronary balloon at the tip of the guiding catheter was used to ease the transition of the catheter into the skin. The guidewire and coronary balloon were reused during the PCI. Each of the patients had clinical postprocedure follow-up at radial compression device release, and at 1 day, 7 days, and 30 days. Major adverse cardiac events and access-site complications, including radial artery occlusion (RAO), were documented. Results. In this consecutive series, we successfully attempted (27/27) BASTIs. There were no difficulties in obtaining radial artery access with the 5 Fr sheathless guiding catheter. Two patients had balloon rupture during initial radial artery access, but were successfully re-attempted with a higher balloon inflation pressure. All patients then underwent successful coronary intervention. There were no adverse events or procedure-related complications at any time period during follow-up. Conclusion. BASTI is a feasible alternative to conventional techniques and may reduce vascular access-site complications and patient morbidity in a cost-effective manner.
J INVASIVE CARDIOL 2012;24(5):231-233
Key words: access-site complications, balloon rupture, balloon-assisted sheathless transradial intervention
_______________________________________________
The transradial approach for percutaneous coronary intervention (PCI) is rapidly becoming a popular method among interventional cardiologists. A lower rate of major access-site complications and earlier patient ambulation make this method more appealing in comparison to the transfemoral approach.1-5 Radial artery occlusion (RAO) is one of the few postprocedural complications and can occur in up to 7%-12% of transradial cases.6 Although largely asymptomatic, the development of RAO may preclude future intervention via the same radial artery. The size of the introducer sheath has been shown to influence the incidence of RAO7 and advancements in the field have thus focused on the miniaturization of the introducer sheath and/or guide catheters in hope of decreasing RAO rates and reducing patient morbidity.
PCI via 5 Fr guiding catheter is accepted as the preferred route by many interventional cardiologists. Benefits of 5 Fr PCI include a smaller size and lower likelihood for spasm. The catheter also employs a soft tip, which makes it less traumatic when cannulating coronary arteries. Studies comparing 5 Fr and 6 Fr catheters via transradial approach favored the use of a 5 Fr catheter system.8,9 Furthermore, the transradial approach with 6 Fr or larger guiding catheters is not always feasible, especially in elderly patients or patients with small radial artery diameters.
Previous studies using large-bore guiding catheters via a sheathless approach have shown promise in decreasing RAO rates.10-12 Consequently, Mizuno et al13 introduced the use of a 5 Fr sheathless guiding catheter, which has the equivalent outer diameter of a 3 Fr introducer sheath; however, this system is not available worldwide. In this report, we describe the use of balloon-assisted inflation during initial radial artery access via the sheathless approach using a 5 Fr guiding catheter. This may represent a new technique in 5 Fr sheathless transradial coronary interventions that is both feasible and cost effective.
Methods
The balloon-assisted sheathless transradial intervention (BASTI) technique was applied during 5 Fr transradial coronary interventions from September 1, 2011 to October 30, 2011. This study was approved by the individual hospital’s institutional review board. After obtaining informed written consent, 27 consecutive patients undergoing staged elective PCI using a 5 Fr guiding catheter were enrolled. At the end of the procedure, hemostasis over the radial artery was obtained using a radial artery compression device (TR Band, Terumo) and patent hemostasis technique.6 In brief, the TR Band was inflated at the site of radial puncture to facilitate removal of the sheath thereafter. Ipsilateral ulnar artery was manually compressed and then the TR Band was deflated slowly until the plethysmographic signal returned, which confirmed radial artery patency. The TR Band was left in place for 2 hours for hemostasis. RAO was assessed by performing a “reverse” Barbeau test and was defined as an absence of plethysmographic signal with ulnar compression indicating absence of antegrade radial artery flow. RAO was assessed by the investigators at clinically mandated follow-up visits. All patients’ demographic and procedural data were entered into a dedicated database. Each of the patients undergoing BASTI had clinical follow-up postprocedure, and at 1 day, 7 days, and 30 days. The composite clinical endpoint of major adverse cardiac events (including death, myocardial infarction, and stroke), and access-site complications, including RAO rates, were obtained.
