


ADVERTISEMENT
Optimizing Reimbursement for Radioembolization: The Importance of Adequate Documentation
ABSTRACT: Purpose: This article aims to review radioembolization-specific coding guidelines so that interventional radiologists can develop a better understanding of what documentation is essential in their reports, leading to appropriate authorization and reimbursement. Background: Over the past 10 years, interventional radiologists (IRs) have been performing increasing numbers of radioembolization procedures in treatment of hepatic malignancy. This article will review coding for radioembolization procedures, from initial interventional radiology clinic visit to postprocedure follow-up imaging. The article will highlight the importance of adequate documentation during clinic visits, image-guided interventions, and postprocedure cross-sectional imaging to ensure efficient insurance authorization and maximal reimbursement. Materials and Methods: The treatment of liver tumors with radioembolization merges key concepts well known to radiation oncology and interventional radiology practices. A typical radioembolization case includes the initial patient consultation; a diagnostic angiogram to allow for treatment planning and possible pretreatment embolization of arteries such as the gastroduodenal artery, right gastric artery, and/or supraduodenal artery; and the actual yttrium-90 radioembolization treatment. SPECT nuclear medicine scans for tumor localization and contrast-enhanced multiphasic cross-sectional imaging for therapy planning and follow-up are also obtained. Thorough documentation of patient history, indications for treatment, appropriateness of therapy, and dosimetry calculations by interventional radiologists are critical to obtain procedural approval by insurance companies and appropriate reimbursement. This article will detail the current procedural terminology codes relevant to radioembolization and highlight the importance of adequate documentation throughout the treatment process. Conclusion: The emergence of radioembolization in the treatment of hepatic malignancy brings challenges for IRs that make clear, precise documentation critical. An understanding of radioembolization coding will allow IRs to provide improved documentation, leading to more efficient treatment authorization and reimbursement by insurance companies.
Key words: yttrium-90, radioembolization, interventional oncology, reimbursement, billing, coding
______________________________________________________________
Clinical trials evaluating the use of yttrium-90 (Y90) transarterial radioembolization for hepatic tumors date back to the 1960s.1 In recent years, Y90 has been increasingly utilized in treating hepatic metastases and hepatocellular carcinoma (HCC) with improved outcomes.2 In 1999, the US Food and Drug Administration (FDA) approved the use of TheraSphere (BTG) particles for HCC via the humanitarian device exemption. Subsequently, in 2002, SIR-Spheres (Sirtex) particles were approved for the treatment of hepatic colorectal cancer metastases with adjuvant intrahepatic artery chemotherapy of FUDR (floxuridine). Since then, Y90 has been utilized for a variety of off-label indications, such as neuroendocrine tumor metastases, breast metastases, uveal melanoma metastases, cholangiocarcinoma, sarcoma, prostate cancer, ovarian metastases, melanoma, renal cell carcinoma, and other hypervascular metastases.3,4 Radioembolization has demonstrated efficacy in the treatment of colorectal carcinoma liver metastases, with reports indicating improved overall survival from 9 months to 15.4-17.2 months.2,5 This burgeoning use of Y90 radioembolization as a successful, novel treatment modality for liver tumors requires interventional radiologists to familiarize themselves with coding, so that they are prepared to provide clear documentation in procedure reports to obtain authorization and optimize reimbursement.
Traditionally, interventional radiologists performed arterial embolization and radiation oncologists performed brachytherapy. However, Y90 radioembolization unites both of these disciplines via Y90 microspheres that are placed intra-arterially by an interventional radiologist. Over the past decade, interventional radiologists have been performing increasing numbers of radioembolization procedures in the treatment of intermediate- to advanced-stage liver-only or liver-dominant hepatic malignancy. However, unlike more traditional interventional oncologic procedures, Y90 radioembolization requires more comprehensive initial evaluation and management visits. Additionally, the documentation of treatment planning, radiation dosimetry calculations, and placement of radioactive sources are usually under the purview of radiation oncology and unfamiliar territory for the interventional radiologist. Consequently, these new developments present novel challenges with regards to coding and billing.
Coding for the administration of Y90 can be quite complex, as the multiple components of the procedure can result in a complicated procedure report. Each case presents a unique set of circumstances, and thus, it is essential that a well-organized operative report be maintained. For example, a separate current procedural terminology (CPT) code is assigned to each artery into which a catheter is placed for diagnostic imaging or intervention, and the operative report should describe this in detail. In order to receive appropriate procedural approval by insurance payers as well as optimum reimbursement, it is imperative that interventional radiologists adequately document the patient history, indications for treatment, appropriateness of therapy, and dosimetry calculations. Thus, an understanding of peer-reviewed guidelines and/or other reasons for treatment can be critical for appropriate payment. Logical and sequential documentation of the procedure allows certified coders to better understand every aspect of the case so that they can then accurately identify and apply CPT codes to optimize reimbursement.
