


Protective Techniques in Image-Guided Percutaneous Hepatic Ablations
Abstract: Image-guided percutaneous thermal ablation has become an important tool of the interventionalist for the treatment of patients with hepatic malignancies. This technique has been demonstrated to be safe and effective in most instances, with complication rates of less than 8%. The occurrence of major complications is most likely in situations where hepatic tumors are adjacent to organs such as the gallbladder, bowel, stomach, duodenum, kidney, and diaphragm. In order to reduce complications and expand the indication of percutaneous ablations of challenging hepatic lesions, several thermal protection techniques such as hydrodissection, carbon dioxide pneumodissection, balloon interposition, and chilled dextrose infusion can be used. The indications and technical details of the protective techniques will be discussed here.
Key words: hepatic tumor ablation, radiofrequency ablation, microwave ablation
___________________________________________________________________________
Among the current locoregional therapies for the treatment of hepatocellular carcinoma (HCC), thermal ablation is considered an effective method of treatment. The technical success rate is approximately 90% and the complication rate is typically less than 5%.1 The local tumor progression rate can range from 2% to 53%, depending on multiple factors, including tumor size and location,2 and ablation can be curative in lesions up to 3 cm. Generally, unsuccessful procedures and local recurrence are influenced by tumor size, presence of adjacent vessels greater than 3 mm in diameter, and tumor biology.3 Some patients may not receive percutaneous thermal ablative therapy (PTAT) because of the location of the liver lesion. Also, suboptimal needle tip placement in the tumor due to concerns of heat-induced complication in adjacent organs may lead to incomplete ablation. Thermally induced injuries may occur when the tumor margin is less than 1 cm away from the bowel, stomach, gallbladder, kidney, or diaphragm.
A meta-analysis on percutaneous radiofrequency ablation (RFA) of liver tumors, which included 2,320 patients and 3,554 lesions, showed the mortality, major complications, and minor complication rates to be 0.3%, 2.2%, and 4.7%, respectively.4 Bowel and stomach perforations were the primary organ injuries associated with mortality and major complications. In addition, minor complications secondary to thermal injury often involved damage to the right renal parenchyma. Before the introduction of organ displacement techniques, the presence of adjacent structures, particularly the bowel, within 1 cm of the target lesion was considered a contraindication to PTAT of hepatic malignancies.5 Using this criterion, it is expected that some patients — with treatable and potentially curable lesions — would miss the opportunity of having the most effective locoregional therapy to treat HCC in a minimally invasive fashion. The treatment alternatives for this group of HCC patients (fewer than 3 lesions, with diameter less than 3 cm; 1 lesion with diameter less than 5 cm) with comparable or better results are liver transplantation, hepatectomy, or surgical thermal ablation (under laparotomy or video-laparoscopy), which are all more invasive procedures. The real benefit from the thermal protection techniques is unknown, but the indications for the treatment of liver cancer with PTAT could be expanded and the rates of mortality and complications possibly reduced. The goal is to describe the protection techniques (PT) used during the PTAT of challenging HCC lesions.
Material and Methods
This retrospective study was determined by the Institutional Review Board to be exempt from their review. From January 2008 to December 2011, a total of 164 HCC patients (Child-Pugh A or B) and 219 lesions were treated using ablation under computed tomography (CT) guidance. All the patients had either (1) 3 or fewer lesions with no lesion greater than 3 cm in maximum diameter or (2) 1 lesion less than 5 cm in maximum diameter. Fifty-seven microwave ablation (MWA) and 162 RFA were used in total (Evident MWA and Cool-tip RFA systems, Covidien). Thermal PT was required in 18.9% (31/164) of patients because the tumor margin was less than 1 cm from the adjacent organ. The type of PT performed was determined by the tumor location and the ability to provide consistent protection throughout the procedure. The PT techniques utilized were hydrodissection, gallbladder lavage, balloon interposition, carbon dioxide (CO2) pneumoperitoneum, and bile duct lavage. Most of the liver ablations were performed under moderate sedation with intravenous administration of midazolam and fentanyl. Endotracheal intubation was performed in patients who underwent the CO2 pneumodissection and in those with respiratory comorbidities or class IV airway Mallampati classification. Ciprofloxacin was administered intravenously for infection prophylaxis. Informed consent was obtained for the PTAT and for the adjacent organ protection. The patients were then followed in our clinic at 30 days and then every 3 months.
Hydrodissection
This technique involves instilling fluid into the intra- or retroperitoneal spaces to push adjacent organs, such as the diaphragm, large bowel, right kidney, and stomach, away from the liver during PTAT. The adjacent organ must be pushed ideally more than 1 cm away from the ablation zone, which should include 1 cm of safety margin of “normal liver” around the tumor. In HCC lesions that reach the capsule, without invasion of adjacent organs, the hydrodissection allows adequate ablation of the entire tumor. Sterile water, 0.9% normal saline, 0.5% lidocaine, and 5% dextrose in water (D5W) have been used for this PT.6 The D5W is likely the safest as it is nonionic, more iso-osmolar than free water, and quickly absorbed.