Balloon-Assisted Sheathless Transradial Intervention (BASTI)
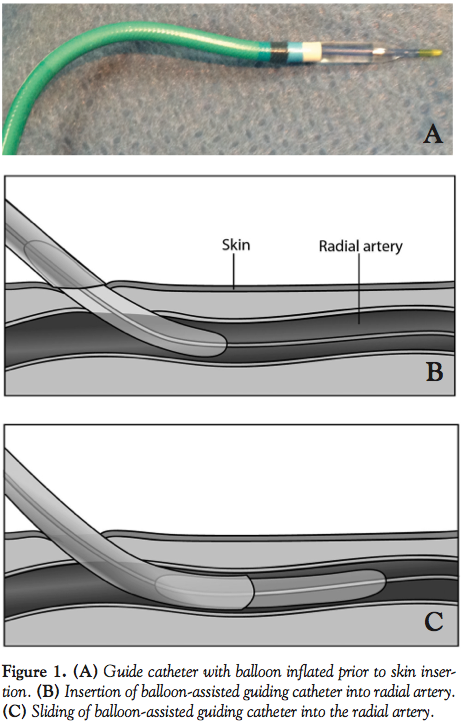 After initial engagement of the right radial artery using a 20-gauge Jelco angiocath with a cocktail infusion consisting of heparin 5000 U, nitroglycerin 100 µg, and verapamil 1 mg, a 0.014″ Runthrough guidewire (Terumo) was advanced into the subclavian artery or ascending aorta. Once the guidewire tip was visualized in the appropriate location, a 5 Fr guiding catheter was advanced over the guidewire directly with the inflated balloon together. To ease insertion of the guiding catheter, a 2.0 mm x 15 mm compliant balloon (Maverick; Boston Scientific) tip was partially inflated with at least 8 atm (Figure 1A) while the guiding catheter was slowly inserted into skin (Figure 1B) and then the radial artery (Figure 1C). Once the catheter reached the subclavian artery or ascending aorta the balloon was deflated and the 0.014″ guidewire is exchanged for a standard 0.035″ guidewire. It is recommended to perform coronary artery engagement of the guiding catheter with the support of a 0.035″ guidewire, rather than a 0.014″ guidewire, due to the thin wall of the 5 Fr guiding catheter and concern for a catheter kink at the skin entry site. The rest of the interventional procedure proceeded as per usual protocol.
After initial engagement of the right radial artery using a 20-gauge Jelco angiocath with a cocktail infusion consisting of heparin 5000 U, nitroglycerin 100 µg, and verapamil 1 mg, a 0.014″ Runthrough guidewire (Terumo) was advanced into the subclavian artery or ascending aorta. Once the guidewire tip was visualized in the appropriate location, a 5 Fr guiding catheter was advanced over the guidewire directly with the inflated balloon together. To ease insertion of the guiding catheter, a 2.0 mm x 15 mm compliant balloon (Maverick; Boston Scientific) tip was partially inflated with at least 8 atm (Figure 1A) while the guiding catheter was slowly inserted into skin (Figure 1B) and then the radial artery (Figure 1C). Once the catheter reached the subclavian artery or ascending aorta the balloon was deflated and the 0.014″ guidewire is exchanged for a standard 0.035″ guidewire. It is recommended to perform coronary artery engagement of the guiding catheter with the support of a 0.035″ guidewire, rather than a 0.014″ guidewire, due to the thin wall of the 5 Fr guiding catheter and concern for a catheter kink at the skin entry site. The rest of the interventional procedure proceeded as per usual protocol.
