

Age-Stratified Baseline and Outcome Characteristics of Patients Undergoing Transcatheter Aortic Valve Implantation: Results From the German Multicenter Registry
Abstract: Objectives. To analyze age dependencies in patients currently undergoing transcatheter aortic valve implantation (TAVI) based on the German TAVI registry. Background. TAVI is a promising, less invasive treatment option for surgical high-risk patients with symptomatic aortic valve stenosis, with the majority being octogenarians treated so far. Younger patients with significant co-morbidities are now increasingly considered for this procedure, but little is known about this population. Methods. The German TAVI registry is an ongoing non-randomized national multicenter study. Consecutive patients who underwent TAVI between January 2009 and June 2010 were included in this analysis. We compared baseline characteristics, procedural characteristics, and short-term clinical outcome up to 30-day follow-up. Results. A total of 1386 patients were divided into 4 roughly equally-sized groups: group A, n = 347, mean age 73.4 ± 4.5 years; group B, n = 350, mean age 80.6 ± 1.1 years; group C, n = 382, mean age 84.5 ± 1.1 years; and group D, n = 312, mean age 88.9 ± 2.2 years. Patient characteristics varied significantly, with more co-morbidities in younger patients. Technical success rates were similar in all groups (96.6%-97.7%; P=NS). 30-day major adverse event rates were similar with an all-cause mortality rate of 7.2% (A), 7.1% (B), 9.7% (C) and 8.7% (D; P=NS). Postprocedural improvement of both New York Heart Association and self-reported health status was significant in all groups, with significantly better improvements in the categories ‘mobility’ and ‘ability for self-care’ in younger patients. Conclusion. TAVI appears to be similarly safe and effective across different age groups with currently applied enrollment criteria, but younger patients present with significantly more co-morbidities. All patient populations experience functional improvements, but this is particularly pronounced for younger patients.
J INVASIVE CARDIOL 2012;24(10):531-536
Key words: transcatheter aortic valve implantation, aortic stenosis, age
________________________________________________________
Aortic valve stenosis is the most common valve disease in Western countries.1 Increasing life expectancy as well as lifestyle characteristics are resulting in a growing impact of degenerative diseases, which is the typical etiology of this valvular pathology. Surgical aortic valve replacement (SAVR) constitutes the current standard of care in the treatment of symptomatic patients resulting in effective symptom relief and near normalization of prognosis.2 For patients at increased surgical risk and those not suitable candidates for SAVR, transcatheter aortic valve implantation (TAVI) has emerged as a promising less-invasive treatment option developed over the past few years, with a growing body of evidence on safety and efficacy in this population.3-6 However, TAVI has been almost restricted thus far to very elderly patients, with a mean age of 81-83 years in published reports. The randomized PARTNER trial just showed improved survival and quality of life for TAVI compared with conservative treatment among patients who were not suitable candidates for SAVR7 in a population with a mean age of 83 years as well as similar safety and efficacy compared with SAVR in a high-risk population with a mean age of 84 years.8
In view of these favorable results, younger patients with significant co-morbidities rendering them high-risk surgical candidates are increasingly considered to undergo TAVI, carefully balancing pros and cons based on current evidence (with lack of long-term data) and guideline recommendations. At present, little is known about this younger patient population in terms of baseline characteristics and clinical outcome in current real-world practice. The present study, which is a sub-analysis of the German TAVI registry, was conducted to address this issue.
Methods
Aim of the study. The aim of this study was to identify age-dependent differences in baseline characteristics as well as procedural and short-term clinical outcome among patients with symptomatic aortic valve stenoses who underwent TAVI in routine clinical practice.
Study design and patient population. The German TAVI registry is a non-randomized national multicenter registry.9 This observational study is industry-independently financed by the Institut für Herzinfarktforschung, Ludwigshafen, Germany, and monitors current use and clinical outcome of TAVI in routine clinical practice to evaluate safety, effectiveness, and health-economical data. Starting in January 2009, participating hospitals committed to include all consecutive patients undergoing TAVI, independent of access type or device used. Patient qualified for a TAVI procedure if they fulfilled the following criteria: presence of severe symptomatic aortic valve stenosis (valve area ≤1 cm2), with or without aortic valve regurgitation and either (1) age ≥80 years and a logistic EuroScore ≥20% or (2) logistic EuroScore <20% and at least one of the following criteria: cirrhosis of liver, pulmonary insufficiency (FEV1 ≤1 L) or porcelain aorta. The patient was considered suitable to undergo a TAVI procedure if the inclusion criteria were met as confirmed by an independent senior cardiologist and senior cardiac surgeon (local heart team). Both currently commercially available devices, the Edwards SAPIEN balloon-expandable prosthesis (Edwards Lifesciences, Inc) and the Medtronic Core-Valve self-expanding device (Medtronic) with all presently established access options, namely, via transfemoral, transapical, transaortic, and transsubclavian access, were included.