 The volume of instilled fluid varies considerably (from 100 cc to 1,000 cc) depending on the tumor location and on the fluid seepage into adjoining anatomic spaces, such as the right pericolic gutter and Morrison’s pouch.6 Because of the fluid seepage and the risk of quick D5W absorption, we perform continuous infusion at a rate of 500 cc/hour after the initial bolus infusion (100 cc to 200 cc). This strategy creates a continuous column of fluid (hydrodissection) that protects adjacent organ(s).
The volume of instilled fluid varies considerably (from 100 cc to 1,000 cc) depending on the tumor location and on the fluid seepage into adjoining anatomic spaces, such as the right pericolic gutter and Morrison’s pouch.6 Because of the fluid seepage and the risk of quick D5W absorption, we perform continuous infusion at a rate of 500 cc/hour after the initial bolus infusion (100 cc to 200 cc). This strategy creates a continuous column of fluid (hydrodissection) that protects adjacent organ(s).
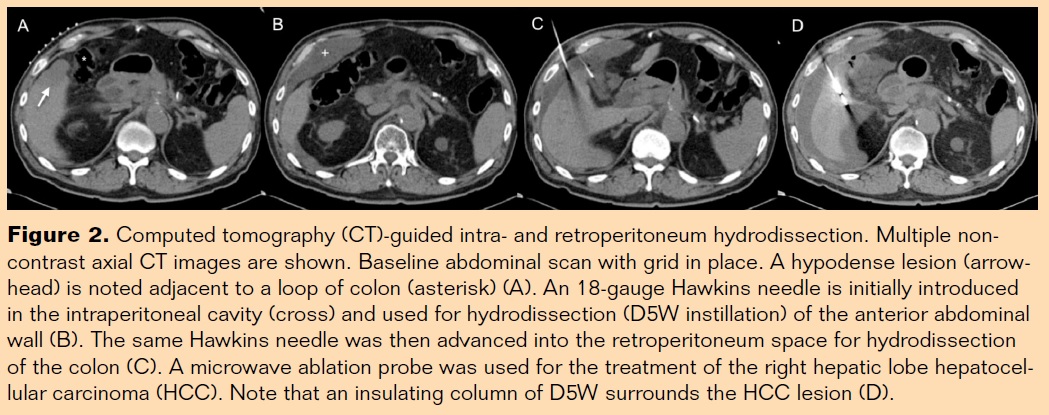
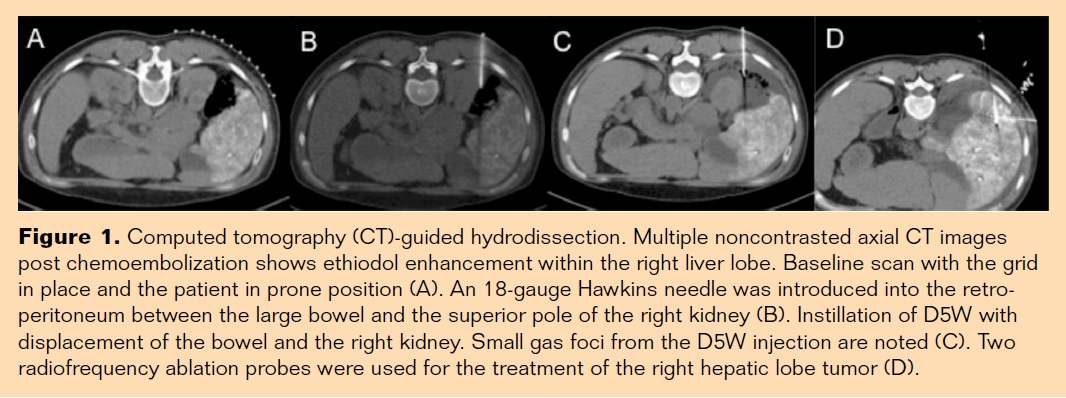
Alternatively, repositioning of the needle tip to an adjacent fat plane can be beneficial if significant spillage into the peritoneal cavity is noted. A grid is placed on the skin that overlays the target area and a baseline abdominal computed tomography (CT) scan is obtained for procedure planning (Figures 1A and 2A). It is important to keep in mind that the adjacent organ position may change in relation to the tumor during the procedure, especially if the patient moves on the CT table. All treatment needles are placed prior to the beginning of hydrodissection. Using standard sterile technique and under local anesthesia, an 18-gauge Hawkins-Akins needle (Cook Medical), initially with the sharp tip mandril, is used to obtain access into the intraperitoneal (Figure 2B) or retroperitoneal spaces (Figure 2C) under CT or ultrasound (US) guidance. Frequently, the Hawkins-Akins sharp tip mandril is exchanged for the blunt tip mandril. This allows the advancement of the needle atraumatic tip into a deeper location, displacing the adjacent organ (stomach, duodenum, bowel, kidney) without perforating it (Figure 1B). Often, 20 cc to 30 cc of D5W is hand injected immediately after the Hawkins-Akins needle (sharp mandril) insertion. Hydrodissection of a virtual space is performed, which allows the needle (now with blunt mandril) to reach deeper locations safely. When CT verifies the adequate needle tip position, the continuous infusion of D5W is started (Figures 1C, 1D, 2C, 2D). Following the ablation procedure, it is unnecessary to aspirate the residual D5W because it is quickly absorbed. It is important to monitor blood glucose levels in diabetic patients undergoing hydrodissection with D5W both during and after the procedure as they will be prone to hyperglycemia do to absorption. Hyperglycemia may be treated with sliding scale insulin based on the blood glucose levels.
