

An Angiographic Consideration Prior to Coronary Bypass Graft Surgery: Importance of Routine Selective Angiography of the Internal Mammary Artery Prior to Myocardial Revascularization
View the video clip from this article in the multimedia section at https://invasivecardiology.com/content/angiographic-consideration-prior-coronary-bypass-graft-surgery.
ABSTRACT: The collateral perfusion via the hypertrophied internal thoracic arteries and rich anastomosis between the epigastric arteries reconstituting femoral artery are an important route in patients with peripheral vascular disease (chronic aortoiliac occlusion), providing blood flow to the lower extremities. Selective angiography of the internal thoracic artery plays a major role in the preoperative evaluation in patients with severe aortoiliac occlusive disease undergoing coronary bypass surgery and may prevent a major potential postoperative complication of acute lower extremity ischemia in these patients.
J INVASIVE CARDIOL 2012;24(5):E87-E89
_____________________________________________
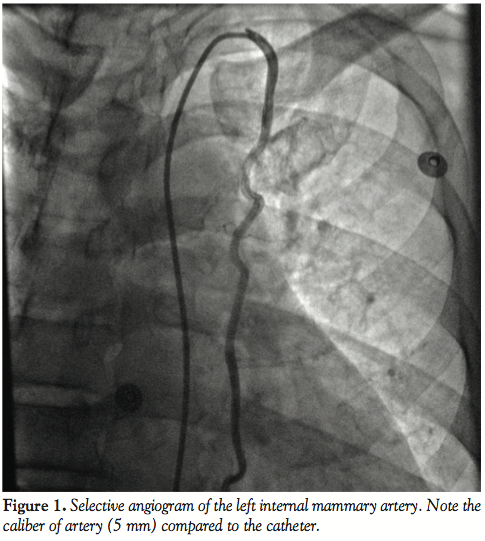
The utilization of internal thoracic arteries for coronary revascularization is well established and preferred to ensure prolonged graft patency. We report a case of a 55-year-old male who had undergone coronary artery bypass graft surgery (CABG) using only venous grafts to the left anterior descending (LAD) and first diagonal coronary arteries. The left internal mammary artery (LIMA) was not used due to extensive collateral formation from the left internal thoracic via superior and inferior epigastric arteries to the left femoral artery compensates the chronically occluded left common and external iliac arteries. Selective angiogram of the LIMA demonstrated it to be larger than normal (5 mm). The caliber is considerably larger than usual (≥3 mm). Further interrogation demonstrated it to be collaterals to the left common femoral artery via the epigastric arteries.
 Case Report. A 55-year-old male admitted with symptoms of unstable angina pectoris. He had history of previous anterior wall myocardial infarction with multiple stents in LAD over prior 2 years. He showed symptoms of claudication with no history of recent tobacco use. On physical examination there was no significant radial or femoral pulse delay, or evidence of systolic blood pressure gradient difference between the upper and lower extremities. The chest radiograph showed no evidence of rib notching or mediastinal widening. Coronary angiography revealed severe stenosis of ostial LAD extending into proximal LAD with a long segment stenosis along with stent restenosis. There was also a high-grade stenosis of the ostium of the first diagonal artery.
Case Report. A 55-year-old male admitted with symptoms of unstable angina pectoris. He had history of previous anterior wall myocardial infarction with multiple stents in LAD over prior 2 years. He showed symptoms of claudication with no history of recent tobacco use. On physical examination there was no significant radial or femoral pulse delay, or evidence of systolic blood pressure gradient difference between the upper and lower extremities. The chest radiograph showed no evidence of rib notching or mediastinal widening. Coronary angiography revealed severe stenosis of ostial LAD extending into proximal LAD with a long segment stenosis along with stent restenosis. There was also a high-grade stenosis of the ostium of the first diagonal artery.
