

30-Day Outcome After Percutaneous Coronary Angioplasty in Nonagenarians: Feasibility and Specific Considerations in Different Clinical Settings
Abstract: Background. Nonagenarians have been systematically excluded from randomized trials dealing with invasive coronary strategies, resulting in a lack of evidence-based guidelines regarding the optimal approach in this population. Aim. To describe the clinical and procedural characteristics and outcomes of patients 90 years of age or older who were treated with percutaneous coronary interventions (PCI). Methods. We evaluated the 30-day outcomes of patients 90 years or older who underwent PCI at our institution, comparing the ST-segment elevation myocardial infarction (STEMI) subgroup with the non-STEMI/unstable angina (UA) and stable angina (SA) subgroups, who had been referred for coronary angiography. Results. Over the time period 2002-2011, we identified 45 nonagenarians (mean age, 93 years; range, 90-102 years). The majority (59%) presented with an acute coronary syndrome and underwent immediate coronary revascularization by PCI. Technical success rate was 90%. The frequency of in-hospital death, need for urgent coronary artery bypass surgery, periprocedural cerebrovascular accident, and major adverse cardiovascular and cerebral events was 11%, 4.5%, 4.5%, and 18%, respectively. At 30 days, mortality was exclusively related to the STEMI subgroup with hemodynamic instability, compared with the non STEMI/UA and SA population. Conclusions. In carefully selected nonagenarians, PCI in contemporary practice may be performed with a high technical success rate with relatively low morbidity and mortality. Questions are raised about the feasibility and outcome of invasive coronary strategies in the high-risk clinical subgroup of STEMI and hemodynamic instability.
J INVASIVE CARDIOL 2011;23(12):521-524
Key words: nonagenarian angioplasty, geriatric PCI
_____________________________________________
The fact that very elderly patients have been excluded from randomized trials dealing with invasive coronary strategies has resulted in lack of evidence regarding the best approach for this specific cohort. The subgroup presenting with acute coronary syndromes (ACS) represents a continuously growing population with the highest risk for complications and death. On the other hand, they are the patients who may have better absolute benefit from reperfusion treatments when compared with younger patients.1
Increased age is an important determinant of outcome after percutaneous revascularization; however, progress in technology, interventional techniques, and adjunctive medical therapies have resulted in improvement in procedural and overall outcomes.2-4
Recently, PCI in octogenarians has become increasingly common, and in selected patients, in-hospital outcome is comparable to younger patients.5,6 As these trends continue, PCI is being performed in a small but increasing number of nonagenarians; however, there is a paucity of outcomes data in this population, limited to case reports and small series.7-10
In light of these facts, we sought to describe the clinical, angiographic, procedural characteristics, and outcomes of patients aged 90 years or older who were treated with PCI at our institution during the period of 2002-2011. We focused especially on the in-hospital and 30-day outcomes, with special attention on the subgroup presenting with ST-segment elevation myocardial infarction (STEMI), comparing it with the more “stable” population, i.e., non-STEMI/unstable angina (UA) and stable angina (SA) cohorts, who had been referred electively to coronary angiography.
Methods
 Study population. Approval for the present study was obtained from the Institutional Review Board. Inclusion criteria were all comers aged 90 years or older at the time of the index PCI, who had undergone the procedure after 2002 and consented to the use of their medical records for research. During the study period, 6600 interventional procedures were performed, 45 (0.7%) of which involved patients ≥90 years old, representing the study population.
Study population. Approval for the present study was obtained from the Institutional Review Board. Inclusion criteria were all comers aged 90 years or older at the time of the index PCI, who had undergone the procedure after 2002 and consented to the use of their medical records for research. During the study period, 6600 interventional procedures were performed, 45 (0.7%) of which involved patients ≥90 years old, representing the study population.
Definitions. Major adverse cardiovascular and cerebrovascular events (MACCE) were defined as one or more of the following: 1) in-hospital death; 2) Q-wave myocardial infarction (MI); 3) urgent or emergent coronary artery bypass grafting (CABG) during index hospitalization; and 4) cerebrovascular accident (CVA) defined as transient ischemic attack (TIA) or stroke. MI was diagnosed in the presence of 2 of the following 3 criteria: 1) typical chest pain for at least 20 minutes; 2) elevation of creatine kinase (or the MB fraction) >2x normal; and/or 3) new Q-waves in the electrocardiogram. In recent years, elevated TnI has become the standard for the diagnosis of MI. In-hospital death included all deaths during the index hospital admission. Procedural success was defined as a residual lumen diameter stenosis ≤20% at the treated segment (culprit lesion), without in-hospital death, Q-wave MI, or need for urgent CABG. 30-day outcome included all-cause mortality, any MI, and the composite endpoint of death, MI, or target lesion revascularization (TLR). We also included in the analysis other procedural complications, such as those related to the vascular access site and acute renal failure. Shock was defined as prolonged systolic blood pressure <90 mm Hg in patients not on inotropes or intra-aortic balloon pump (IABP) support or <110 mm Hg in patients requiring treatment with inotropes or IABP support.