Pneumodissection
This technique utilizes the infusion of CO2 into the intra- or retroperitoneal spaces with the goal to displace adjacent organs away from the liver, especially the diaphragm. It is performed under CT guidance because the gas causes image artifact when magnetic resonance or US are used. The patient must be intubated for mechanical ventilation. The pneumoperitoneum is painful and tends to cause basal lung atelectasis. The patient’s CO2 level should be checked with capnography. We believe that there is more accuracy placing all of the treatment needles before the beginning of pneumodissection. Often, adjustments in needle depth may be required as the liver is displaced from the abdominal wall and the diaphragm.
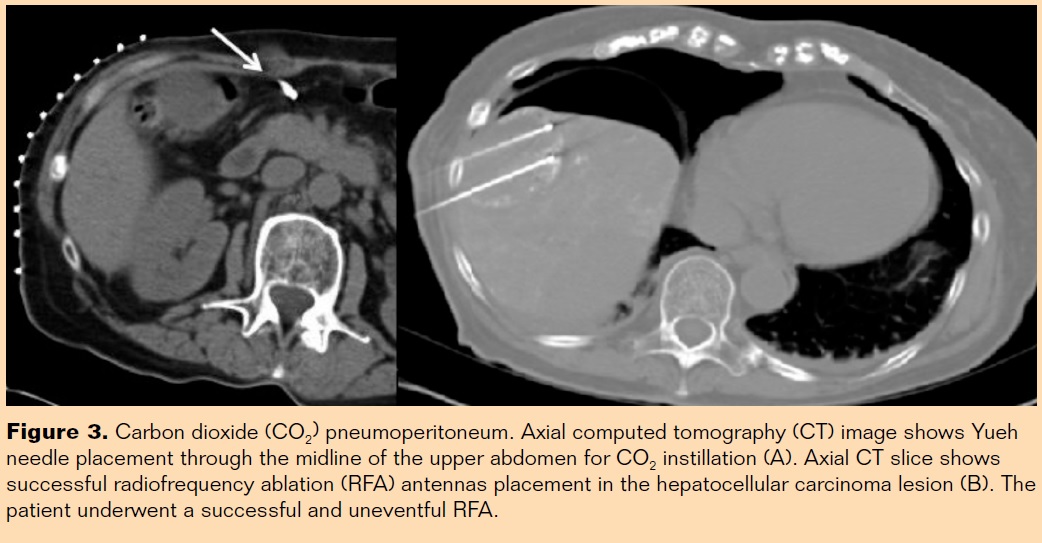 Initially, an 18-gauge Yueh needle (Cook Medical) is inserted in the peritoneal cavity (Figure 3A) and then connected to an electronic CO2 endoflator (Karl Storz). The CO2 infusion rate is set to 1L/min, the maximum abdominal pressure is set to 10 mmHg, and usually it takes 2L to 3L to achieve this pressure level. The CO2 equipment is the same used for video laparoscopic procedures. When CT images show the liver edge is greater than 15 mm from the adjacent organ, the ablation procedure may be started (Figure 3B, 3C). Carbon dioxide is insufflated as needed to keep the intra-abdominal pressure at 10 mmHg, as gas can shift, diffuse, or resorb over time. Larger and variable volumes of CO2 must be used when compared to hydrodissection given its tendency to diffuse from the initial site of injection. It has been suggested that approximately 1,250 cc can distract bowel by approximately 15 mm, although 20 cc to 50 cc may produce a similar effect when injected into more confining spaces such as the retroperitoneum.7 Interval CT scans are used to confirm adequate displacement of adjacent organs. Depending on the tumor location, the right and left triangular and the coronary ligaments may limit the pneumodissection protection. Although rare, potential complications of pneumodissection are hypotension, bradycardia, and gas embolization.