This article will review radioembolization-specific coding guidelines so that interventional radiologists recognize the importance of proper documentation during clinic visits, image-guided interventions, and postprocedure cross-sectional imaging to ensure optimum reimbursement. In addition, this article will review the coding for radioembolization procedures from initial patient consultation to postprocedure follow-up imaging.
Procedure Overview
In entirety, the Y90 procedure involves (1) an initial patient consultation; (2) diagnostic angiogram to allow for treatment planning; (3) possible pretreatment embolization of arteries; (4) SPECT nuclear medicine scans for evaluation of shunt fraction and tumor localization; (5) cross-sectional imaging to evaluate tumor volumes, overall tumor burden, plan treatment, and confirm liver-only or liver-dominant disease; (6) Y90 radioembolization treatment; and (7) clinical follow-up — including office visits, labs, and multiphasic contrast-enhanced cross-sectional imaging. As previously stated, this procedure requires proficiency in certain aspects of clinical care that are less familiar to the interventional radiologist, such as comprehensive initial evaluation and management visits as well as radioactive seed placement, which presents novel challenges with respect to coding for reimbursement.
Overview of Current Procedural Terminology Codes
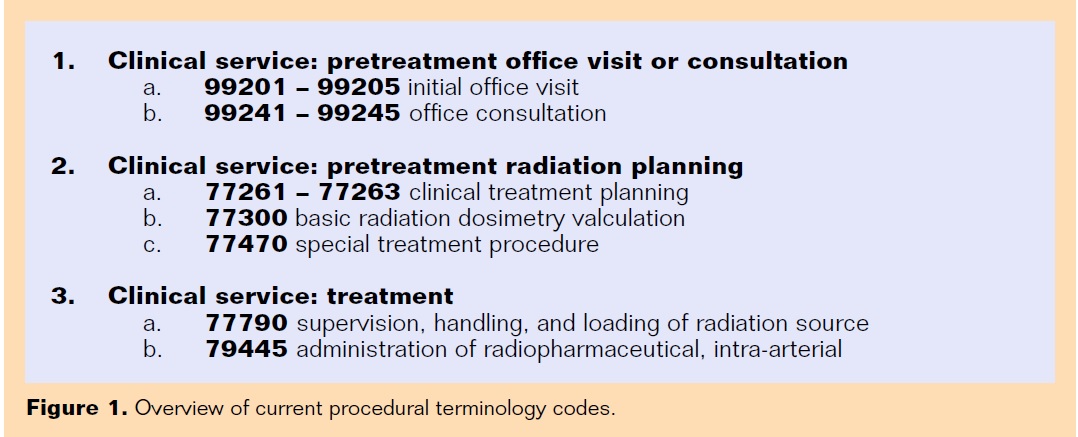 Coding for the procedure involves billing for 3 clinical services: (1) pretreatment office visit or consultation, (2) pretreatment radiation planning, and (3) treatment (Figure 1).
Coding for the procedure involves billing for 3 clinical services: (1) pretreatment office visit or consultation, (2) pretreatment radiation planning, and (3) treatment (Figure 1).
Pretreatment Office Visit or Consultation
The CPT codes for “pretreatment office visit or consultation” are (1) 99201 – 99205 “initial office visit,” (2) 99211 – 99215 “subsequent office visit,” and 99241 – 99245 “office consultation” (not for Medicare patients).
