


The Importance of Embolic Material and Artery Selection During Transarterial Chemoembolization of Hepatocellular Carcinoma
Abstract: The embolization technique and materials used for transarterial chemoembolization (TACE) vary widely and are often chosen on a case-by-case basis. A combination of factors, most importantly the size and location of the tumor(s), determine which materials and technique are best. It has been observed that 2 major factors affecting tumor response are the arterial selectivity and embolic particle size: more selective embolization and smaller particles each result in greater tumor necrosis. We present the case of a 57-year-old male with 2 hepatocellular carcinoma (HCC) tumors in the right hepatic lobe. This patient was initially treated with complete right lobar TACE and experienced an incomplete radiologic response. Repeat treatment with more selective arterial embolization and smaller particles resulted in a complete response. This case provides a useful example of an improved outcome using superselective embolization with smaller microparticles.
Key words: Hepatocellular carcinoma, transarterial chemoembolization, superselective catheterization
________________________
A 57-year-old male was referred to our department for transarterial chemoembolization of hepatocellular carcinoma. This patient first became known to us in 2011 during his initial workup for cirrhosis at the age of 55. His past medical history included cirrhosis status post liver transplant, hepatitis C, alcohol abuse, and rheumatic heart disease. He suffered from recurrent ascites requiring paracentesis, hepatic encephalopathy, esophageal varices, and pancytopenia presumably due to splenomegaly. Relevant labs included AST 56, ALT 22, total bilirubin 1.98, albumin 2.7, WBC 1.7, Hgb 8.6, platelets 74, INR 1.48. The patient’s alpha fetoprotein level was normal.
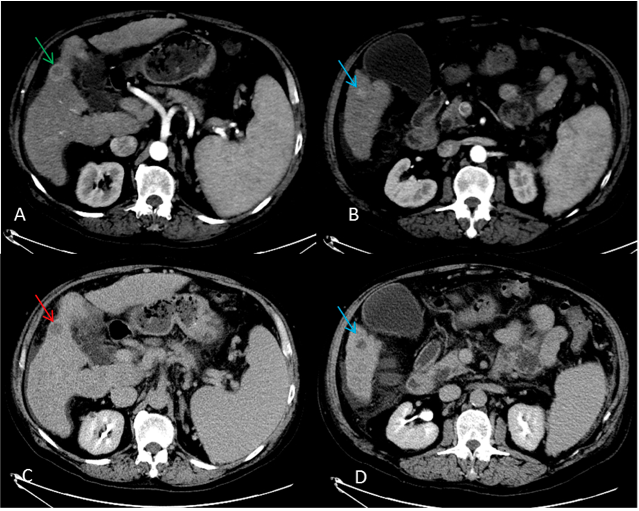 The patient underwent screening for HCC using computed tomography (CT) with triple phase liver protocol. His first 2 examinations, in May and August of 2011, demonstrated hepatic cirrhosis and sequelae of portal hypertension, but they were negative for HCC. Subsequent screening on July 21, 2012 and October 4, 2012 identified a right hepatic lobe (segment V) tumor measuring 2.5 cm, with an enhancement pattern characteristic of HCC (Figure 1. Axial arterial [A, B] and delayed [C, D] phase images from a July 21, 2012, computed tomography examination demonstrate a 2.5 cm segment V lesion with peripheral arterial phase and capsule enhancement (green arrow) and delayed phase wash-out [red arrow]. A second arterially enhancing segment V lesion located more inferiorly was also suspicious for HCC [blue arrows].). A second 1.7 cm segment V lesion that was not as well defined demonstrated nodular peripheral arterial enhancement that was also suspicious. Given the patient’s disease burden and performance status, the decision was made to manage the patient using transarterial chemoembolization (TACE).