Initially, an 18-gauge Yueh needle (Cook Medical) is inserted in the peritoneal cavity (Figure 3A) and then connected to an electronic CO2 endoflator (Karl Storz). The CO2 infusion rate is set to 1L/min, the maximum abdominal pressure is set to 10 mmHg, and usually it takes 2L to 3L to achieve this pressure level. The CO2 equipment is the same used for video laparoscopic procedures. When CT images show the liver edge is greater than 15 mm from the adjacent organ, the ablation procedure may be started (Figure 3B, 3C). Carbon dioxide is insufflated as needed to keep the intra-abdominal pressure at 10 mmHg, as gas can shift, diffuse, or resorb over time. Larger and variable volumes of CO2 must be used when compared to hydrodissection given its tendency to diffuse from the initial site of injection. It has been suggested that approximately 1,250 cc can distract bowel by approximately 15 mm, although 20 cc to 50 cc may produce a similar effect when injected into more confining spaces such as the retroperitoneum.7 Interval CT scans are used to confirm adequate displacement of adjacent organs. Depending on the tumor location, the right and left triangular and the coronary ligaments may limit the pneumodissection protection. Although rare, potential complications of pneumodissection are hypotension, bradycardia, and gas embolization.
Balloon Interposition
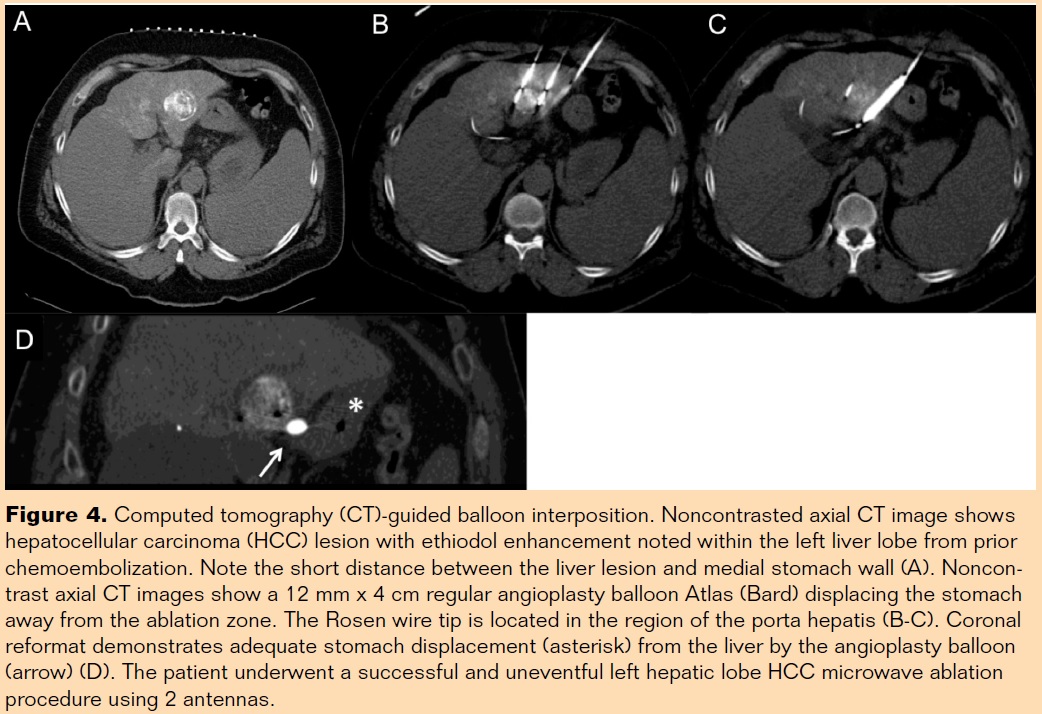 This technique uses a standard balloon catheter, commonly used for angioplasty, to displace adjacent organs (e.g. stomach, duodenum, bowel) from marginal hepatic malignancies.8 Under CT guidance, an 18-gauge Trocar needle is advanced to the virtual plane between the liver and the adjacent organ. Following this, a .035˝ diameter, 180 cm long, stiff Amplatz wire (Boston Scientific) or a .035˝ diameter, 145 cm long Rosen wire (Cook Medical) is carefully advanced to the peritoneal cavity. A 7 Fr introducer sheath is advanced until the peritoneal cavity is reached to secure access through the abdominal wall. The distance between the organ to be displaced and the skin is measured and the balloon catheter positioned according to this length. The balloon is unsheathed for insufflation and resheathed in case there is accidental balloon rupture. Typically, a 10 mm to 12 mm angioplasty balloon is enough to create an adequate gap between the liver border and adjacent organ. The balloon’s interposition can be used as the primary PT or when other options such as hydro- or pneumodissection have failed. Care must be taken to adequately secure the balloon in place before ablation begins. It may be inflated either with room air (negative contrast) or with very diluted iodine contrast solution (1 cc of contrast: 9 cc of sterile saline). Higher contrast concentrations will lead to image artifacts. Adequate separation (at least 10 mm) has to be documented by CT (Figure 4) before the PTAT begins. Balloons offer protection via physical displacement and by their ability to serve as a thermal blanket. Theoretically, thermal-induced balloon rupture may happen when the ablation probe is less than 7 mm away. This is particularly concerning if the antenna tip is oriented in parallel to the balloon catheter shaft. It is noteworthy that multiple balloons may be needed for the adequate ablation of lobulated or amorphous lesions.