The present analysis consists of all TAVI patients of this registry enrolled between January 2009 and June 2010. This population was stratified by age and divided into 4 groups, generating roughly equally-sized groups with discrete age boundaries. Safety endpoints were in-hospital and 30-day mortality, in-hospital stroke, myocardial infarction, major vascular complications, and cardiac tamponade. Efficacy endpoints were technical success, postprocedural pressure gradients, New York Heart Association (NYHA) class at 30 days as well as quality of life assessment based on the EuroQol 5d questionnaire.10
Devices and procedure. The German TAVI registry is open to all commercially available prostheses. Up to now, all patients received either the Medtronic CoreValve or the Edwards SAPIEN prosthesis, which have been described in detail elsewhere.11,12 Briefly, the Medtronic CoreValve prosthesis consists of a tri-leaflet bioprosthetic porcine pericardial tissue valve, which is mounted and sutured in a self-expanding nitinol stent frame. The profile size is 18 Fr. With the current generation, 2 different device sizes are available for different annulus dimensions: the 26 mm prosthesis for aortic annulus sizes from 20 to 23.5 mm and the 29 mm prosthesis for annulus sizes from 23.5 to 27 mm. Vascular access options for device placement are the transfemoral, transsubclavian, and transaortic routes.
The Edwards SAPIEN and more recently the Edwards SAPIEN XT device are balloon-expandable prostheses with a bovine pericardial tissue valve. Vascular access options included the transfemoral, transapical, and transaortic routes. Initial transfemoral and transapical procedures were performed with the RetroFlex delivery catheter followed by the RetroFlex II catheter incorporating a flexible nose cone and the Ascendra transapical catheter. The profile size of the transfemoral vascular sheath was 22-24 Fr. Two device sizes were available at the time of enrollment, the 23 mm device for annulus sizes ranging between 18-21.5 mm and the 26 mm device for annulus sizes from 21.5-24 mm. Technical details of the implant procedure have been described previously.11,12
Definitions. Technical success was defined as: (1) successful vascular access, delivery, and deployment of the device with final successful retrieval of the delivery system; and (2) correct position of the device in the proper anatomical location with adequate performance of the prosthetic heart valve (mean pressure gradient <20 mm Hg) and without use of multiple prostheses. Stroke was defined as rapid onset of a focal or global neurological deficit without presence of alternative causes, with a duration of >24 hours or available neuroimaging documenting a new hemorrhage or infarct. Myocardial infarction was defined as new ischemic symptoms or signs with elevated cardiac biomarkers (troponin and/or CK-MB). Major vascular complications were any thoracic aortic dissection, access-site or access-related vascular injury leading to either death, need for significant blood transfusions, unplanned percutaneous or surgical intervention, or irreversible end-organ damage.
Statistics. Categorical variables are presented as frequencies and percentages. Continuous variables are presented as mean ± standard deviation. Group differences were compared with the Kruskal-Wallis test as well as the two-tailed Wilcoxon rank sum test for the Kaplan Meier estimates. P-values <.05 were considered significant. Data were collected by web-based electronic data capture provided by the Institut für Herzinfarktforschung (IHF) at the Heart Center Ludwigshafen, Germany. All patients gave written informed consent before the procedure. The authors had full access to and take full responsibility for the integrity of the data.