The patient underwent screening for HCC using computed tomography (CT) with triple phase liver protocol. His first 2 examinations, in May and August of 2011, demonstrated hepatic cirrhosis and sequelae of portal hypertension, but they were negative for HCC. Subsequent screening on July 21, 2012 and October 4, 2012 identified a right hepatic lobe (segment V) tumor measuring 2.5 cm, with an enhancement pattern characteristic of HCC (Figure 1. Axial arterial [A, B] and delayed [C, D] phase images from a July 21, 2012, computed tomography examination demonstrate a 2.5 cm segment V lesion with peripheral arterial phase and capsule enhancement (green arrow) and delayed phase wash-out [red arrow]. A second arterially enhancing segment V lesion located more inferiorly was also suspicious for HCC [blue arrows].). A second 1.7 cm segment V lesion that was not as well defined demonstrated nodular peripheral arterial enhancement that was also suspicious. Given the patient’s disease burden and performance status, the decision was made to manage the patient using transarterial chemoembolization (TACE).
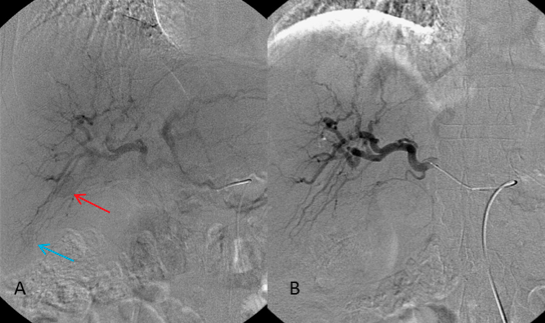 The patient was brought to the interventional department on October 8, 2012, four days after his second positive screening study. Right common femoral access was obtained and arteriography of the superior mesenteric artery (SMA) and celiac arteries was performed using a C2 catheter. The portal vein was confirmed to be patent with normal hepatopetal blood flow. A microcatheter was subsequently advanced into the right hepatic artery just beyond the origin of the cystic artery. Arteriography at this level demonstrated arterial blush in the region of the main segment V lesion (Figure 2. Anteroposterior images from an angiogram [A] and right hepatic lobar embolization [B] performed October 8, 2012. A small, faint arterial blush [red arrow] within hepatic segment V corresponds to one of the two lesions seen on computed tomography. A second blush, not as well seen, was felt to represent the second, more inferiorly located lesion [blue arrow].). A second, less well defined blush was thought to represent the second tumor. Embolization was performed from this location using one vial of 100-300 um LC Beads (BTG) drug-eluting beads (DEB) loaded with 75 mg of doxorubicin. After this vial was injected, persistent blood flow to the right hepatic artery was observed, so further embolization with 80% of one vial of 300-500 um Embospheres (Merit Medical) was performed. The embolization was terminated when near stasis was achieved. The patient tolerated the procedure without complication.
The patient was brought to the interventional department on October 8, 2012, four days after his second positive screening study. Right common femoral access was obtained and arteriography of the superior mesenteric artery (SMA) and celiac arteries was performed using a C2 catheter. The portal vein was confirmed to be patent with normal hepatopetal blood flow. A microcatheter was subsequently advanced into the right hepatic artery just beyond the origin of the cystic artery. Arteriography at this level demonstrated arterial blush in the region of the main segment V lesion (Figure 2. Anteroposterior images from an angiogram [A] and right hepatic lobar embolization [B] performed October 8, 2012. A small, faint arterial blush [red arrow] within hepatic segment V corresponds to one of the two lesions seen on computed tomography. A second blush, not as well seen, was felt to represent the second, more inferiorly located lesion [blue arrow].). A second, less well defined blush was thought to represent the second tumor. Embolization was performed from this location using one vial of 100-300 um LC Beads (BTG) drug-eluting beads (DEB) loaded with 75 mg of doxorubicin. After this vial was injected, persistent blood flow to the right hepatic artery was observed, so further embolization with 80% of one vial of 300-500 um Embospheres (Merit Medical) was performed. The embolization was terminated when near stasis was achieved. The patient tolerated the procedure without complication.