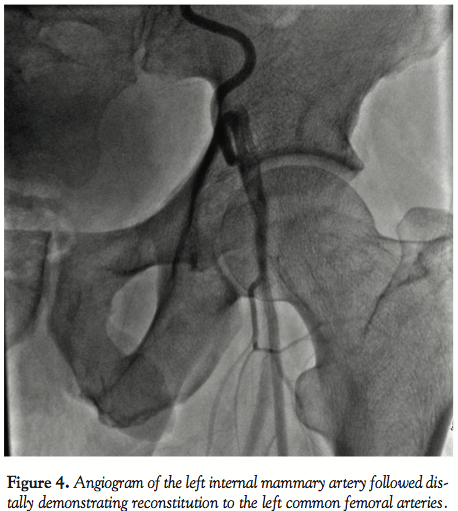
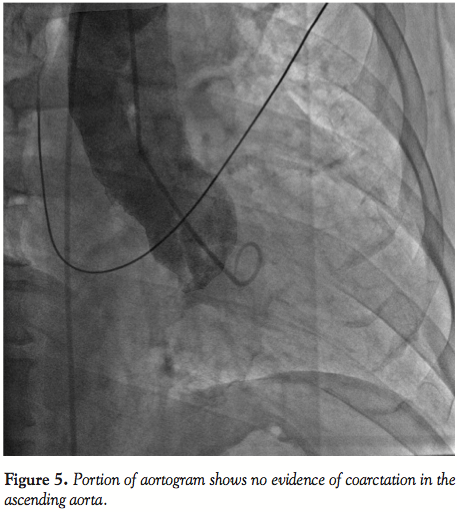
 Imaging of the right coronary and circumflex arteries revealed no significant lesion. The left ventricular ejection fraction was normal. The injection into the LIMA showed marked increased diameter (Figure 1) with unusually long collaterals extending to the left common femoral artery (Figure 2). There was a total occlusion of the left common femoral artery (Figure 3) with reconstitution of the common femoral artery from the LIMA collaterals (Figure 4). There was no evidence of coarctation in the proximal ascending aorta identified of the aorta on this or prior coronary angiography studies (Figure 5).
Imaging of the right coronary and circumflex arteries revealed no significant lesion. The left ventricular ejection fraction was normal. The injection into the LIMA showed marked increased diameter (Figure 1) with unusually long collaterals extending to the left common femoral artery (Figure 2). There was a total occlusion of the left common femoral artery (Figure 3) with reconstitution of the common femoral artery from the LIMA collaterals (Figure 4). There was no evidence of coarctation in the proximal ascending aorta identified of the aorta on this or prior coronary angiography studies (Figure 5).
 Discussion. Patients with peripheral vascular disease have a high prevalence of coronary artery disease and frequently undergo CABG. There are reports of acute limb ischemia after internal thoracic artery harvesting.1,2,3,4 Selective angiographic visualization of the internal mammary artery is an essential part of the preoperative evaluation in patients with severe peripheral vascular disease undergoing CABG.5 Based on the superior long-term results, the LIMA is widely used for CABG. However, the vessel can play an important role as a collateral source to chronically ischemic lower limbs from the iliac artery occlusion.2,6 Along with other visceral and parietal collateral pathways, the LIMA, superior epigastric artery, and inferior epigastric artery route is a major collateral pathway to the arteries of the lower extremities in patients with chronic aortoiliac occlusive disease.4,7
Discussion. Patients with peripheral vascular disease have a high prevalence of coronary artery disease and frequently undergo CABG. There are reports of acute limb ischemia after internal thoracic artery harvesting.1,2,3,4 Selective angiographic visualization of the internal mammary artery is an essential part of the preoperative evaluation in patients with severe peripheral vascular disease undergoing CABG.5 Based on the superior long-term results, the LIMA is widely used for CABG. However, the vessel can play an important role as a collateral source to chronically ischemic lower limbs from the iliac artery occlusion.2,6 Along with other visceral and parietal collateral pathways, the LIMA, superior epigastric artery, and inferior epigastric artery route is a major collateral pathway to the arteries of the lower extremities in patients with chronic aortoiliac occlusive disease.4,7
 Lower extremity run-off is better visualized during subclavian and/or internal thoracic arteriography than during aortography. Furthermore, a much smaller amount of contrast material is needed.6,8-10 The management strategy to avoid serious vascular complications after internal thoracic artery harvesting depends on heightened awareness of this particular vascular condition and careful choice of surgical approach.