Results
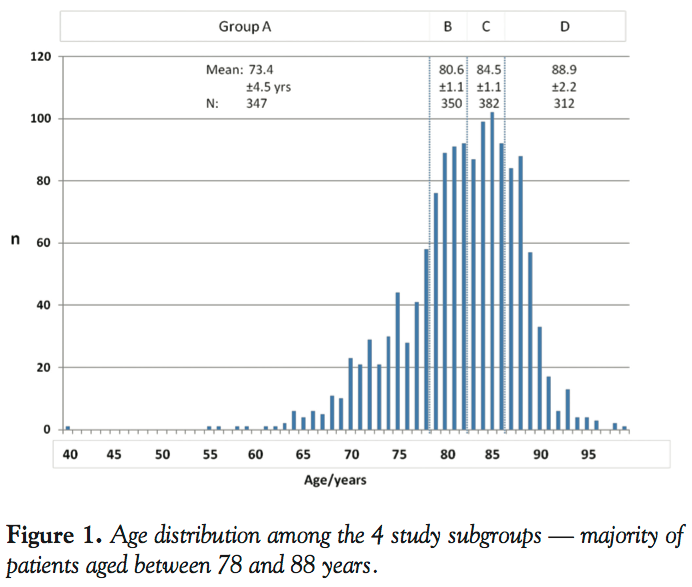 A total of 1386 consecutive patients undergoing TAVI for treatment of symptomatic aortic valve stenosis have been included in the present analysis and divided in the following groups: (1) group A, mean age 73.4 ± 4.5 years, range 40-78 years, n = 347 (24.9%); (2) group B, 80.6 ± 1.1 years, range 79-82 years, n = 350 (25.2%); (3) group C, 84.5 ± 1.1 years, range 83-86 years, n = 382 (27.5%); and (4) group D, 88.9 ± 2.2 years, range 87-99 years, n = 312 (22.4%) (Figure 1).
A total of 1386 consecutive patients undergoing TAVI for treatment of symptomatic aortic valve stenosis have been included in the present analysis and divided in the following groups: (1) group A, mean age 73.4 ± 4.5 years, range 40-78 years, n = 347 (24.9%); (2) group B, 80.6 ± 1.1 years, range 79-82 years, n = 350 (25.2%); (3) group C, 84.5 ± 1.1 years, range 83-86 years, n = 382 (27.5%); and (4) group D, 88.9 ± 2.2 years, range 87-99 years, n = 312 (22.4%) (Figure 1).
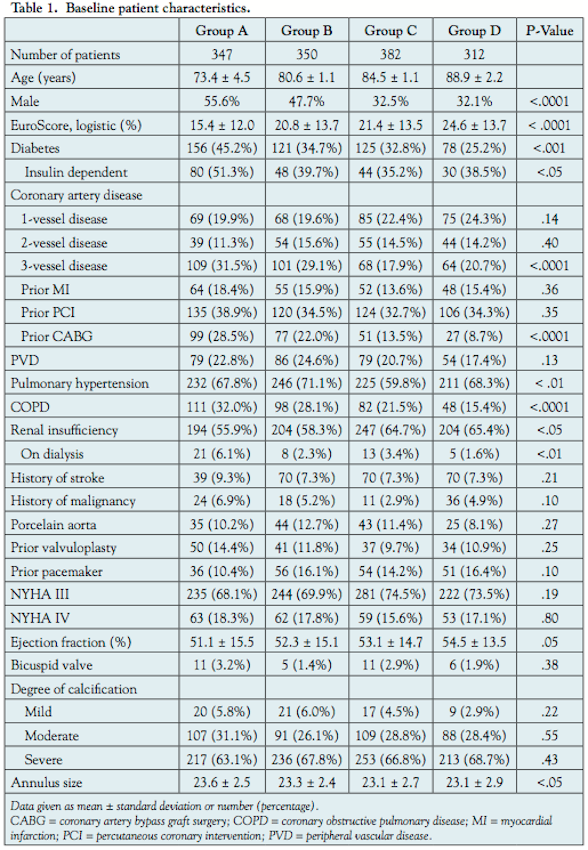 Patient baseline characteristics. Patient baseline characteristics are summarized in Table 1. The groups showed significant differences with respect to major co-morbidities which were more frequent in the younger patient population as compared to older patients: severe coronary artery disease, previous coronary artery bypass grafting (CABG), diabetes, insulin-requiring diabetes, chronic obstructive pulmonary disease (COPD), and renal failure requiring hemodialysis. Male gender was more prevalent in younger patients. There were no differences in terms of clinical symptoms prior to the procedure. Mean preprocedural aortic valve gradient was slightly higher in older patients and the aortic annulus was significantly smaller, but there were no differences in the calcification pattern. The logistic EuroScore was 15.4 ± 12.0% in the youngest population (group A), 20.8 ± 13.7% in group B, 21.4 ± 13.5% in group C, and 24.6 ± 13.7% in group D (P<.0001).