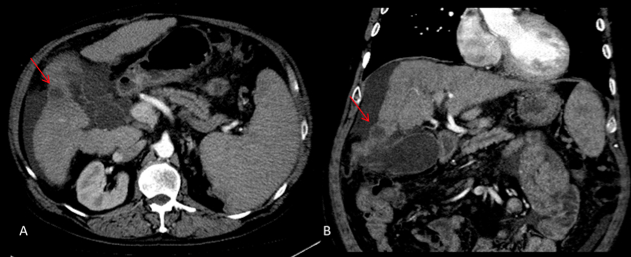
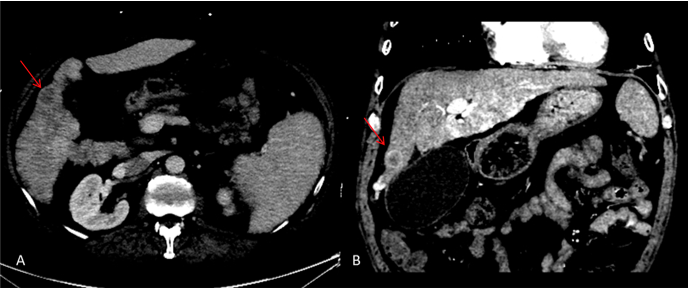 Follow-up CT performed on December 4, 2012 identified persistent arterial phase enhancement and delayed phase washout of the main segment V tumor, raising concern for residual HCC (Figure 3. Axial [A] and coronal [B] arterial phase images from a computed tomography examination performed December 4, 2012, demonstrating residual peripheral arterial phase enhancement around the segment V lesion, suspicious for residual or recurrent hepatocellular carcinoma [arrows]. The more inferiorly located lesions that was seen previously is not identified on this examination.). The patient returned to our department on February 13, 2013 for repeat TACE.
Follow-up CT performed on December 4, 2012 identified persistent arterial phase enhancement and delayed phase washout of the main segment V tumor, raising concern for residual HCC (Figure 3. Axial [A] and coronal [B] arterial phase images from a computed tomography examination performed December 4, 2012, demonstrating residual peripheral arterial phase enhancement around the segment V lesion, suspicious for residual or recurrent hepatocellular carcinoma [arrows]. The more inferiorly located lesions that was seen previously is not identified on this examination.). The patient returned to our department on February 13, 2013 for repeat TACE.
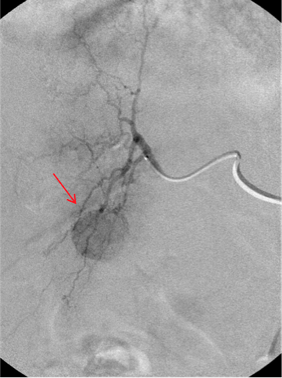 After obtaining right common femoral access and confirming portal venous patency, the segment V hepatic artery was selected. Arteriography demonstrated that the anterior branch of this vessel supplied a portion of the residual tumor (Figure 4. Repeat hepatic angiography was performed on February 13, 2013, with superselective embolization of hepatic segment V. A well-defined arterial blush [arrow] outlines the segment V lesion, which was identified by the follow-up computed tomography [arrow]. The second lesion is not identified.). Superselective embolization of this anterior branch was performed using 90% of one vial of 70-150 um LC Beads loaded with 75 mg doxorubicin. Near stasis was achieved. The target lesion demonstrated intense angiographic uptake of contrast and embolization material. Postembolization arteriography demonstrated preserved flow within the posterior branch of the segment V artery. The patient tolerated the procedure without complication.
After obtaining right common femoral access and confirming portal venous patency, the segment V hepatic artery was selected. Arteriography demonstrated that the anterior branch of this vessel supplied a portion of the residual tumor (Figure 4. Repeat hepatic angiography was performed on February 13, 2013, with superselective embolization of hepatic segment V. A well-defined arterial blush [arrow] outlines the segment V lesion, which was identified by the follow-up computed tomography [arrow]. The second lesion is not identified.). Superselective embolization of this anterior branch was performed using 90% of one vial of 70-150 um LC Beads loaded with 75 mg doxorubicin. Near stasis was achieved. The target lesion demonstrated intense angiographic uptake of contrast and embolization material. Postembolization arteriography demonstrated preserved flow within the posterior branch of the segment V artery. The patient tolerated the procedure without complication.