Statistical analysis. Continuous variables are summarized as mean ± standard deviation, and discrete variables are presented as frequency (percentages). Student’s t-test or the U-test were used for continuous variables between two groups. Categorical variables were compared using the Chi-square test or Fisher exact test. P≤.05 was considered significant.
Results
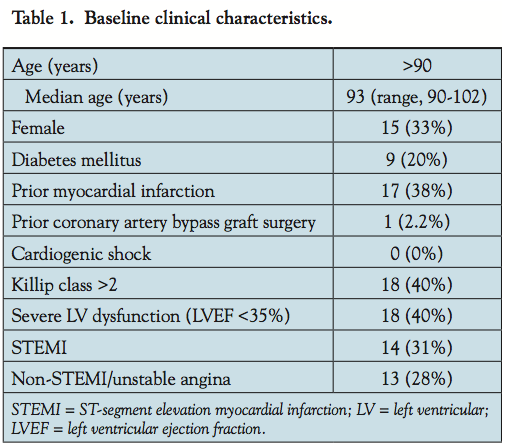 Baseline characteristics. The clinical characteristics of the 45 patients included in the analysis are summarized in Table 1. The patients were predominantly men, and the majority presented with an acute coronary syndrome. The median age was 93 years (range, 90-102 years). A past history of previous MI, Killip class >2 at admission, and severe LV dysfunction were frequently present. Related comorbidities of this advanced age group were: severe aortic stenosis present in 4 patients (9%); chronic renal failure in 8 patients (18%); severe
Baseline characteristics. The clinical characteristics of the 45 patients included in the analysis are summarized in Table 1. The patients were predominantly men, and the majority presented with an acute coronary syndrome. The median age was 93 years (range, 90-102 years). A past history of previous MI, Killip class >2 at admission, and severe LV dysfunction were frequently present. Related comorbidities of this advanced age group were: severe aortic stenosis present in 4 patients (9%); chronic renal failure in 8 patients (18%); severe 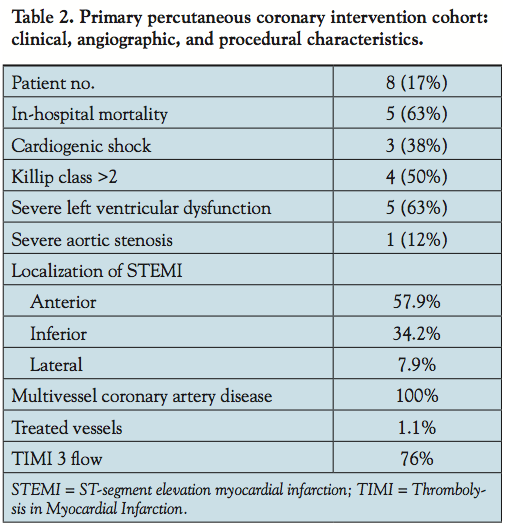 peripheral artery disease in 4 patients (9%); 1 patient with significant carotid artery stenosis; 3 patients after CVA; and 1 patient with renal cell carcinoma. The primary PCI (PPCI) subgroup comprises 8 patients (18%) who were admitted with STEMI (Table 2). In this subgroup, 3 patients (38%) presented with severe hemodynamic instability in cardiogenic shock and 4 additional patients (50%) were in Killip class >2. One patient who underwent PPCI also had severe aortic stenosis. The majority of the STEMI were localized at the anterior wall (57.9%), the entire cohort showed multivessel coronary artery disease, and TIMI 3 flow was achieved in 76% of this subgroup.
peripheral artery disease in 4 patients (9%); 1 patient with significant carotid artery stenosis; 3 patients after CVA; and 1 patient with renal cell carcinoma. The primary PCI (PPCI) subgroup comprises 8 patients (18%) who were admitted with STEMI (Table 2). In this subgroup, 3 patients (38%) presented with severe hemodynamic instability in cardiogenic shock and 4 additional patients (50%) were in Killip class >2. One patient who underwent PPCI also had severe aortic stenosis. The majority of the STEMI were localized at the anterior wall (57.9%), the entire cohort showed multivessel coronary artery disease, and TIMI 3 flow was achieved in 76% of this subgroup.