Patient baseline characteristics. Patient baseline characteristics are summarized in Table 1. The groups showed significant differences with respect to major co-morbidities which were more frequent in the younger patient population as compared to older patients: severe coronary artery disease, previous coronary artery bypass grafting (CABG), diabetes, insulin-requiring diabetes, chronic obstructive pulmonary disease (COPD), and renal failure requiring hemodialysis. Male gender was more prevalent in younger patients. There were no differences in terms of clinical symptoms prior to the procedure. Mean preprocedural aortic valve gradient was slightly higher in older patients and the aortic annulus was significantly smaller, but there were no differences in the calcification pattern. The logistic EuroScore was 15.4 ± 12.0% in the youngest population (group A), 20.8 ± 13.7% in group B, 21.4 ± 13.5% in group C, and 24.6 ± 13.7% in group D (P<.0001).
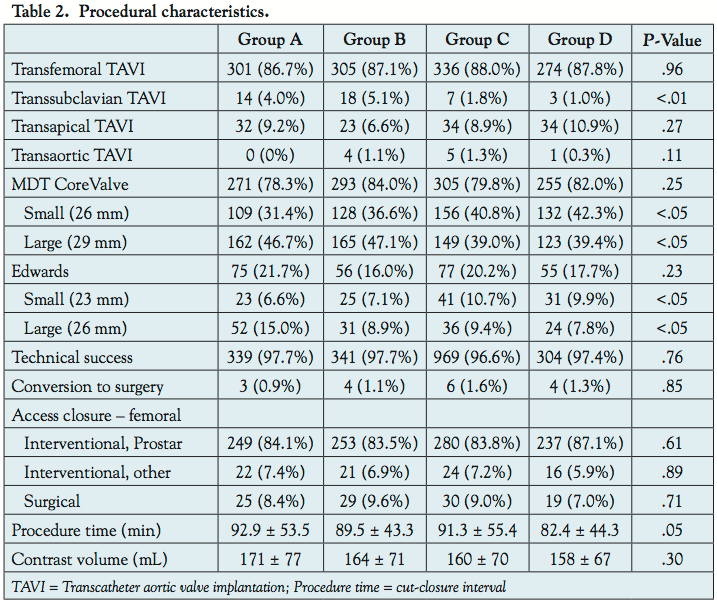 Procedural characteristics and outcome. Transfemoral access was used in 87%-88% of all cases, followed by transapical in 6%-11%, transsubclavian in 1%-5%, with a significantly higher utilization in groups A and B, and transaortic in patients >80 years old only in about 1% (P=NS). The CoreValve prosthesis was used in 78%-84%, the Edwards SAPIEN prosthesis in 16%-22% without differences between the study groups. Similarly, the technical success rate was almost equivalent in all 4 groups ranging between 96.6% and 97.7%. In addition, there were no differences in access closure methods (Table 2).
Procedural characteristics and outcome. Transfemoral access was used in 87%-88% of all cases, followed by transapical in 6%-11%, transsubclavian in 1%-5%, with a significantly higher utilization in groups A and B, and transaortic in patients >80 years old only in about 1% (P=NS). The CoreValve prosthesis was used in 78%-84%, the Edwards SAPIEN prosthesis in 16%-22% without differences between the study groups. Similarly, the technical success rate was almost equivalent in all 4 groups ranging between 96.6% and 97.7%. In addition, there were no differences in access closure methods (Table 2).
 Echocardiographic outcome. Implantation of the TAVI prostheses resulted in immediate and marked improvement of the hemodynamic valve status, significantly reducing the transvalvular mean gradient in all 4 study groups (Table 3). The overall preprocedural rate of severe aortic regurgitation was low, but significantly higher in younger patients (NYHA class III: group A 4.9% vs group D 1.3%, P<.01; NYHA class IV: group B 2.3% vs group C 0.3%, P<.05). Post procedure, there were no differences between the study groups with class III/IV regurgitation in only 1.2% to 1.9% of patients.
Echocardiographic outcome. Implantation of the TAVI prostheses resulted in immediate and marked improvement of the hemodynamic valve status, significantly reducing the transvalvular mean gradient in all 4 study groups (Table 3). The overall preprocedural rate of severe aortic regurgitation was low, but significantly higher in younger patients (NYHA class III: group A 4.9% vs group D 1.3%, P<.01; NYHA class IV: group B 2.3% vs group C 0.3%, P<.05). Post procedure, there were no differences between the study groups with class III/IV regurgitation in only 1.2% to 1.9% of patients.
