


ADVERTISEMENT
Carbon Dioxide Imaging in Interventional Oncology: Preserving Renal Function and Providing Potentially Lifesaving Procedures to Previously Precluded Patients
Carbon dioxide has been used as an imaging contrast agent since the early 1900s. Its use has proliferated in a variety of clinical scenarios secondary to its unique properties combined with advancements in technology. Additionally, when used appropriately, it is extremely safe. A cursory examination of the literature comparing articles regarding complications of iodinated contrast or CO2 demonstrates a vast disparity with very few complications from intravascular use of CO2. For more specific information, a comprehensive review of CO2 angiography has just been published.1
There are many procedures in which CO2 can be used alone or in conjunction with iodinated contrasts. These include detection of acute hemorrhage, presence of contrast allergy, portal vein visualization, and venography. The principal advantage is its lack of nephrotoxicity. Many interventional procedures require a significant volume of iodinated contrast. We know from the literature that contrast-induced nephropathy (CIN) has been reported as the 2nd or 3rd leading cause of hospital-acquired renal failure.2 The incidence of hospital-acquired contrast-induced nephropathy approximates 7%.3
The significance of CIN was reported by McCullough.4 When he compared those individuals who developed hospital-acquired CIN to those who received contrast and maintained a stable creatinine, those with CIN had 5.5 times the incidence (34%) of in-hospital mortality. Those patients who required dialysis had higher mortality rates. Furthermore, the duration of hospitalization was twice those without CIN and was accompanied by increased morbidity and cost. Increased mortality was also delayed and the 1- and 2-year mortality was doubled.
In a retrospective analysis by Rihal et al of approximately 7,500 in-hospital patients, mortality was 22% for the 3.3% of patients who developed CIN, whereas the in-hospital mortality was 1.4% for patients who did not develop CIN. The 1- and 5-year mortality rates were almost 4 times greater in the CIN group.5
The incidence of CIN relates to underlying renal insufficiency, site of injection, and volume of contrast. The major variable in this is volume of contrast. Many medical adjuncts have been used unsuccessfully in an attempt to protect the kidney, but aside from hydration, these have been relatively ineffective. It seems obvious that the most efficacious way to prevent CIN is to reduce the volume of iodinated contrast.
Use of CO2 for Interventional Oncology
Many patients requiring interventional oncologic procedures receive a significant amount of contrast. Most of the time this is for vascular interrogation and follow-up. In addition, many of these patients are older and have a number of comorbidities including diabetes, renal insufficiency, hypertension, vascular disease, and liver failure. Additionally, these patients commonly function with hypovolemia because of poor hydration or occult bleeding. This is exacerbated if a patient develops postembolization syndrome and decreases intake due to nausea and vomiting. If NSAIDS or other medications that can be toxic to the kidneys are prescribed, the patient becomes predisposed to additional renal insult regardless of their underlying renal function. To underscore this potential situation is the performance of transhepatic arterial chemoembolization (TACE) for hepatocellular carcinoma. There are at least 3 studies that demonstrate acute renal failure (ARF) post TACE.6-8 To summarize these, there is a 3% to 8% incidence of ARF post chemoembolization with and without renal insufficiency. Acute renal failure was directly correlated with a number of procedures, diabetes, creatinine ≥1.5, and ascites.
The advantages of CO2 in this and other interventional oncologic procedures are many. The most obvious and beneficial is the decreased utilization of iodinated contrast. That is, of course, if there is appropriate visualization. As a vascular imaging agent, CO2 may occasionally fall short in visualization of large structures because it has to displace all of the blood in the vessel to render an accurate image. Fortunately, because of the ability to  displace blood in smaller vessels, CO2 demonstrates close to a one-to-one comparison with contrast when the vessels are 10 mm or less (Figure 1). This includes most of the vessels that need to be visualized in oncologic procedures.
displace blood in smaller vessels, CO2 demonstrates close to a one-to-one comparison with contrast when the vessels are 10 mm or less (Figure 1). This includes most of the vessels that need to be visualized in oncologic procedures.