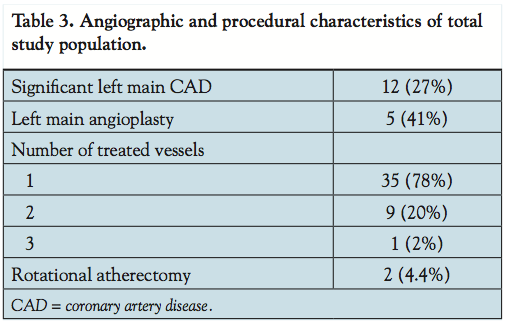 Angiographic and procedural characteristics. Table 3 summarizes the angiographic and procedural characteristics of the entire study population. The majority of patients (59%) underwent urgent revascularization at the time of presentation; elective PCI was performed in 41% of the cohort. Multivessel disease was present in the entire study population, with American College of Cardiology/American Heart Association type B2 or C culprit lesions. Significant left main coronary artery (LMCA) disease was present in 27%, in the vast majority of cases only one vessel was treated (78%), and 2 patients (4.4%) needed rotational atherectomy as the interventional strategy. Despite lesion complexity, overall procedural success was 90%.
Angiographic and procedural characteristics. Table 3 summarizes the angiographic and procedural characteristics of the entire study population. The majority of patients (59%) underwent urgent revascularization at the time of presentation; elective PCI was performed in 41% of the cohort. Multivessel disease was present in the entire study population, with American College of Cardiology/American Heart Association type B2 or C culprit lesions. Significant left main coronary artery (LMCA) disease was present in 27%, in the vast majority of cases only one vessel was treated (78%), and 2 patients (4.4%) needed rotational atherectomy as the interventional strategy. Despite lesion complexity, overall procedural success was 90%.
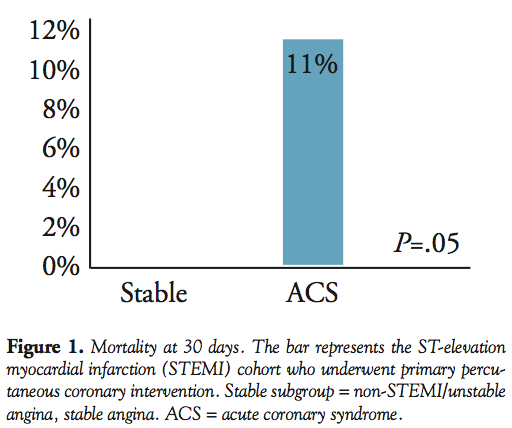
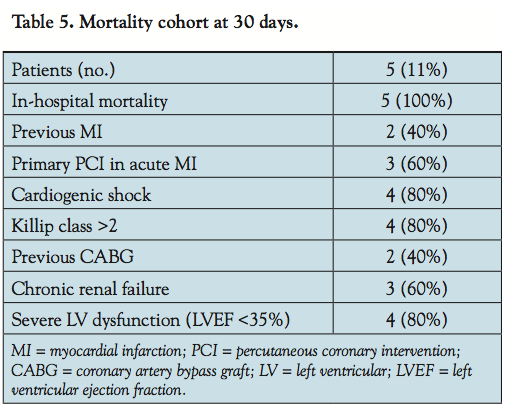
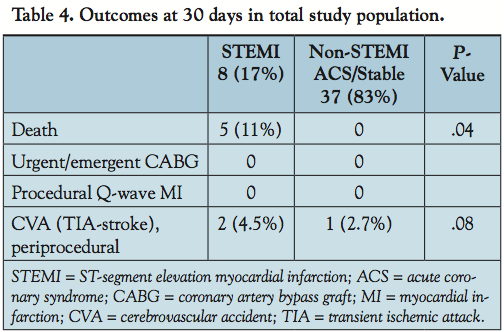 Table 5 summarizes the mortality cohort. Overall, 5 patients (11%) died, all of which occurred in-hospital in the PPCI subgroup compared with the non-STEMI/UA or SA subgroup. A systematic review of the database comparing these two groups, showed that at 30 days there was no further mortality among survivors. Focusing on the PPCI subgroup (8 patients), 5 patients died, all of whom presented with severe hemodynamic instability. In this high-risk group, accounting for the mortality in this cohort, 80% were in cardiogenic shock at presentation supported by intra-aortic balloon counterpulsation, 40% had previous CABG, 60% showed chronic renal failure and 80% severe left ventricular dysfunction (LVEF <35%). In-hospital major complications were major bleeding according to the TIMI bleeding scale11 in 2 patients (25%) and acute renal failure in 1 patient (12.5%), and occurred only in the PPCI subgroup.