Results
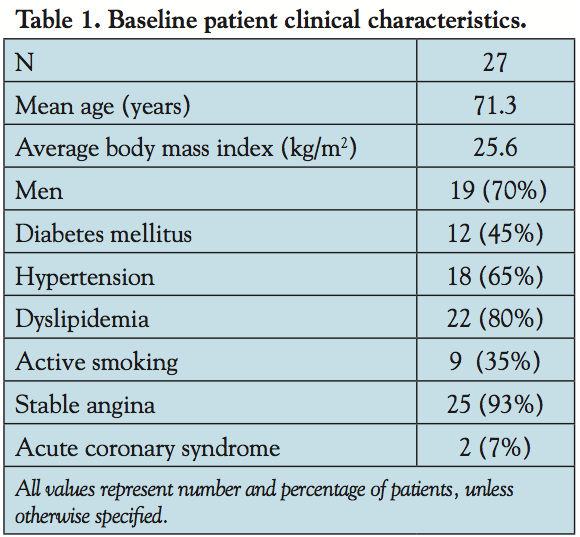 In this series, we successfully performed all 5 Fr sheathless transradial coronary interventions using the BASTI method for initial radial artery access. Baseline characteristics of the patients (Table 1) and procedural parameters (Table 2) are shown. Bifurcation lesions were found in 48% of cases. All bifurcation lesions were treated via a provisional stenting approach with a jailed guidewire in the side branch only. All side-branch lesions exhibited TIMI 3 flow post main branch stent placement and did not require any further intervention. Type C lesions
In this series, we successfully performed all 5 Fr sheathless transradial coronary interventions using the BASTI method for initial radial artery access. Baseline characteristics of the patients (Table 1) and procedural parameters (Table 2) are shown. Bifurcation lesions were found in 48% of cases. All bifurcation lesions were treated via a provisional stenting approach with a jailed guidewire in the side branch only. All side-branch lesions exhibited TIMI 3 flow post main branch stent placement and did not require any further intervention. Type C lesions 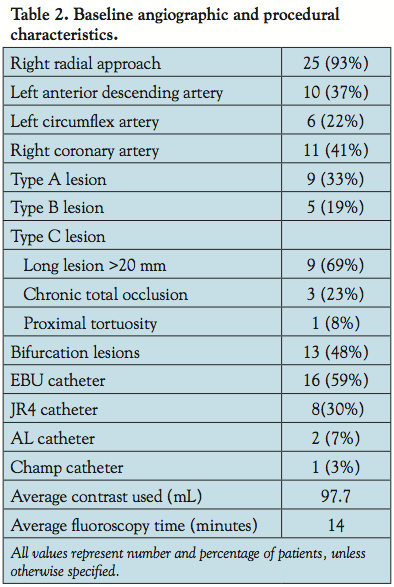 were encountered in 48% of cases and included lesions containing long disease segments ≥20 mm, chronic total occlusions, or tortuosity of the proximal vessel segment. The average amount of contrast used was 97.7 mL while the average fluoroscopy time was 14 minutes. There was no difficulty in stent deployment and no cases required stent withdrawal. Clinical outcomes including RAO are shown in Table 3. There were no procedure-related complications, such as guide catheter
were encountered in 48% of cases and included lesions containing long disease segments ≥20 mm, chronic total occlusions, or tortuosity of the proximal vessel segment. The average amount of contrast used was 97.7 mL while the average fluoroscopy time was 14 minutes. There was no difficulty in stent deployment and no cases required stent withdrawal. Clinical outcomes including RAO are shown in Table 3. There were no procedure-related complications, such as guide catheter 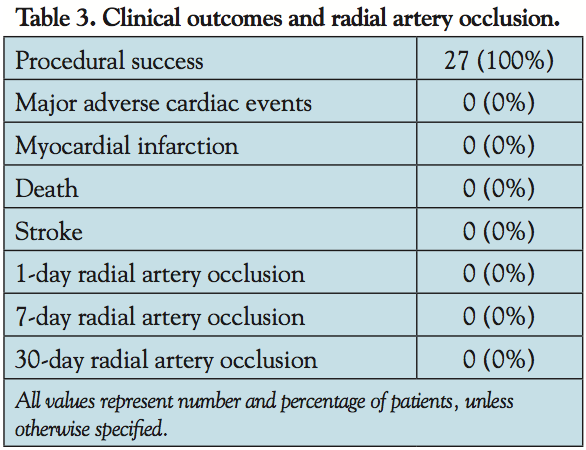 dissection, to report. No patient experienced radial artery spasm or complained of access-site pain during catheter insertion or withdrawal. In 25 out of 27 patients, radial artery access was obtained with one attempt. Two patients had the balloon rupture during initial attempt at skin insertion. After a second attempt was performed using a higher pressure of balloon inflation and ensuring adequate skin dilation by using a 4 Fr sheath dilator (outside diameter, 0.035″), radial artery access was successfully obtained in these patients as well. All patients underwent successful PCI. There were no adverse events or procedure-related complications at any time period during follow-up. Radial artery patency was confirmed in all patients at each time point.
