

Acquired (Post-Angioplasty) Coronary Ventricular Fistula Draining into Left Ventricle Aneurysm
ABSTRACT: Coronary artery fistula is a rare condition where a fistulous communication exists between the coronary artery and a cardiac chamber or vein. Mostly they are of congenital origin, but rarely may be acquired due to trauma, post cardiac surgery or angioplasty, or very rarely, because of coronary aneurysm rupture. Ours is an interesting case of a post-coronary artery bypass graft surgery status with a fistula in second obtuse marginal branch of left circumflex coronary artery draining into left ventricle aneurysm. We explore possible causes including erosion of the thin aneurysmal wall into coronary lumen. Given the history of previous surgical revascularization, it may be a contained rupture and the possibility of pulsatile effect of the obtuse marginal branch eroding into the thin wall aneurysm is considered.
J INVASIVE CARDIOL 2012;24(5):E99-E100
______________________________________________
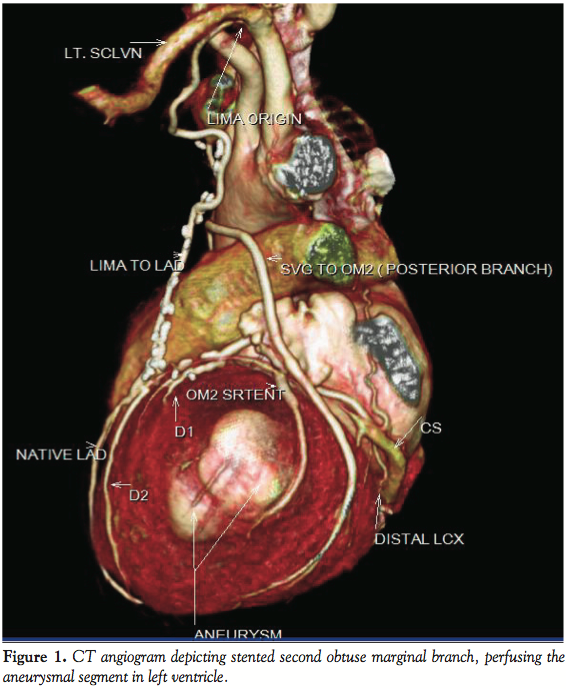 Case Report. A 65-year-old male patient presented with dyspnea on minimal exertion, New York Heart Association (NYHA) class III from 4 months. He was a known hypertensive, non-diabetic and suffered anterior wall myocardial infarction in 1998. Coronary angiography showed double vessel disease in 1998 [left anterior descending coronary artery (LAD) mid 100% stenosis and second obtuse marginal (OM2) 95%]. Subsequently patient underwent coronary artery bypass grafting with a left internal mammary artery graft to the LAD and saphenous venous graft to OM2. In 2007 he developed unstable angina and underwent percutaneous transluminal coronary angioplasty with stent to native OM2. Two-dimensional echocardiogram showed regional wall motion abnormality in LAD and left circumflex coronary artery territory with left ventricle (LV) ejection fraction of 25% with LV aneurysm in lateral wall. Now with complaints of dyspnea on exertion NYHA 2, he was again taken up for coronary angiogram that showed mid LAD 100% stenosis, mild plaquing in right coronary artery, and left circumflex coronary artery showed distal 50% plaque with patent stent in OM2 and complete occlusion of OM2 branch that was grafted in 1998. There was a coronary artery fistula distally in OM2 draining to LV aneurysm (Figure 1). Stress thallium was done that showed non-significant reversible myocardial ischemic deficit in LAD territory. Patient was advised medical management as this fistula was unlikely to result in significant myocardial overload to justify percutaneous closure. Review of older angiograms did not show its presence until 2007 from most recent angiogram. CT angiogram clearly showed a fistula arising from OM2 and draining into LV aneurysm in the lateral wall (Figure 2).