This technique uses a standard balloon catheter, commonly used for angioplasty, to displace adjacent organs (e.g. stomach, duodenum, bowel) from marginal hepatic malignancies.8 Under CT guidance, an 18-gauge Trocar needle is advanced to the virtual plane between the liver and the adjacent organ. Following this, a .035˝ diameter, 180 cm long, stiff Amplatz wire (Boston Scientific) or a .035˝ diameter, 145 cm long Rosen wire (Cook Medical) is carefully advanced to the peritoneal cavity. A 7 Fr introducer sheath is advanced until the peritoneal cavity is reached to secure access through the abdominal wall. The distance between the organ to be displaced and the skin is measured and the balloon catheter positioned according to this length. The balloon is unsheathed for insufflation and resheathed in case there is accidental balloon rupture. Typically, a 10 mm to 12 mm angioplasty balloon is enough to create an adequate gap between the liver border and adjacent organ. The balloon’s interposition can be used as the primary PT or when other options such as hydro- or pneumodissection have failed. Care must be taken to adequately secure the balloon in place before ablation begins. It may be inflated either with room air (negative contrast) or with very diluted iodine contrast solution (1 cc of contrast: 9 cc of sterile saline). Higher contrast concentrations will lead to image artifacts. Adequate separation (at least 10 mm) has to be documented by CT (Figure 4) before the PTAT begins. Balloons offer protection via physical displacement and by their ability to serve as a thermal blanket. Theoretically, thermal-induced balloon rupture may happen when the ablation probe is less than 7 mm away. This is particularly concerning if the antenna tip is oriented in parallel to the balloon catheter shaft. It is noteworthy that multiple balloons may be needed for the adequate ablation of lobulated or amorphous lesions.
Gallbladder, Bile Duct, and Stomach Lavage
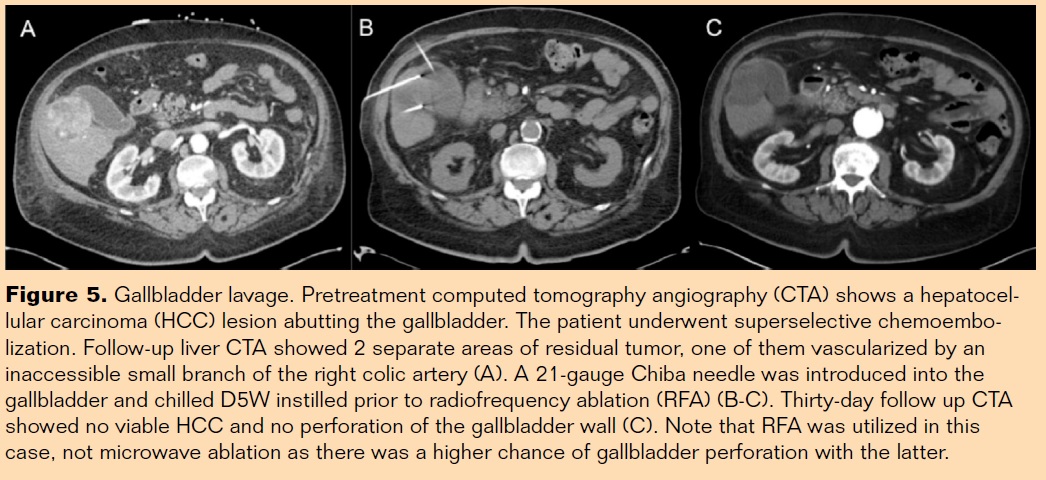 Liver ablation adjacent to the stomach, gallbladder, and main bile ducts can be technically challenging due to the risk of organ perforation and of bile duct stricture. Animal studies showed protective effects on gastric lavage and gallbladder lavage when the ablation was performed approximately 5 mm apart during RFA.9,10 It should be noted that the risk of gallbladder damage is increased when the antenna is oriented parallel to the gallbladder’s long axis as opposed to perpendicular. Chilled D5W for the lavage of the stomach, gallbladder, and bile ducts11 may be useful protection techniques during liver PTAT. Gastric and bile duct lavage requires endoscopy for the insertion of nasogastric and nasobiliary tubes, respectively. The gallbladder lavage may be performed percutaneously using a 21-gauge Chiba needle under CT or US guidance. The combination of a small caliber needle introduced through the liver parenchyma without tumor minimizes the risk of postprocedure bile peritonitis. Initially, needle aspirative bile drainage of the gallbladder is performed for decompression, avoiding over distension that could result in seepage or bacteremia. Chilled D5W is then hand injected in a bolus of 30 cc to 50 cc, followed by continuous infusion at rate of 50 cc/hour. The liver ablation can be started with the antennas preferably placed perpendicularly to the gallbladder (Figures 5A and 5B).