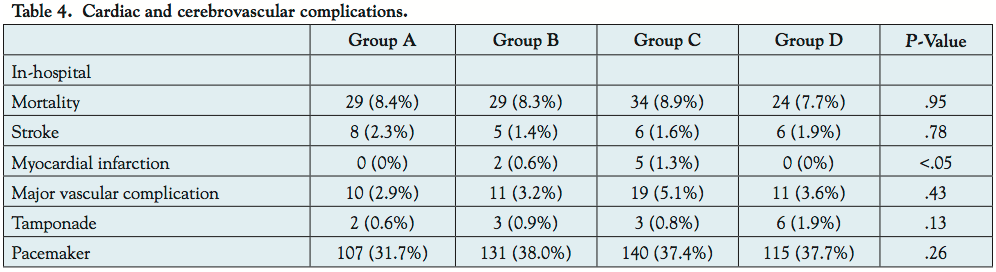 Clinical outcome. There were no differences in major cardiac or cerebrovascular event rates during the in-hospital and 30-day period between all 4 study groups except slightly more myocardial infarctions in group C (1.3%) (Table 4). Thirty-day all-cause mortality was 7.2% (A), 7.1% (B), 9.7% (C), and 8.7% (D) (P=NS) (Figure 2). Strokes occurred in 1.4%-2.3% of patients. The rates of major vascular complications were 2.9%-5.1%. Postprocedural pacemaker implantation was performed in 31.7% and 38.0% of patients.
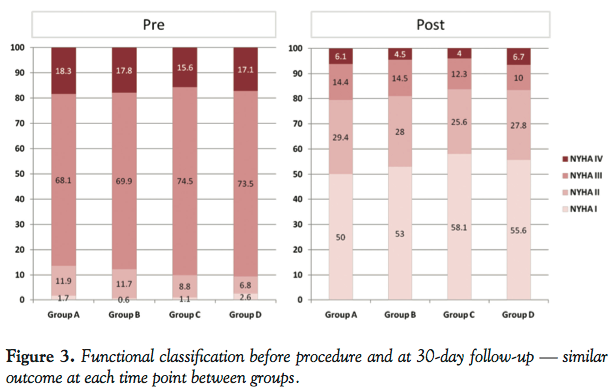
Clinical outcome. There were no differences in major cardiac or cerebrovascular event rates during the in-hospital and 30-day period between all 4 study groups except slightly more myocardial infarctions in group C (1.3%) (Table 4). Thirty-day all-cause mortality was 7.2% (A), 7.1% (B), 9.7% (C), and 8.7% (D) (P=NS) (Figure 2). Strokes occurred in 1.4%-2.3% of patients. The rates of major vascular complications were 2.9%-5.1%. Postprocedural pacemaker implantation was performed in 31.7% and 38.0% of patients. 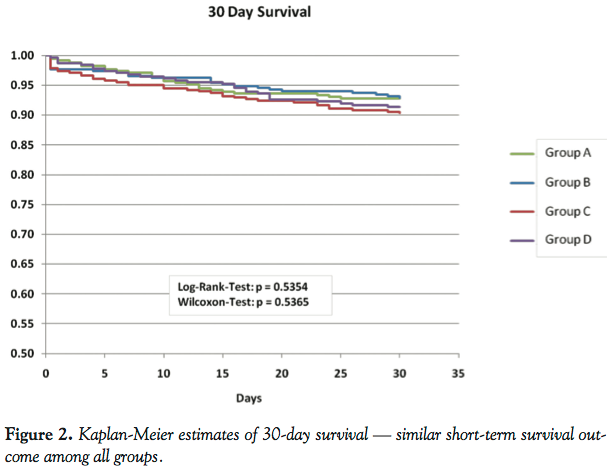 Postprocedural improvement of the functional patient status was remarkable and similar between the study groups with regard to NYHA classification. At 30 days, the majority of patients were in NYHA class I/II (Figure 2). Similarly, there was a pronounced improvement in all categories of the self-reported health status (EuroQol 5d) in all groups comparing pre- and postprocedural results. However, younger patients demonstrated a significantly better improvement in the categories ‘mobility’ and ability for ‘self-care’ compared to older patients.
Postprocedural improvement of the functional patient status was remarkable and similar between the study groups with regard to NYHA classification. At 30 days, the majority of patients were in NYHA class I/II (Figure 2). Similarly, there was a pronounced improvement in all categories of the self-reported health status (EuroQol 5d) in all groups comparing pre- and postprocedural results. However, younger patients demonstrated a significantly better improvement in the categories ‘mobility’ and ability for ‘self-care’ compared to older patients.