Case Report. A 65-year-old male patient presented with dyspnea on minimal exertion, New York Heart Association (NYHA) class III from 4 months. He was a known hypertensive, non-diabetic and suffered anterior wall myocardial infarction in 1998. Coronary angiography showed double vessel disease in 1998 [left anterior descending coronary artery (LAD) mid 100% stenosis and second obtuse marginal (OM2) 95%]. Subsequently patient underwent coronary artery bypass grafting with a left internal mammary artery graft to the LAD and saphenous venous graft to OM2. In 2007 he developed unstable angina and underwent percutaneous transluminal coronary angioplasty with stent to native OM2. Two-dimensional echocardiogram showed regional wall motion abnormality in LAD and left circumflex coronary artery territory with left ventricle (LV) ejection fraction of 25% with LV aneurysm in lateral wall. Now with complaints of dyspnea on exertion NYHA 2, he was again taken up for coronary angiogram that showed mid LAD 100% stenosis, mild plaquing in right coronary artery, and left circumflex coronary artery showed distal 50% plaque with patent stent in OM2 and complete occlusion of OM2 branch that was grafted in 1998. There was a coronary artery fistula distally in OM2 draining to LV aneurysm (Figure 1). Stress thallium was done that showed non-significant reversible myocardial ischemic deficit in LAD territory. Patient was advised medical management as this fistula was unlikely to result in significant myocardial overload to justify percutaneous closure. Review of older angiograms did not show its presence until 2007 from most recent angiogram. CT angiogram clearly showed a fistula arising from OM2 and draining into LV aneurysm in the lateral wall (Figure 2).
 Discussion. Numerous case reports and reviews have been published on coronary artery fistulas and the majority are of congenital origin. Acquired coronary artery communications to LV cavity are extremely rare and are usually due to accidental or iatrogenic trauma. Our case befits the acquired category, as the fistula was not present in serial angiograms in 1998 and 2007. There have been case reports of coronary fistulas developing post myocardial infarction1 that may be related to adverse ventricular remodelling.2 Very rare case reports have been published where these fistulas developed post coronary angioplasty.3,4 The draining of fistula at the site of LV aneurysm underlines the possible mechanism of its formation. Destruction of the myocardium may have exposed microcapillaries in the subendocardium to the LV cavity and improved blood flow post-stenting in this area may have hastened the whole process.5 To our knowledge this is an extremely rare case where coronary angioplasty and stenting in the coronary artery has precipitated the formation of coronary artery fistula in the respective territory.
Discussion. Numerous case reports and reviews have been published on coronary artery fistulas and the majority are of congenital origin. Acquired coronary artery communications to LV cavity are extremely rare and are usually due to accidental or iatrogenic trauma. Our case befits the acquired category, as the fistula was not present in serial angiograms in 1998 and 2007. There have been case reports of coronary fistulas developing post myocardial infarction1 that may be related to adverse ventricular remodelling.2 Very rare case reports have been published where these fistulas developed post coronary angioplasty.3,4 The draining of fistula at the site of LV aneurysm underlines the possible mechanism of its formation. Destruction of the myocardium may have exposed microcapillaries in the subendocardium to the LV cavity and improved blood flow post-stenting in this area may have hastened the whole process.5 To our knowledge this is an extremely rare case where coronary angioplasty and stenting in the coronary artery has precipitated the formation of coronary artery fistula in the respective territory.
References
- Said SA, van der Werf T. Acquired coronary cameral fistulas: are these collaterals losing their destination? Clin Cardiol. 1999;22(4):297-302.
- Nugue O, Decoulx E, Millaire A, Leroy O, Beuscart C, Ducloux G. Coronary-left ventricular fistula in post-infarction of the myocardium. Apropos of a new case. Review of the literature [in French]. Ann Cardiol Angeiol (Paris). 1994;43(2):55-61.
- Lipiec P, Peruga JZ, Krzemińska-Pakula M, Foryś J, Drozdz J, Kasprzak JD. Right coronary artery-to-right ventricle fistula complicating percutaneous transluminal angioplasty: case report and review of the literature. J Am Soc Echocardiogr. 2004;17(3):280-283.
- Hur SH, Han SW, Won KS. Coronary artery-left ventricle fistula after PTCA: diagnosed by contrast echocardiography. J Invasive Cardiol. 2003;15(12):729-731.
- Schanzenbächer P, Bauersachs J . Acquired right coronary artery fistula draining to the right ventricle: angiographic documentation of first appearance following reperfusion after acute myocardial infarction, with subsequent spontaneous closure. Heart. 2003;89(8):e22.
______________________________________________
From the Department of Cardiology at Mukat Hospital, Ludhiana (Punjab), India,1 41003.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 16, 2011, provisional acceptance given November 22, 2011, final version accepted December 22, 2011.
Address for correspondence: Dr Amit Gupta, Consultant and Interventional Cardiologist, Department of Cardiology, SPS Apollo Hospital, Sherpur Chowk, Ludhiana (Punjab), India, 141003. Email: docamitgupta@yahoo.co.in

