


Percutaneous Transpleural Radiofrequency Ablation of Hepatic Dome Hepatocellular Carcinoma Aided by CO2 Pneumothorax Creation
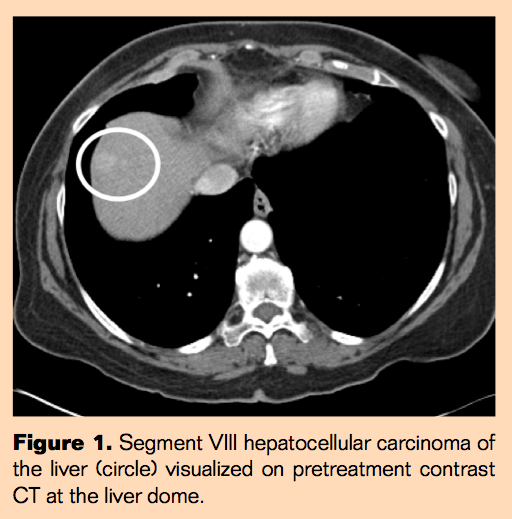
A 70-year-old female presented with cirrhosis secondary to nonalcoholic steatohepatitis and subsequent diagnosis of hepatocellular carcinoma in segments II and VIII in 2009. The patient was status post transjugular intrahepatic portosystemic shunt creation 7 years prior for upper gastrointestinal bleed and was considering liver transplantation, needing potential minimally invasive “bridge” treatments to prevent further progression of disease. She was status post radiofrequency ablation (RFA) treatment of segment II hepatic lesions with no evidence of local residual disease in the ablation zone and now presented with a segment VIII 2-cm hepatic lesion consistent with hepatocellular carcinoma.
Case Images
Treatment of Hepatic Dome Lesions
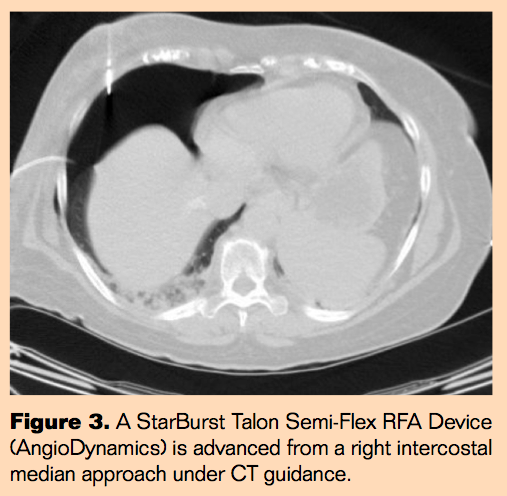
Percutaneous ablative treatments are complicated by the proximity of the diaphragm, lung, and overlying ribs, resulting in a complex geometry for needle placement.1 Access options include transhepatic steep cranial angulated needle access (“climbing liver”) from a subcostal approach, direct intercostal transthoracic needle access after creating CO2pneumothorax to avoid interposed lung,2 and D5W hydrodissection, which may complement both approaches to limit thermal injury to the diaphragm in select cases.3
Discussion
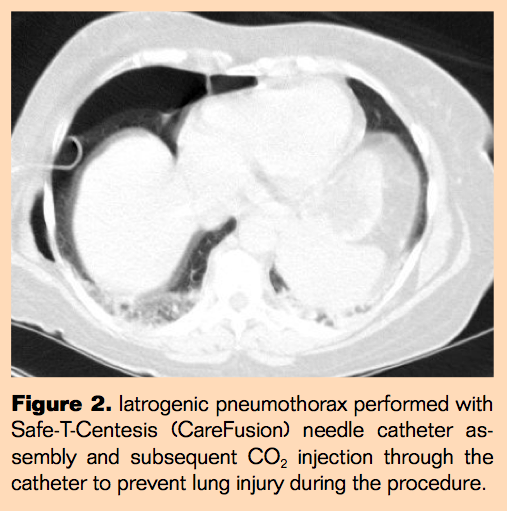
Needle advancement during RFA treatment of hepatic dome lesions may require a steep subcostal approach to avoid the lung. To mitigate the possible complexity of a steep cranial needle approach through the liver, CO2-facilitated pneumothorax creation can be utilized, allowing for a direct transpleural percutaneous needle path. Placement of the RFA needle at an acute angle to reach the hepatic dome often is performed without complication, but it carries the risk of damage nearby hepatic arterial or venous structures. D5W infusion in the subdiaphragmatic space along the bare area of the liver may also be used as an adjunctive technique to protect the diaphragm from the thermal effect of RFA. D5W infusion carries a small risk of inducing sympathetic pleural effusion and atelectasis as reported by Uehara et al and Iwai et al.4,5 CO2-induced “protective pneumothorax” allows for adequate displacement of the lung parenchyma from the hepatic lesion and safe passage of the needle with minimal complications. Low complication rate is due to rapid evacuation of CO2 with chest tube and passive absorption by the lung parenchyma during and after the procedure. An additional benefit of CO2 administration is greater impedance of heat generated by radiofrequency and thermal energy compared to D5W. Contraindications to CO2-facilitated pneumothorax are few and relative including pleural adhesions and air leak requiring tube drainage.6,7
Conclusion
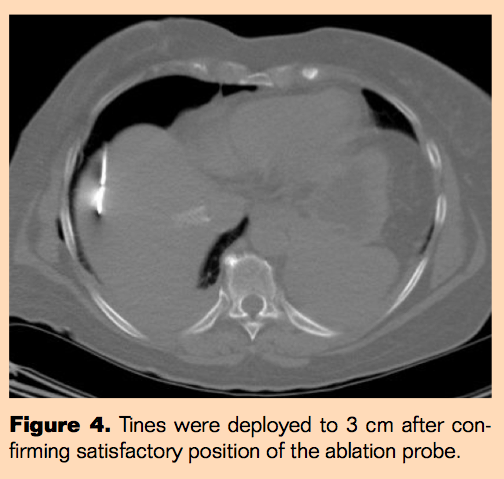
CO2 pneumothorax creation may be helpful to streamline and simplify needle access to hepatic dome lesions. The CT lung window should be checked with interval needle advancements to avoid injury to the re-expanding lung. Additional CO2 may need to be administered to maintain a satisfactory percutaneous window. If the lesion is not immediately abutting the capsule, hydrodissection may not be necessary to protect from diaphragmatic thermal injury.
Editor’s note: This article underwent peer review by one or more members of the Interventional Oncology 360 editorial board.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no disclosures related to the content of this manuscript.
Recommended citation: Meshkov D, Salsamendi J. Percutaneous transpleural radiofrequency ablation of hepatic dome hepatocellular carcinoma aided by CO2 pneumothorax creation. Intervent Oncol 360. 2013;1(1):E15-E18.