Discussion
 Although not a randomized control trial, this study provides important insights into the current practice of TAVI. Based on the German TAVI registry,9 these data on more than 1300 consecutive TAVI patients reflect real-world conditions and therefore, it forms a profound basis for the conducted analysis. As indication criteria for TAVI are fairly standardized, derived from the CE mark studies of both commercially available devices, the Medtronic CoreValve prosthesis and the Edwards SAPIEN prosthesis, overall patient characteristics in our study are comparable with previously reported studies and registries,3-7,11,12 with the majority of patients being octogenarians. However, it is unknown so far if there are relevant differences in patient characteristics and outcomes after TAVI in this very elderly population compared to younger patients. We therefore compared in our study 4 groups of patients stratified by age, which revealed several important findings. Firstly, younger patients presented with significantly more co-morbidities compared to older patients, which is not a surprising finding. In order to qualify for a TAVI procedure, the patient must be considered high risk for surgery. Age alone contributes already as a risk factor, so younger patients must have additional risk contributors in order to be eligible for the procedure with given standards. Interestingly, this substantially increased co-morbidity profile does not translate into a higher risk score, here the logistic EuroScore, which is caused by the high weight of age in this type of scoring system. Today we have growing evidence that age alone is not a strong risk predictor in patients undergoing either surgical aortic valve replacement or TAVI, but frailty and reduced functional status are, which questions both validity and value of the EuroScore in this setting.13,14
Although not a randomized control trial, this study provides important insights into the current practice of TAVI. Based on the German TAVI registry,9 these data on more than 1300 consecutive TAVI patients reflect real-world conditions and therefore, it forms a profound basis for the conducted analysis. As indication criteria for TAVI are fairly standardized, derived from the CE mark studies of both commercially available devices, the Medtronic CoreValve prosthesis and the Edwards SAPIEN prosthesis, overall patient characteristics in our study are comparable with previously reported studies and registries,3-7,11,12 with the majority of patients being octogenarians. However, it is unknown so far if there are relevant differences in patient characteristics and outcomes after TAVI in this very elderly population compared to younger patients. We therefore compared in our study 4 groups of patients stratified by age, which revealed several important findings. Firstly, younger patients presented with significantly more co-morbidities compared to older patients, which is not a surprising finding. In order to qualify for a TAVI procedure, the patient must be considered high risk for surgery. Age alone contributes already as a risk factor, so younger patients must have additional risk contributors in order to be eligible for the procedure with given standards. Interestingly, this substantially increased co-morbidity profile does not translate into a higher risk score, here the logistic EuroScore, which is caused by the high weight of age in this type of scoring system. Today we have growing evidence that age alone is not a strong risk predictor in patients undergoing either surgical aortic valve replacement or TAVI, but frailty and reduced functional status are, which questions both validity and value of the EuroScore in this setting.13,14
The technical success rate was similarly high in all groups (97%-98%), which is in line with recently reported series,3-6 and there were no relevant procedural differences with regard to type of devices used and access sites. Despite remarkable differences in baseline characteristics, the incidence of major adverse cardiac and cerebrovascular events in-hospital as well as at 30-day follow-up was identical in the study groups, with a 30-day all-cause mortality of 7%-10% in this high-risk patient population, which compares favorably relative to the spontaneous clinical course in untreated patients and is well in line with the most recent publications from experienced centers, reporting a 30-day mortality range of 4%-10%.4-6 Incidence of pacemaker implantations was fairly high in all groups, partially related to local non-restrictive implantation policies and lack of established guideline recommendations for this special subset of patients, and partially related to the high proportion of CoreValve implantations, which are known to be associated with a higher incidence of conduction abnormalities and need for permanent pacing. However, there are no randomized data thus far comparing both technologies regarding this aspect and there is certainly a need for further investigation and development of widely accepted and uniform criteria on pacemaker indications after TAVI procedures.