Table 5 summarizes the mortality cohort. Overall, 5 patients (11%) died, all of which occurred in-hospital in the PPCI subgroup compared with the non-STEMI/UA or SA subgroup. A systematic review of the database comparing these two groups, showed that at 30 days there was no further mortality among survivors. Focusing on the PPCI subgroup (8 patients), 5 patients died, all of whom presented with severe hemodynamic instability. In this high-risk group, accounting for the mortality in this cohort, 80% were in cardiogenic shock at presentation supported by intra-aortic balloon counterpulsation, 40% had previous CABG, 60% showed chronic renal failure and 80% severe left ventricular dysfunction (LVEF <35%). In-hospital major complications were major bleeding according to the TIMI bleeding scale11 in 2 patients (25%) and acute renal failure in 1 patient (12.5%), and occurred only in the PPCI subgroup.
Discussion
 The major findings of the present study are: 1) in nonagenarians, PCI is frequently performed for an acute coronary syndrome presenting with complex lesion morphology; 2) despite this fact, the technical success rate was high; 3) mortality was in-hospital and related to the high-risk cohort, specifically in the PPCI subgroup presenting in cardiogenic shock and severe left ventricular dysfunction; 4) the PPCI subgroup showed acceptable rates of major bleeding and acute renal failure; and 5) patients in Killip class 1 at admission and final TIMI 3 flow at the end of the procedure had a high survival rate.
The major findings of the present study are: 1) in nonagenarians, PCI is frequently performed for an acute coronary syndrome presenting with complex lesion morphology; 2) despite this fact, the technical success rate was high; 3) mortality was in-hospital and related to the high-risk cohort, specifically in the PPCI subgroup presenting in cardiogenic shock and severe left ventricular dysfunction; 4) the PPCI subgroup showed acceptable rates of major bleeding and acute renal failure; and 5) patients in Killip class 1 at admission and final TIMI 3 flow at the end of the procedure had a high survival rate.
Our study is limited to 30-day follow-up in order to evaluate specifically the benefit of the invasive strategy in this population. After this time period, the outcome could be strongly influenced by different comorbidities frequently present in this cohort, i.e., severe aortic stenosis, malignancies, cerebrovascular disease, and chronic renal failure, making the analysis more difficult.
Although nonagenarians represent a small subset of patients in contemporary practice, there has been an exponential rise in the number of patients in recent years.12 It is a global trend and is likely to continue with the aging population.
This is reflected in the data from the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the American College of Cardiology/American Heart Association Guidelines) registry on the outcomes of 5000 nonagenarians treated for non-ST elevation ACS.13 The authors report that these patients have high in-hospital mortality (12%), but outcomes were better among those patients treated by guideline-recommended care, which in the case of ACS involves an invasive strategy.
In a study by Holmes et al,14 the investigators noted improvement in procedural success rates over time, likely due to advances in technique, operator experience, and adjunctive therapy, with a significant reduction of in-hospital mortality and MACE rates.
As reported in previous studies,6,7 PCI in nonagenarians is frequently performed in the setting of an ACS. The culprit lesions have complex morphology, with type C lesions in two-thirds of patients. However, despite these high-risk characteristics, the in-hospital mortality (6%) and MACE (9%) rates were not prohibitively high.
In our study, the mortality was exclusively in-hospital, in those patients with STEMI compared with those with non-ST elevation ACS or stable angina pectoris.
Bridges et al15 recently published the experience from the Society of Thoracic Surgeons national database of outcomes after cardiac surgery for coronary artery disease and valvular heart disease in over 1000 nonagenarians. They concluded that while surgical mortality increased with age, reasonable outcomes could be achieved with careful selection of patients. However, the operative mortality for CABG was high at 11.8% and frequency of stroke was 2.9%.
Finally, this study may raise the question of the feasibility and outcome of PPCI in nonagenarians presenting with STEMI and cardiogenic shock. At this time, careful patient selection for invasive strategies is recommended as the procedural outcome appears to be poor in this high-risk population.
Study limitations. This is a retrospective single-center analysis and is subject to the limitations of such a study. It is difficult to determine the relative importance of different operators’ skills, improvement in technology, improved antiplatelets and other adjunctive therapy, and the use of new stents that have developed during the time frame of the data collection. Furthermore, we focused on the 30-day outcomes of the PCI population, and cannot comment on the mid- and long-term follow-up or on the outcomes of patients treated medically or those undergoing surgical revascularization. Indeed, data from the CRUSADE registry confirm that coronary revascularization is performed in only a minority (12.6%) of nonagenarians presenting with non-ST segment elevation ACS. Due to the retrospective design of the CRUSADE data, it is not possible to define why certain patients had been selected for PCI over others. They appear to represent a small proportion of all nonagenarians presenting with an ACS, and it is likely that the absence of comorbidities represents a major factor that determines selection for revascularization.