dissection, to report. No patient experienced radial artery spasm or complained of access-site pain during catheter insertion or withdrawal. In 25 out of 27 patients, radial artery access was obtained with one attempt. Two patients had the balloon rupture during initial attempt at skin insertion. After a second attempt was performed using a higher pressure of balloon inflation and ensuring adequate skin dilation by using a 4 Fr sheath dilator (outside diameter, 0.035″), radial artery access was successfully obtained in these patients as well. All patients underwent successful PCI. There were no adverse events or procedure-related complications at any time period during follow-up. Radial artery patency was confirmed in all patients at each time point.
Discussion
Recently, the sheathless approach to transradial PCI has gained popularity among interventionalists throughout the world including the United States.10-12 This approach embraces the current trend toward the miniaturization of catheters and allows for catheter upsizing of approximately 2 Fr sizes without increasing traumatic risk to the radial artery commonly associated with the introducer sheath. In transradial catheterization, the use of smaller catheters decreases radial access-site complications, especially RAO. According to Saito et al,7 a radial artery-to-sheath ratio less than 1 is predictive of radial artery occlusion. Therefore, 5 Fr guiding catheters, smaller than the standard catheter used for transradial PCI, will lessen the traumatic burden to the radial artery and decrease the risk of complications such as spasm, bleeding, or occlusion. The 5 Fr sheathless hydrophilic guiding catheter system (Virtual 3 Fr; Medikit) has been described and benefits include a puncture-site injury equivalent to a conventional 3 Fr introducer sheath.13,14 However, this system employs the use of a dedicated central dilator that is currently unavailable in the United States.
There are few reports using a multipurpose or Flexor sheath (Cook Medical, Inc) as an inside dilator in the sheathless approach.11,12 One of the discrepancies in these reports is the lack of smooth transition between the dilator and the guiding catheters. A rough transition point may theoretically cause more trauma to the radial artery, and subsequently more RAO. A recent study by From et al15 described a similar balloon-assisted technique, but the operators were unsuccessful in obtaining radial artery access. Furthermore, the authors quickly point out that the technique was only attempted once, and therefore not adequately studied. Our case series describes an innovative method that may allow for more widespread use of the 5 Fr sheathless system and its advantages. Here we report 27 consecutive cases employing the BASTI method for radial artery access. The inflated balloon tip on the catheter provides a smooth seal and low trauma during transition from skin to artery. Since catheter size and site of arterial puncture are the major predictors of access-site complications, the use of a balloon-assisted 5 Fr sheathless system via the transradial approach may thus improve patient comfort and minimize the risks of access-site complications including asymptomatic RAO. While there were 2 cases of balloon rupture during initial skin insertion, this was easily corrected after adequate skin dilation and higher balloon inflation during the second attempt.
Cost may be a factor when considering the sheathless approach. The use of a multipurpose or Flexor sheath may add to catheterization expenses; however, the BASTI method enables the operators to use available equipment and should not cause a major cost increase. Furthermore, the guidewires and balloon-tipped catheters used during initial radial artery access can theoretically be utilized again during the coronary intervention.
This technique is an innovative application of current market-approved interventional equipment. However, several limitations still exist. First, catheters with smaller inner diameters have important limitations with regard to devices and techniques that can be used (ie, kissing balloon stents, rotational atherectomy, etc.). Second, any sheathless system lacks the inherent support structure that an introducer sheath provides, and therefore catheter kinking can be a concern. Third, if procedural difficulties arise, catheter exchange will be cumbersome in a sheathless system. Finally, this is a small sample size and additional experience with more patients is required to accurately measure success and lack of complications associated with this procedure. A larger, multicenter study is underway to assess the feasibility and safety of BASTI.