 Computed tomography on April 1, 2013 demonstrated that the tumors were now hypoattenuating without any evidence of enhancement (Figure 5. Axial [A] and coronal [B] computed tomography images from a study performed April 1, 2013. No residual arterial phase enhancement is seen within the previously described tumors [red arrows].), consistent with a complete tumor response to therapy based on the European Association for the Study of Liver (EASL) criteria.1 The patient underwent liver transplant on October 5, 2014. Pathologic examination of the native liver revealed a single moderately to poorly defined HCC tumor. Although the patient did well postoperatively, he was admitted to the hospital briefly on March 24, 2015, with elevated LFTs. Biopsy of the transplant liver showed mild acute cellular rejection. This was treated with high dose Solu-Medrol with good response. The patient remains in good condition. His most recent CT scan dated May 24, 2015 demonstrated no evidence of parenchymal, biliary, or vascular complication.
Computed tomography on April 1, 2013 demonstrated that the tumors were now hypoattenuating without any evidence of enhancement (Figure 5. Axial [A] and coronal [B] computed tomography images from a study performed April 1, 2013. No residual arterial phase enhancement is seen within the previously described tumors [red arrows].), consistent with a complete tumor response to therapy based on the European Association for the Study of Liver (EASL) criteria.1 The patient underwent liver transplant on October 5, 2014. Pathologic examination of the native liver revealed a single moderately to poorly defined HCC tumor. Although the patient did well postoperatively, he was admitted to the hospital briefly on March 24, 2015, with elevated LFTs. Biopsy of the transplant liver showed mild acute cellular rejection. This was treated with high dose Solu-Medrol with good response. The patient remains in good condition. His most recent CT scan dated May 24, 2015 demonstrated no evidence of parenchymal, biliary, or vascular complication.
Discussion
Transarterial therapies have dramatically altered the management of patients with inoperable liver cancer, particularly intermediate stage hepatocellular carcinoma (HCC). Transarterial chemoembolization (TACE) is the currently recommended therapy for this category of patients, according to the American Association for the Study of Liver Diseases guidelines.2 However, disagreement between interventional oncologists regarding the optimal TACE technique has prevented standardization of this important therapy.
Conventional TACE consisted of injection of a lipiodol/doxorubicin mixture followed by an embolic agent, commonly gelfoam, and was shown in early studies to both confer a strong antitumor effect as well as a survival advantage.3 This technique is now considered to be inferior due to the limited duration of embolization associated with gelfoam. Newer techniques utilizing DEB as the embolic material have evolved. Advantages of DEB include higher, more sustained release of chemotherapy into the tumor, with minimal systemic plasma concentration.4 Clinical trials have confirmed these advantages.5,6 Investigation into differences in patient outcomes between conventional and DEB TACE is ongoing.
Aside from the choice of embolic material, technical considerations in planning or performing TACE include the selectivity of arterial catheterization and the size of embolic particles. The establishment of TACE as the standard treatment for intermediate-grade HCC is based on a meta-analysis of six trials, several of which utilized whole-liver or lobar embolization.7 In this technique, embolization is performed with the catheter within the proper hepatic artery or lobar hepatic artery respectively. In contrast, most practitioners currently preferentially perform selective or superselective TACE, securing the embolization catheter as close to the tumor as possible.
There are two main reasons for the adoption of more selective embolization, both of which may seem obvious. First, embolizing as close as possible to the tumor is thought to result in concentration of the chemoembolic agent within the lesion and ensure maximum chemotherapeutic treatment. Second, more selective embolization results in preservation of arterial blood supply to as much of the functional liver tissue as possible. This strategy decreases one of the main side effects of TACE, which is precipitation or exacerbation of liver failure.
Small studies have shown that selective and superselective TACE result in higher rates of histologic tumor necrosis than lobar TACE.8,9 One of these studies demonstrated a trend toward improved 5-year disease-free survival in patients with a single nodule less than or equal to 5 cm treated with superselective compared with lobar technique, although this finding was not statistically significant.9 A trend toward improved survival was also observed in patients who achieved complete tumor necrosis compared with those with partial necrosis. The results from another prospective study of 118 patients suggest that patients with small (<5 cm) HCC lesions treated with selective/superselective TACE require repeat treatment less frequently than those treated with lobar TACE.8
These are small, nonrandomized studies, and therefore more investigation into tumor response and clinical outcomes after superselective vs lobar TACE is required. It is clear that lobar TACE must be performed in cases of multiple nodules in the same lobe or when superselective catheterization is not technically feasible due to anatomic considerations. However, using selective or superselective catheterization is considered to be superior, when these techniques are possible.