Conclusion
Our study demonstrates that advanced age alone must not be a contraindication for performing coronary angiography and PCI when clear indication is present. Nonagenarians presenting with high-risk clinical situations represent a challenge, and careful selection appears to be pivotal. Further research efforts are required to characterize which nonagenarians would benefit from revascularization, and to some extent this requires the development of methods to quantify fitness and frailty16 in the elderly.
References
- Centers for Disease Control and Prevention. Trends in aging — United States and Worldwide. MMWR Morb Mortal Wkly Rep. 2003;52:101-104.
- Singh M, Rihal CS, Gersh BJ, et al. Twenty-five-year trend in in-hospital and long term outcome after percutaneous intervention: a single-institution experience. Circulation. 2007;115(22):2835-2841.
- Singh M, Rihal CS, Lennon RJ, Garrat KN, Mathew V, Holmes Jr DR. Prediction of complications following nonemergency percutaneous coronary interventions. Am J Cardiol. 2005;96(7):907-912.
- Batchelor WB, Anstrom KJ, Muhlbaier LH, et al. Contemporary outcome trends in the elderly undergoing percutaneous coronary interventions: results in 7472 octogenarians. National Cardiovascular Network Collaboration. J Am Coll Cardiol. 2000;36(3):723-730.
- Halon DA, Adawi S, Dobrecky-Meri I, Lewis BS. Importance of increasing age on presentation and outcome of acute coronary syndromes in elderly patients. J Am Coll Cardiol. 2004;43(3):346-352.
- Thompson RC, Holmes Jr DR, Gersh BJ, Mock MB, Bailey KR. Percutaneous transluminal coronary angioplasty in the elderly: early and long term results. J Am Coll Cardiol. 1991;17(6):1245-1250.
- Gowda RM, Chamakura SR, Khan IA, Vasavada BC, Sacchi TJ. Percutaneous coronary intervention in a nonagenarian woman for intractable post-infarction angina. Int J Cardiol. 2004;93(1):77-78.
- Moreno R, Salazar A, Banuelos C, et al. Effectiveness of percutaneous coronary interventions in nonagenarians. Am J Cardiol. 2004;94(8):1058-1060.
- Teplitsky I, Assali A, Lev E, Brosh D, Vaknin-Assa H, Kornowsky R. Results of coronary interventions in patients ≥90 years of age. Catheter Cardiovasc Interv. 2007;70(7):937-943.
- Wu Y, Hou C, Chou Y, Tsa C. Percutaneous coronary interventions in nonagenarians. Acta Cardiol. 2004;20:73-82.
- Rao SV, O’Grady K, Granger CV, et al. A comparison of the clinical impact of bleeding measured by two different classifications among patients with acute coronary syndromes. J Am Coll Cardiol. 2006;47(4):809-816.
- From AM, Rihal CS, Lennon RJ, Holmes Jr DR, Prasad A. Temporal trends and improved outcomes of percutaneous coronary revascularization in nonagenarians. J Am Coll Cardiol. 2008;1(6):692-698.
- Skolnick AH, Alexander KP, Chen AY, et al. Characteristics, management and outcomes of 5557 patients age ≥90 years with acute coronary syndromes: results from the CRUSADE initiative. J Am Coll Cardiol. 2007;49(17):1790-1797.
- Cohen HA, Williams DO, Holmes Jr DR. Impact of age on procedural and 1-year outcome in percutaneous transluminal coronary angioplasty: a report from the NHLBI Dynamic Registry. Am Heart J. 2003;146(3):513-519.
- Bridges CR, Edwards FH, Peterson ED, Coombs LP, Ferguson TB. Cardiac surgery in nonagenarians and centenarians J Am Coll Surg. 2003;197(3):347-356, discussion 356-357.
- Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489-495.
_____________________________________________
From the Cardiology Division, Interventional Cardiology Unit, Assaf Harofeh Medical Center, Tel-Aviv University, Sackler School of Medicine, Zerifin, Israel.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted July 28, 2011, provisional acceptance given August 17, 2011, final version accepted September 7, 2011.
Address for correspondence: Alberto Hendler, MD, FESC, Assaf Harofeh Medical Center, Cardiology Division, Zerifin, Israel. Email: ahendler@asaf.health.gov.il