Conclusion
5 Fr BASTI is a feasible alternative to conventional techniques and may reduce vascular access-site complications and patient morbidity in a cost-effective manner.
References
- Kiemeneij F, Laarman GJ, Odekerken D, et al. A randomized comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches: the ACCESS study. J Am Coll Cardiol. 1997;29(6):1269-1275.
- Agostoni P, Biondi-Zoccai GL, Benedictis LD, et al. Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures. J Am Coll Cardiol. 2004;44(2):349-354.
- Bertrand OF, Rao SV, Pancholy S, et al. Transradial approach for coronary angiography and interventions: results of the first international transradial practice survey. JACC Cardiovasc Interv. 2010;3(10):1022-1031.
- Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377(9775):1409-1420.
- Caputo RP, Tremmel JA, Rao S, et al. Transradial arterial access for coronary and peripheral procedures: executive summary by the transradial committee of the SCAI. Catheter Cardiovasc Interv. 2011 May 4. doi: 10.1002/ccd.23052. [Epub ahead of print]
- Pancholy S, Coppola J, Patel T, Roke-Thomas M. Prevention of radial artery occlusion-patent hemostasis evaluation trial (PROPHET study): a randomized comparison of traditional versus patency documented hemostasis after transradial catheterization. Catheter Cardiovasc Interv. 2008;72:335-340.
- Saito S, Hajime I, Hosokawa G, Tanaka S. Influence of the ratio between radial artery inner diameter and sheath outer diameter on radial artery flow after transradial coronary intervention. Cathet Cardiovasc Interv. 1999;46(2):173-178.
- Dahm JB, Vogelgesang D, Hummel A, et al. A randomized trial of 5 vs. 6 French transradial percutaneous coronary interventions. Catheter Cardiovasc Interv. 2002;57(2):172-176.
- Gwon HC, Doh JH, Choi JH, et al. A 5 Fr catheter approach reduces patient discomfort during transradial coronary intervention compared with a 6 Fr approach: a prospective randomized study. J Interv Cardiol. 2006;19(2):141-147.
- Mamas M, D’Souza S, Hendry C, et al.Use of the sheathless guide catheter during routine transradial percutaneous coronary intervention: a feasibility study. Catheter Cardiovasc Interv. 2010;75(4):596-602.
- From AM, Gulati R, Prasad A, Rihal CS. Sheathless transradial intervention using standard guide catheters. Catheter Cardiovasc Interv. 2010;76(7):911-996.
- Kwan J, Huang Y, Vales L, et al. 7-Fr sheathless transradial percutaneous coronary intervention. Catheter Cardiovasc Interv. 2011;77(Suppl 1):S1-S156.
- Mizuno, S, Takeshita S, Taktani Y, Saito S. Percutaneous coronary intervention using a virtual 3 Fr guiding catheter. Catheter Cardiovasc Inverv. 2010;75(7):983-988.
- Takeshita S, Saito S. Transradial coronary intervention using a novel 5 Fr sheathless guiding catheter. Catheter Cardiovasc Interv. 2009;74(6):862-865.
- From AM, Bell MR, Rihal, CS, Gulati R. Minimally invasive transradial intervention using sheathless standard guiding catheters. Catheter Cardiovasc Interv. 2011 May 11. doi: 10.1002/ccd.23013. [Epub ahead of print]
_______________________________________________
From the 1Department of Cardiology, Beth Israel Medical Center, New York, New York, 2Department of Cardiology, Wright Center for Graduate Medical Education, Scranton, Pennsylvania, and 3Department of Cardiology, Smt. N.H.L. Medical Municipal College, Sheth V.S. General Hospital, Gujarat, India.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted December 28, 2011, provisional acceptance given January 23, 2012, final version accepted February 7, 2012.
Address for correspondence: Justin A. Ratcliffe, MD, Beth Israel Medical Center – Heart Institute, 5th Floor Baird Hall, First Avenue at 16th Street, New York, NY 10003. Email: jratcliffe@chpnet.org