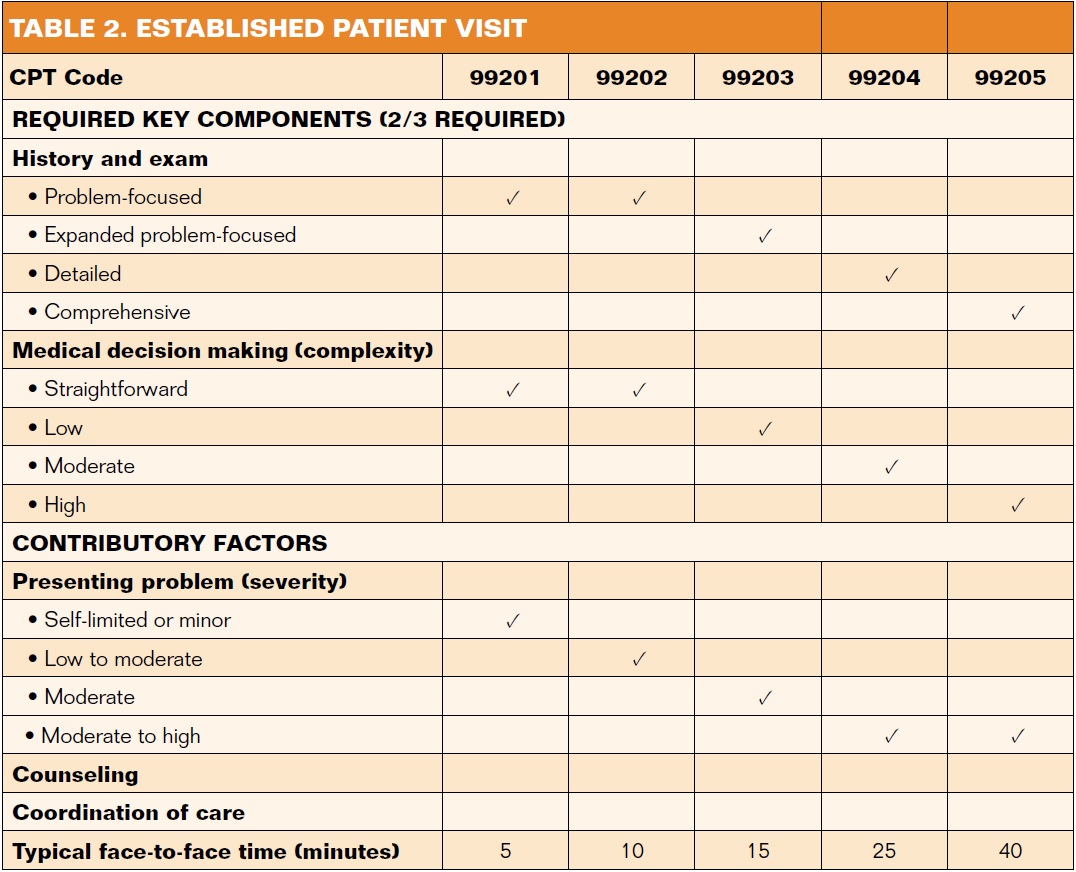
 It is imperative to properly document the request for consultation, document key elements of evaluation and management (history, physical exam, level of medical decision making, and/or the amount of time spent with the patient), report any clinical diagnoses (listing the most pertinent to microsphere therapy as the primary diagnosis), and provide a report of consultation to the requesting physician if appropriate (Tables 1 and 2). Although interventional radiologists may be tempted to use the CPT 99241-99245 “office consultation” codes, which offer greater reimbursement, Medicare does not reimburse for these codes even if all requirements are met.
It is imperative to properly document the request for consultation, document key elements of evaluation and management (history, physical exam, level of medical decision making, and/or the amount of time spent with the patient), report any clinical diagnoses (listing the most pertinent to microsphere therapy as the primary diagnosis), and provide a report of consultation to the requesting physician if appropriate (Tables 1 and 2). Although interventional radiologists may be tempted to use the CPT 99241-99245 “office consultation” codes, which offer greater reimbursement, Medicare does not reimburse for these codes even if all requirements are met.
Pretreatment Radiation Planning
 The CPT codes for “pretreatment radiation planning” are (1) 77261 – 77263 “clinical treatment planning,” (2) 77300 “basic radiation dosimetry calculation,” and (3) 77470 “special treatment procedure.”
The CPT codes for “pretreatment radiation planning” are (1) 77261 – 77263 “clinical treatment planning,” (2) 77300 “basic radiation dosimetry calculation,” and (3) 77470 “special treatment procedure.”
“Clinical treatment planning” offers insight into the considerations regarding the procedure plan and also outlines details of the selected plan. This should include a review of prior imaging/biopsy/surgery, details of any treatment already received, correlation of physical exam with prior testing, treatment volume determination, toxicity or tolerance concerns, treatment time/dosage and sequence of treatment modality, orders and medical reasons for imaging guidance (including frequency and modality), any concerns or variables unique to the patient, and care coordination. If an interventional radiologist is performing the procedure without a radiation oncologist, the treatment plan must be documented separately from the procedure report. The “basic radiation dosimetry calculation” should include the physician’s order, identify the areas being treated, provide the dose (GBq), and include a physician signature and date. “Clinical treatment planning” can only be billed once per case, whereas “basic radiation dosimetry calculation” can be billed as often as necessary. Finally, the “special treatment procedure” is used when extra time is required beyond the basic radiation dosimetry calculation, and this should include prior treatment and outcome, a review of current computed tomography (CT), liver function studies, Eastern Cooperative Oncology Group performance, and a dose calculation entry.
Treatment
Lastly, the CPT codes for “treatment” are (1) 77790 “Supervision, Handling and Loading of Radiation Source” and (2) 79445 “administration of radiopharmaceutical, intra-arterial.”