One of the most relevant findings of this analysis, however, is the effect of TAVI on functional patient status. Successful procedures result in a remarkable improvement of the functional status in both elderly and young patients. All 4 groups presented with the same NYHA characteristics prior to the procedure, with >85% being in NYHA class III/IV, and improved the same way afterward (>80% NYHA I/II). The quality of life assessment using the EuroQol score demonstrated a similar finding with substantial improvements in all categories in the study groups comparing pre- and postprocedure. However, this more detailed analysis revealed significant differences between younger and older patients with regard to the parameters ‘mobility’ and ‘self-care,’ showing a significantly better status in the younger population after the procedure. Therefore, TAVI significantly impacts on quality of life, which corroborates previously published data assessing quality of life up to 6 months post TAVI.15-17 But it is particularly the younger population that improves the most, although similarly limited beforehand. Therefore, younger populations have a higher net improvement than older populations, which are more likely to be affected by frailty, etc. In addition, this finding indicates that although presenting with a higher co-morbid risk profile, younger patients are similarly functionally affected by the valve disease as older patients with a lower co-morbidity profile.
Study limitations. This analysis is based on a non-randomized observational study. Since study populations showed substantial differences in baseline characteristics, this report is not suitable to assess the predictive value of age on procedural and clinical outcomes in patients undergoing TAVI. Further studies will address this issue by multivariate analyses. As the registry includes a considerable number of sites with young TAVI programs, it is likely that results will further improve with high procedural volumes. Only procedural and short-term clinical outcomes up to 30 days are reported, which is important to define device safety, but insufficient to delineate differences in efficacy profiles. All commonly used device and access types have been included. Since both were distributed evenly between the study groups, we did not perform subgroup analyses with regard to these parameters.
Conclusion
This study demonstrates that TAVI achieves similar results on safety and efficacy among different age populations with currently applied enrollment criteria. Younger patients undergoing TAVI have more co-morbidities than elderly patients, which is driven by the need of high-risk conditions to undergo a TAVI procedure. Both patient populations experience a substantial functional improvement after the procedure, which appears to be particularly pronounced in younger patients.
Acknowledgment. We would like to thank Mr Martin Horack of the Institut für Herzinfarktforschung, Germany, for his efforts and support of this study.
Appendix
Participating centers in order of enrolled patients. HELIOS Klinikum Siegburg: U. Gerckens, E. Grube, L. Buellesfeld (268); Universitätsklinikum Essen: H. Eggebrecht, R. Erbel (120); Herzzentrum Ludwigshafen: R. Zahn (98); Universität Leipzig Herzzentrum: A. Linke, G. Schuler (97); Cardio Vasculäres Centrum (CVC) Frankfurt Sankt Katharinen: H.Sievert (95); Universitätsklinikum Jena: H.R. Figulla (80); Asklepios Klinik St. Georg Hamburg: K.H. Kuck (70); Krankenhaus der barmherzigen Brüder Trier: K.E. Hauptmann (70); Städt. Klinikum München Klinik Bogenhausen: E. Hoffmann (70); Klinikum Links der Weser Bremen, R. Hambrecht (58); Universitätsklinikum Bonn, Med. Klinik und Poliklinik II: G. Nickenig (51); Segeberger Kliniken GmbH: G. Richardt (47); Augustinum Klinik München: M. Block (44); Elisabeth-Krankenhaus Essen: C.H. Naber (42); Herzzentrum Bad Krozingen: F.J. Neumann (28); Robert-Bosch-Krankenhaus, Stuttgart: U. Sechtem, M. Vöhringer (27); Unfallkrankenhaus Berlin: L. Bruch (25); Sana Herzzentrum Cottbus: A. Harnath (23); HELIOS Klinikum Wuppertal: H. Guelker (18); Krankenhaus München-Neuperlach: H. Mudra; Universitätsklinikum Rostock: Ch. Nienaber (18); Klinikum Schwabing, München: S. Sack (17); Klinikum Coburg: J. Brachmann (15); Städt. Kliniken Neuss Lukaskrankenhaus: M. Haude (4); Katharinenhospital Stuttgart: T. Nordt (2); Universitätsklinikum Regensburg: G. Riegger (2); Klinikum Traunstein: W. Moshage (1); Krankenhaus München – Neuperlach: H. Mudra (1).
References
- Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro heart survey on valvular heart disease. Eur Heart J. 2003;24(13):1231-1243.
- Vahanian A, Baumgartner H, Bax J, et al. Guidelines on the management of valvular heart disease: the task force on the management of valvular heart disease of the European Society of Cardiology. Eur Heart J. 2007;28(2):230-268.
- Piazza N, van Gameren M, Jüni P, et al. A comparison of patient characteristics and 30-day mortality outcomes after transcatheter aortic valve implantation and surgical aortic valve replacement for the treatment of aortic stenosis: a two-centre study. EuroIntervention. 2009;5(5):580-588.