As described above, the case we have presented included the use of smaller embolization particles during the patient’s second treatment. Therefore, the choice of microparticle size deserves mention. The use of smaller beads is considered to confer a stronger antitumor effect due to greater blockade of terminal tumor vessels and delivery of chemotherapeutic agent to the tissue. Supporting this theory, one animal study demonstrated that the use of smaller particles causes greater tumor necrosis.10
The choice of particle size must be made on a case-by-case basis. The use of smaller particles has been associated with fatal pulmonary embolism in rare cases.11 Therefore, although the arteriole and tumor capillary bed will typically act as a filter, all attempts must be made to identify the presence of a hepatic arterial-systemic venous shunt prior to embolization. If systemic draining veins to the tumor are identified angiographically, larger particles or a different embolic agent should be used. Furthermore, some authors suggest the use of larger particles in patients with very large tumors (>10 cm), and in ones where the tumor is in close proximity to the diaphragm.11
Conclusion
TACE is an important therapy for patients with intermediate-grade HCC. However, a standard technique has yet to be established, and current techniques vary between institutions and individual patients. In general, when possible, superselective TACE is considered to be superior compared with lobar or whole-liver TACE, both in terms of tumor necrosis as well as preserving functional liver tissue. These findings are supported by small studies. The use of smaller microparticles is also considered to cause greater tumor necrosis, which has also been shown in animal models. The case presented here provides an example in which superselective embolization with smaller microparticles resulted in a superior radiologic outcome.
Editor’s note: Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no related disclosures.
Manuscript received June 6, 2015; manuscript accepted July 15, 2015.
Suggested citation: Storace M, White J, Bianco B. The importance of embolic material and artery selection during transarterial chemoembolization of hepatocellular carcinoma. Intervent Oncol 360. 2015;3(9):E101-E107.
References
1. Bruix J, Sherman M, Llovet JM, et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. J Hepatol. 2001;35(3):421–430.
2. Bruix J, Sherman M; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020-1022.
3. Llovet JM, Bruix J. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomized controlled trial. Lancet. 2002;359(9319):1734-1739.
4. Lee KH, Liapi E, Cornell C, et al. Doxorubicin-Loaded QuadraSphere microspheres: plasma pharmacokinetics and intratumoral drug concentration in an animal model of liver cancer. Cardiovasc Intervent Radiol. 2010;33(3):576-582.
5. Lammer J, Malgari K, Vogl T, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Intervent Radiol. 2010;33(1):41-52.
6. Song MJ, Chun HJ, Song do S, et al. Comparative study between doxorubicin-eluting beads and conventional transarterial chemoembolization for treatment of hepatocellular carcinoma. J Hepatol. 2012;57(6):1244-1250.
7. Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003;37(2):429-442.
8. Golfieri R, Cappelli A, Cucchetti A. Efficacy of selective transarterial chemoembolization in inducing tumor necrosis in small (<5 cm) hepatocellular carcinomas. Hepatology. 2011:53(5):1580-1589.
9. Dharancy S, Boitard J, Decaens T, et al. Comparison of two techniques of transarterial chemoembolization before liver transplantation for hepatocellular carcinoma: a case-control study. Liver Transpl. 2007;13(5):665-671.
10. Lewis AL, Taylor RR, Stratford PW, Gonzalez MV, Willis SL, Stratford PW. Pharmacokinetic and safety study of doxorubicin-eluting beads in a porcine model of hepatic arterial embolization. J Vasc Interv Radiol. 2006;17(8):1335-1345.
11. Brown KT. Fatal pulmonary complications after arterial embolization with 40-120 micrometer tris-acryl gelatin microspheres. J Vasc Intervent Radiol. 2004;15(8):887-888.