Liver ablation adjacent to the stomach, gallbladder, and main bile ducts can be technically challenging due to the risk of organ perforation and of bile duct stricture. Animal studies showed protective effects on gastric lavage and gallbladder lavage when the ablation was performed approximately 5 mm apart during RFA.9,10 It should be noted that the risk of gallbladder damage is increased when the antenna is oriented parallel to the gallbladder’s long axis as opposed to perpendicular. Chilled D5W for the lavage of the stomach, gallbladder, and bile ducts11 may be useful protection techniques during liver PTAT. Gastric and bile duct lavage requires endoscopy for the insertion of nasogastric and nasobiliary tubes, respectively. The gallbladder lavage may be performed percutaneously using a 21-gauge Chiba needle under CT or US guidance. The combination of a small caliber needle introduced through the liver parenchyma without tumor minimizes the risk of postprocedure bile peritonitis. Initially, needle aspirative bile drainage of the gallbladder is performed for decompression, avoiding over distension that could result in seepage or bacteremia. Chilled D5W is then hand injected in a bolus of 30 cc to 50 cc, followed by continuous infusion at rate of 50 cc/hour. The liver ablation can be started with the antennas preferably placed perpendicularly to the gallbladder (Figures 5A and 5B).
Results
Among the 164 HCC patients treated with PTAT, 31 patients underwent the protection techniques. They had the following distribution: 16 hydrodissection, 6 gallbladder lavage, 4 balloon interposition, 3 CO2 pneumoperitoneum, 2 bile duct lavage. Global technical success, defined by adequate ablative needle(s) placement and adjacent organ protection through the entire procedure, was 100%. There were no complications in the patients (0/31) who had PT. The PTs started to be utilized in our group in January 2011. Before that, 112 HCC patients had PTAT and the heat-related complication rate was 2% (2/112). Perforations occurred in the large bowel of 1 patient and in the gallbladder of 1 patient. They were managed with long-term percutaneous drain catheter placement and antibiotics and had positive outcomes. Both lesions had the tip of the MWA antennas located about 7 mm to 10 mm from the perforated organs. The gallbladder perforation had the antenna placed parallel to the longer axis of this organ. All PTATs are performed under CT guidance; however, some PTs may require additional US assistance for accurate intra- or retroperitoneal needle positioning. The PTs during the liver ablations increased the total procedure time by 25 minutes on average (range from 22 minutes to 45 minutes additional time). Cost analysis of the protective techniques was not performed.
Discussion
Among the current locoregional therapies, RFA and MWA are safe and very effective for the treatment of this group of HCC patients (fewer than 3 lesions, with diameter less than 3 cm; or one lesion with diameter less than 5 cm). The use of PTAT has increased over the last decade (primarily in patients with less than 3 lesions, each one <3 cm in diameter, or with a single lesion <5 cm in diameter) and it is quickly replacing hepatectomy as first-line therapy for Child-Pugh A patients with HCC. Among the relevant PTAT complications, several heat-related injuries have been reported in the literature and include organ perforation (stomach, small and large bowel, diaphragm, pericardium), hepatopericardial fistula, biliary stricture, and renal infarct.4,5 The large bowel is the most susceptible and most common abdominal organ injured during PTAT of hepatic malignancies. In addition, the stomach is also at significant risk during left hepatic ablations, although less so because the gastric wall is thicker. Less common are reports of diaphragmatic necrosis and perforation.7 Previous studies have shown that approximately 14% of all major complications after liver ablations are related to thermal injury of adjacent structures and that 25% of these resulted in death (secondary to bowel perforation).4
In a study with 215 HCC patients treated by PTAT, the central and the difficult peripheral lesions had local tumor recurrence of 3.1% and 8.4%, respectively. It is interesting to note that each study patient served as his or her own internal control because they had not only peripheral lesions in difficult locations but also more centralized lesions not abutting adjacent structures.12 Therefore, the PT should always be considered when the lesion(s) are located at liver edge (peripheral) and in those close to the main bile ducts and to the gallbladder. Early investigation on methods to minimize thermal-induced injuries secondary to PTAT included the aspiration of bowel contents to promote decompression. Varied patient positioning was also attempted in an effort to displace the small bowel. Unfortunately, these strategies were sporadically successful at best.