- Thomas M, Schymik G, Walther T, et al. Thirty-day results of the SAPIEN aortic bioprosthesis European outcome (SOURCE) registry. A European registry of transcatheter aortic valve implantation using the Edwards SAPIEN valve. Circulation. 2010;122(1):62-69.
- Rodés-Cabau J, Webb JG, Cheung A, et al. Transcatheter aortic valve implantation for the treatment of severe symptomatic aortic stenosis in patients at very high or prohibitive surgical risk: acute and late outcomes of the multicenter Canadian experience. J Am Coll Cardiol. 2010;55(11):1080-1090.
- Tamburino C, Capodanno D, Ramondo A, et al. Incidence and predictors of early and late mortality after transcatheter aortic valve implantation in 663 patients with severe aortic stenosis. Circulation. 2011;123(3):299-308.
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-2198.
- Zahn R, Gerckens U, Grube E, et al. Transcatheter aortic valve implantation: first results from a multi-centre real-world registry. Eur Heart J. 2011;32(2):198-204.
- Kind P. The EuroQol instrument: an index of health-related quality of life. Quality of life and pharmaco-economics in clinical trials. Second edition. Spiker B, ed. Lippincott-Raven Publishers. Philadelphia 1996.
- Grube E, Buellesfeld L, Mueller R, et al. Progress and current status of percutaneous aortic valve replacement: results of three device generations of the corevalve revalving system. Circ Cardiovasc Interv. 2008;1(3):167-175.
- Webb JG, Pasupati S, Humphries K, et al. Percutaneous transarterial aortic valve replacement in selected high-risk patients with aortic stenosis. Circulation. 2007;116(7):755-763.
- Buellesfeld L, Wenaweser P, Gerckens U, et al. Transcatheter aortic valve implantation: predictors of procedural success — the Siegburg-Bern experience. Eur Heart J. 2010;31(8):984-991.
- ElBardissi AW, Shekar P, Couper GS, Cohn LH. Minimally invasive aortic valve replacement in octogenarian, high-risk, transcatheter aortic valve implantation candidates. J Thorac Cardiovasc Surg. 2011;141(2):328-335.
- Bekeredjian R, Krumsdorf U, Chorianopoulos E, et al. Usefulness of percutaneous aortic valve implantation to improve quality of life in patients >80 years of age. Am J Cardiol. 2010;106(12):1777-1781.
- Krane M, Deutsch MA, Bleiziffer S, et al. Quality of life among patients undergoing transcatheter aortic valve implantation. Am Heart J. 2010;160(3):451-457.
- Gotzmann M, Hehen T, Germing A, et al. Short-term effects of transcatheter aortic valve implantation on neurohormonal activation, quality of life and 6-minute walk test in severe and symptomatic aortic stenosis. Heart. 2010;96(14):1102-1106.
________________________________________________________
*Joint first authors.
From 1Bern University Hospital, Switzerland, 2St Petrus Hospital Bonn, Germany, 3University Hospital Essen, Germany, 4Heart Center Ludwigshafen, Germany, 5University Hospital Leipzig, Germany, 6Cardiovascular Center Frankfurt, Germany, 7University Hospital Jena, Germany, 8Asklepios Klinik St Georg, Department of Cardiology, Hamburg, Germany, 9Krankenhaus der Barmherzigen Brüder Trier, Germany, 10Heart Center Bremen, Germany, 11Abteilung für Kardiologie, Segeberger Kliniken, Bad Segeberg, Germany, 12International Heart Center Rhein-Ruhr, Essen, Germany, 13Robert-Bosch-Krankenhaus, Stuttgart, Germany, 14Hospital Munich-Neuperlach, Germany, 15Institut für Herzinfarktforschung, Ludwigshafen, Germany, and 16Bonn University Hospital, Germany.
Funding: The study was funded by the Institut für Herzinfarktforschung, Germany.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. LB, UG, EG, AL, and HS worked as trainers or proctors for either Medtronic or Edwards or both and received speaker honoraria. HRF is co-founder and co-inventor of JenaValve technology, as well as medical advisor to JenaValve technology, HS is a member of the scientific advisory board of JenaValve technology. The other authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 2, 2012, provisional acceptance given April 30, 2012, final version accepted May 30, 2012.
Address for correspondence: Lutz Buellesfeld, MD, Department of Cardiology, Bern University Hospital , CH-3010 Bern, Switzerland. Email: Lutz.Buellesfeld@insel.ch