Lower extremity run-off is better visualized during subclavian and/or internal thoracic arteriography than during aortography. Furthermore, a much smaller amount of contrast material is needed.6,8-10 The management strategy to avoid serious vascular complications after internal thoracic artery harvesting depends on heightened awareness of this particular vascular condition and careful choice of surgical approach.
 Given the consequences of this unusual entity it might be advisable to perform abdominal aortography with bilateral runoff in patients with coronary artery disease condition and clinical or sonographic evidence of peripheral vascular disease. It’s also more important to routinely perform selective angiogram of the internal mammary artery in patients with aortoiliac occlusive disease who are potential candidates for CABG. While selective internal thoracic arteriogram is an essential component of coronary angiography with the intent of referral for CABG, it is mandatory in patients with any history suggestive of concomitant lower extremity peripheral artery disease.
Given the consequences of this unusual entity it might be advisable to perform abdominal aortography with bilateral runoff in patients with coronary artery disease condition and clinical or sonographic evidence of peripheral vascular disease. It’s also more important to routinely perform selective angiogram of the internal mammary artery in patients with aortoiliac occlusive disease who are potential candidates for CABG. While selective internal thoracic arteriogram is an essential component of coronary angiography with the intent of referral for CABG, it is mandatory in patients with any history suggestive of concomitant lower extremity peripheral artery disease.
In our case the unusual caliber (5 mm) of the LIMA and its collateralization of the left common femoral artery via the epigastric artery pathway is worth documentation. This condition may be rare, but it is important to realize that such an unusual collateral pathway may be present in cases in which ordinary abdominal aortography and pelvic runoff does not reveal any obvious collaterals compensating an occluded iliac artery.
References
- de Heer LM, Buijsrogge MP, Lahpor JR. Acute limb ischemia after internal thoracic artery harvesting: a case report. J Thorac Cardiovasc Surg. 2011;141(1):e5-e7.
- Adar R, Rubinstein Z, Hirshberg A. Internal mammary artery coronary bypass and leg ischemia. J Vasc Surg. 1998;7(6):820-821.
- Ben-Dor I, Waksman R, Satler LF, et al. A further work of caution before using the internal mammary artery for coronary revascularizaion in patients with severe perpheral vascular disease. Catheter Cardiovasc Interv. 2010;75(2):195-201.
- Dietzek AM, Goldsmith J, Veith FJ, Sanchez LA, Gupta SK, Wengerter KR. Interruption of critical aortoiliac collateral circulation during nonvascular operations: a cause of acute limb-threatening ischemia. J Vasc Surg. 1990;12(6):645-653.
- Kitamura S, Inoue K, Kawachi K, et al. Lower extremity ischemia secondary to internal thoracic-coronary artery bypass grafting. Ann Thorac Surg. 1993;53(1):157-159.
- Chait A. The internal mammary artery: an overlooked collateral pathway to the leg. Radiology. 1976;121(3 Pt. 1):621-624.
- Krupski WC, Sumchai A, Effeney DJ, Ehrenfeld WK. The importance of abdominal wall collateral blood vessels. Planning incisions and obtaining arteriography. Arch Surg. 1984;119(7):854-859.
- Kim J, Won JY, Park SI, Lee DY. Internal thoracic artery collateral to the external iliac artery in chronic aortoiliac occlusive disease. Korean J Radiol. 2003;4(3):179-183.
- Vine HS, Sacks BA. Visualization of the distal arterial vessels in complete aortic occlusion. AJR Am J Roentgenol. 1980;134(4):847-848.
- Edwards EA, Lemay M. Occlusion patterns and collaterals in arteriosclerosis of the lower aorta and iliac arteries. Surgery. 1955;38(5):950-962.
_____________________________________________
From the Department of Cardiology, West Anaheim Medical Center, Anaheim, California.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted November 3, 2011, provisional acceptance given November 14, 2011, final version accepted December 14, 2011.
Address for correspondence to: Fred Shalom, MD, FACC, Department of Cardiology, West Anaheim Medical Center, 3033 West Orange Avenue, Anaheim, CA 92804. Email: fredshalommd@gmail.com