Over the last 5 years, the development of PT has widened the indications to treat hepatic malignancies that would have otherwise been accessible but contraindicated due to the high risk of thermal injuries. The most common PT is hydrodissection (artificial ascites). Because normal saline is an ionic solution, it is not recommended as it has been shown to conduct heat and electricity more than sterile distilled water or D5W.6 Of note is a recent study that showed the feasibility and efficacy of hydrodissection in 143 patients with HCC abutting the diaphragm or bowel.13 Carbon dioxide pneumodissection is relatively simple, and it is similar to the pneumoperitoneum created during abdominal video laparoscopies. Also, the thermal conductivity of CO2 is approximately 37 times less than that of water, making the choice of gas or balloon interposition more appealing in cases where damage to bowel wall is likely to occur.7 Also, it is important to understand the anatomic spaces surrounding the liver. The instillation of 50 cc of gas or D5W often produces different tissues distraction depending on if it is applied within the intra- or retroperitoneal spaces. Any prior surgeries can alter how hydro- (fluid) and pneumodissection (air) can track around the liver and adjoining spaces.
In our experience, RFA antennas are preferred over MWA devices when there is risk of thermal injury during PTAT procedures. Before PTs were used, 2 of 112 HCC patients had thermal-injury secondary to the PTAT. Retrospective case review showed that both bowel and gallbladder perforations had the antennas too close for a procedure without protection. The MWA energy is more powerful, and consequently the temperature rises more quickly around the antenna. Typically, it is much less susceptible than RF to the heat-sink effect when peritumor blood vessels that are greater than 3 mm steal heat faster than it can be delivered to cause tumor necrosis. On the other hand, RF energy provides more “gentle” ablation, but it is still capable of causing thermal-induced complications.
Even if the distraction distances necessary to provide appropriate thermal insulation are not fully agreed upon, we use a distance greater than 10 mm as a safety margin. It is important to remember that, depending on the antenna used, the heat zone may reach up to 7 mm beyond the needle tip. Also relevant, the ablation zone may be influenced by fat tissue, cirrhotic liver, air (thermal insulators) and adjacent blood vessels (heat dissipation) greater than 3mm surrounding the tumor.
The real effectiveness of PTs is difficult to assess in controlled trials with humans. However, a recent study demonstrated that cooling of bile ducts with a nasogastric tube could prevent biliary complications induced by RFA of HCC close to major bile ducts without increasing local recurrence.14 Similarly, hydrodissection for percutaneous RFA of HCC lesions abutting the diaphragm had a significant effect on thermal protection of the diaphragm, but not on therapeutic efficacy.15 Also, gastric lavage during RFA of the liver in a porcine model has demonstrated significant protective effects of the gastric wall vs control.9 Protection techniques had no complications and they increased the total time of liver ablations 25 minutes on average, which was felt not to be a problem. Cost analyses were not performed for PT, but it is likely that the relative low cost of the needles (Hawkins, Chiba) of the CO2 infusion and of the angioplasty balloon and ancillary devices is quite a bit lower than the expense of a liver open surgical resection or open/video laparoscopic-assisted ablation. However, endoscopic-assisted PTs are expected to be more costly. Still, the benefit of protecting the patient with these techniques probably outweighs the cost of managing bile duct strictures or gastric perforation.
Liver lesion location should dictate the type of PT to be selected. Hydrodissection (16/31 cases) was the most commonly used. It is relatively simple to perform, costs less, and effectively protects the right upper quadrant anterior abdominal wall, the hepatic flexure of the colon, and the right kidney. Because D5W is quickly absorbed or it may move to a different anatomical space, we routinely use continuous infusion (500 cc/hour) throughout the procedure. In diabetic patients, sterile distilled water is preferred over D5W. Adjacent organs to the left hepatic lobe might be better protected when the balloon interposition technique is used, because hydrodissection may be limited due to the seepage of the fluid to the splenic fossa or to the left parietocolic gutter. In hepatic dome lesions, we believe that CO2 pneumoperitoneum has advantages over hydrodissection because it displaces the liver from the diaphragm more consistently. Again, hydrodissection in this area has the risk of seepage. Obviously, CO2 pneumoperitoneum has limited application in displacing the liver away from the diaphragm where the coronary and triangular ligaments insert.