Most interventionalists use microcatheters because of their many advantages in negotiating peripherally reducing spasm and allowing flow. One small disadvantage of microcatheters is the inability or difficulty injecting diagnostic amounts of iodinated contrast. This is easily remedied with CO2, which has a viscosity that is 1/400 that of iodinated contrast. It can be injected with ease and demonstrates not only peripheral but central anatomy (Figure 2). Central demonstration is key in certain situations. If you are unsure of your catheter placement, giving contrast will only demonstrate the anatomy distal to the catheter tip. Using CO2, the 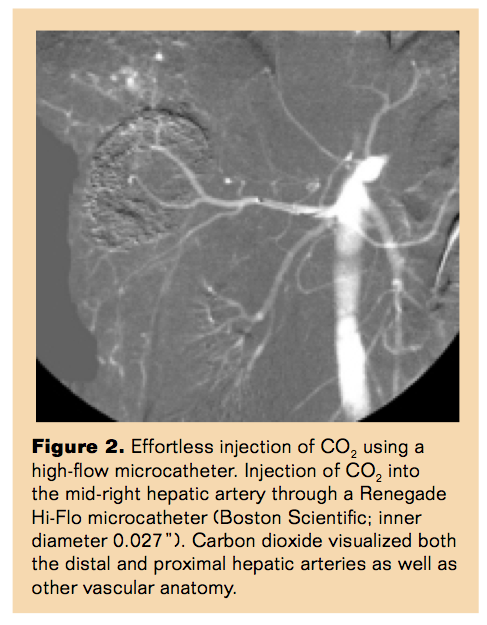 gas will reflux and demonstrate the peripheral and central anatomy. This may prevent nontarget embolization or unnecessary removal and replacement of the microcatheter.
gas will reflux and demonstrate the peripheral and central anatomy. This may prevent nontarget embolization or unnecessary removal and replacement of the microcatheter.
Furthermore, considering the low viscosity of CO2, we have used it for portal vein embolization for all the reasons above plus localization. Using a 22 gauge transhepatic needle, 10 cc to 20 cc of intraparenchymal CO2 can be administered and will opacify the portal vein. This allows for planning and radicle access in portal vein embolization (Figure 3).
Conclusion

In summary, CO2 vascular imaging can be used alone or as an adjunct to limit the volume of iodinated contrast in interventional oncologic procedures. Additional unique CO2 properties may also be useful to the operator. CO2 can not only prevent the sequelae of ARF and chronic renal failure and its ramifications, but more importantly, it can offer renal insufficiency patients the opportunity to have lifesaving or life-sparing procedures from which they would otherwise have been precluded.
References
- Caridi JG, Cho KJ, Fauria C, Eghbalieh N. Carbon dioxide digital subtraction angiography (CO2 DSA): a comprehensive user guide for all operators. Vasc Dis Manag. 2014;11(10):E221-E256.
- Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39(5):930-936.
- Bartholomew BA, Harjai KJ, Dukkipati S, et al. Impact of nephropathy after percutaneous coronary intervention and a method for risk stratification. Am J Cardiol. 2004;93(12):1515-1519.
- McCullough P. Contrast induced acute kidney injury. J Am Coll Cardiol. 2008;51(15):1419-1428.
- Rihal CS, Textor SC, Grill DE. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002;105(19):2259-2264.
- Huo TI, Wu JC, Lee PC, Chang FY, Lee SD. Incidence and risk factors for acute renal failure in patients with hepatocellular carcinoma undergoing transarterial chemoembolization: a prospective study. Liver Int. 2004;24(3):210-215.
- Jang BK, Lee SH, Chung WJ, et al. Incidence and risk factors of acute renal failure after transcatheter arterial chemoembolization for hepatocellular carcinoma. Korean J Hepatol. 2008;14(2):168-177.
- Yamazaki H, Oi H, Matsushita M, et al. Renal cortical retention on delayed CT and nephropathy following transcatheter arterial chemoembolisation. Br J Radiol. 2001;74(884):695-700.
_________________________________________
Editor’s note: Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr. Caridi reports that he serves as medical director at AngioAdvancements with potential future stock ownership.
Manuscript received December 16, 2014; manuscript accepted February 1, 2015.
Address for correspondence: James G. Caridi, MD, FSIR, Tulane University School of Medicine, Department of Radiology SL-54 1430, Tulane, LA 70112, United States. Email: jimcaridi@gmail.com
Suggested citation: Caridi JG. Carbon dioxide imaging in interventional oncology: preserving renal function and providing potentially lifesaving procedures to previously precluded patients. Intervent Oncol 360. 2015;3(4):E44-E47.