In terms of specific treatment codes, this will depend on whether the “authorized user” is the interventional radiologist or someone else, such as nuclear medicine physician or radiation oncologist. Thus, the billing in terms of the treatment codes will have some variability based on the infrastructure at each institution.
When documenting “supervision, handling, and loading of radiation source,” it is important to note the physician’s prescription and medical directive for the microsphere dose, which includes a statement about the observation of radiation safety standards as well as the technical component charge (but also appropriate in a freestanding facility). For “administration of radiopharmaceutical, intra-arterial,” the dose of Y90 microsphere and its successful delivery to the tumor bed should be recorded.
Postprocedure scintigraphy is typically utilized following both the mapping procedure and the radioembolization procedure. The imaging that occurs in the nuclear medicine department after administration of Tc-99m macroaggregated albumin or Yttrium microspheres can be planar (78201) or SPECT (78205) liver imaging. This report is typically dictated by the nuclear medicine physician.
Pitfalls in Documentation
The consequences of incomplete documentation are not strictly restricted to reduced reimbursement, as it can also result in an audit conducted by a medical recovery audit contractor or insurance company, which may generate additional fines and repayments. The most common components missing in the procedure report are fluoroscopy time, sedation start and end times, and a detailed account of the arteries and anatomic sites accessed.6
It is important for the interventional radiologist to know which procedures are covered by Medicare, Medicaid, and particular private insurers. With respect to Y90, Medicare has reimbursed providers under the hospital code C2616 in the hospital outpatient setting. The FDA indicates that Y90 is approved for the treatment of unresectable metastatic liver tumors from primary colorectal cancer with adjuvant intrahepatic artery floxuridine (FUDR) chemotherapy.7 On the other hand, Medicaid may or may not reimburse, and consequently, the hospital should review their Medicaid fee schedule to determine the level of reimbursement. In the past, Y90 therapy has been reimbursed by Aetna, Anthem, Cigna, United Healthcare, Health Net, Humana, Oxford, and Blue Cross/Blue Shield.7
When using Y90 off label, it is paramount to adhere to standard coding rules, especially if reimbursed by Medicare. If appropriate listed codes exist, these should be used to describe the procedure. On the other hand, if no appropriate codes exist, use “not otherwise classified or unlisted” procedure codes. The interventional radiologist should also submit supporting clinical documentation explaining medical necessity of the off-label use.
Conclusion
The addition of Y90 radioembolization to the arsenal of the interventional radiologist has created a unique set of challenges to proper reimbursement. A more comprehensive initial evaluation and clinical management, documentation of treatment planning, radiation dosimetry calculations, and administration of radioactive sources are unfamiliar territory that requires clear and precise documentation. An understanding of radioembolization coding will allow interventional radiologists to provide improved documentation, leading to more efficient treatment authorization and optimum reimbursement.
Editor’s note: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript received April 20, 2016; manuscript accepted June 29, 2016.
Address for correspondence: Amanjit S. Baadh, MD, Rush University Department of Radiology, 1653 W Congress Pkwy, Chicago, IL 60612, United States. Email: andybaadh@yahoo.com.
Suggested citation: Chopra R, Hoffman JC, Baadh AS. Optimizing reimbursement for radioembolization: the importance of adequate documentation. Intervent Oncol 360. 2016;4(8):E136-E142.
References
- Gates VL, Atassi B, Lewandowski RJ, et al. Radioembolization with Yttrium-90 microspheres: review of an emerging treatment for liver tumors. Future Oncol. 2007;3(1):73-81.
- Mahnken AH, Spreafico C, Maleux G, Helmberger T, Jakobs TF. Standards of practice in transarterial radioembolization. Cardiovasc Intervent Radiol. 2013;36(3):613-622.
- Giannini EG, Farinati F, Ciccarese F, et al; Italian Liver Cancer (ITA.LI.CA) group. Prognosis of untreated hepatocellular carcinoma. Hepatology. 2015;61(1):184-190.
- Liu DM, Cade DN, Knight J, et al. Yttrium-90 radioembolization. Endovasc Today. 2008 June. Available at: evtoday.com/pdfs/EVT0608_08.pdf
- Kallini JR, Gabr A, Salem R, Lewandowski RJ. Transarterial radioembolization with yttrium-90 for the treatment of hepatocellular carcinoma. Adv Ther. 2016;33(5):669-714.
- Sirtex. Coding sheet January 2016: pre-treatment mapping and microspheres administration: hospital outpatient, ASC and physician services. Available at: https://www.sirtex.com/media/70435/2016-sirtex-coding-sheet-updated032116-final.pdf
- Healthcare Administrative Partners. How to document y-90 radioembolization cases to maximize reimbursement. Available at: https://info.hapusa.com/Blog/bid/72834/How-to-Document-Y-90-Radioembolization-Cases-to-Maximize-Reimbursement