Conclusion
Thermal protection strategies are technically feasible and safe. They should be considered for the treatment of liver cancer situated in challenging locations that typically would represent a relative contraindication for PTAT. Also, PTs may provide a more adequate ablation zone (including the 1 cm safety margin) despite proximity of adjacent organs. Protection techniques may expand the number of patients that can benefit from PTAT, while decreasing the incidence of major complications. More studies are needed to define the precise role these techniques play during liver percutaneous ablations.
References
- Guimaraes M, Uflacker R. Locoregional therapy for hepatocellular carcinoma. Clin Liver Dis. 2011;15(2):395-421.
- Nakazawa T, Kokubu S, Shibuya A, et al. Radiofrequency ablation of hepatocellular carcinoma: correlation between local tumor progression after ablation and ablative margin. AJR Am J Roentgenol. 2007;188(2):480-488.
- Lu DSK, Raman SS, Limanond P, Aziz D, Economou J, Busuttil R, Sayre J. Influence of large peritumoral vessels on outcome of radiofrequency ablation of liver tumors. J Vasc Interv Radiol. 2003;14:1267–1274.
- Livraghi T, Solbiati L, Meloni MF, Gazelle GS, Halpern EF, Goldberg SN. Treatment of focal liver tumors with percutaneous radio-frequency ablation: complications encountered in a multicenter study. Radiology. 2003;226(2):441-451.
- Rhim H, Dodd GD 3rd, Chintapalli KN, et al. Radiofrequency thermal ablation of abdominal tumors: lessons learned from complications. Radiographics. 2004;24(1):41-52.
- Laeseke PF, Sampson LA, Brace CL, Winter TC 3rd, Fine JP, Lee FT Jr. Unintended thermal injuries from radiofrequency ablation: protection with 5% dextrose in water. AJR Am J Roentgenol. 2006;186:S249-S254.
- Raman SS, Aziz D, Chang X, Sayre J, Lassman C, Lu D. Minimizing diaphragmatic injury during radiofrequency ablation: efficacy of intraabdominal carbon dioxide insufflation. AJR Am J Roentgenol. 2004;183(1):197-200.
- Yamakado K, Nakatsuka A, Akeboshi M, Takeda K. Percutaneous radiofrequency ablation of liver neoplasms adjacent to the gastrointestinal tract after balloon catheter interposition. J Vasc Interv Radiol. 2003;14(9):1183-1186.
- Lee J, Lim HK, Choi D, Kim SH, Min K, Jeon YH. Radiofrequency ablation of the liver abutting stomach: in vivo comparison of gastric injury before and after intragastric saline administration in a porcine model. Eur J Radiol. 2009;72(1):154-159.
- Lee J, Rhim H, Jeon YH, et al. Radiofrequency ablation of liver adjacent to body of gallbladder: histopathologic changes of gallbladder wall in a pig model. AJR Am J Roentgenol. 2008;190(2):418-425.
- Ogawa T, Kawamoto H, Kobayashi Y, et al. Prevention of biliary complication in radiofrequency ablation for hepatocellular carcinoma-cooling effect by endoscopic nasobiliary drainage tube. Eur J Radiol. 2010;73(2):385-390.
- Chen MH, Yang W, Yan K, et al. Radiofrequency ablation of problematically located hepatocellular carcinoma: tailored approach. Abdom Imaging. 2008;33(4):428-436.
- Song I, Rhim H, Lim HK, Kim YS, Choi D. Percutaneous radiofrequency ablation of hepatocellular carcinoma abutting the diaphragm and gastrointestinal tracts with the use of artificial ascites: safety and technical efficacy in 143 patients. Eur Radiol. 2009;19(11):2630-2640
- Lieberman S, Goldin E, Lotem M, Bloom AI. Irrigation of the bile ducts with chilled saline during percutaneous radiofrequency ablation of a hepatic ocular melanoma metastasis. AJR Am J Roentgenol. 2004;183(3):596-598.
- Kang TW, Rhim H, Lee MW, et al. Radiofrequency ablation for hepatocellular carcinoma abutting the diaphragm: comparison of effects of thermal protection and therapeutic efficacy. AJR Am J Roentgenol. 2011;196(4):907-913.
Editor’s note: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript received February 2, 2016; provisional acceptance given April 2, 2016; manuscript accepted April 13, 2016.
Address for correspondence: Patrick Gilbert MD, Vascular & Interventional Radiology, Medical University of South Carolina, 25 Courtenay Drive, MSC 226, Charleston, SC 29425. Email: gilberp@musc.edu
Suggested citation: Gilbert P, Arrington D, Yamada R, Hannegan C, Anderson MB, Selby Jr B, Guimaraes M. Protective techniques in image-guided percutaneous hepatic ablations. Intervent Oncol 360. 2016;4(5):E75-E85.

