


Novel Extreme Triple Telescopic Support for Percutaneous Coronary Intervention
 Since the first coronary angioplasty was performed in 1977, the field of interventional cardiology has grown tremendously. Ever more complex coronary lesions have been approached percutaneously with better and better results. Technological advances, new techniques, and the increasing individual as well as “collective” experience of the interventional cardiology community made cases thought to be impossible to treat with percutaneous coronary intervention (PCI) in the past, now successful. Usually, the more complex the PCI, the more guide catheter (GC) support is required for success.
Since the first coronary angioplasty was performed in 1977, the field of interventional cardiology has grown tremendously. Ever more complex coronary lesions have been approached percutaneously with better and better results. Technological advances, new techniques, and the increasing individual as well as “collective” experience of the interventional cardiology community made cases thought to be impossible to treat with percutaneous coronary intervention (PCI) in the past, now successful. Usually, the more complex the PCI, the more guide catheter (GC) support is required for success.
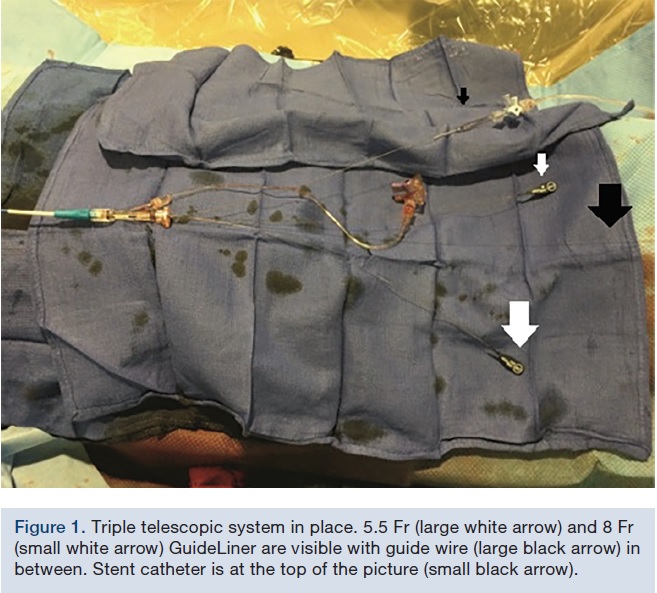
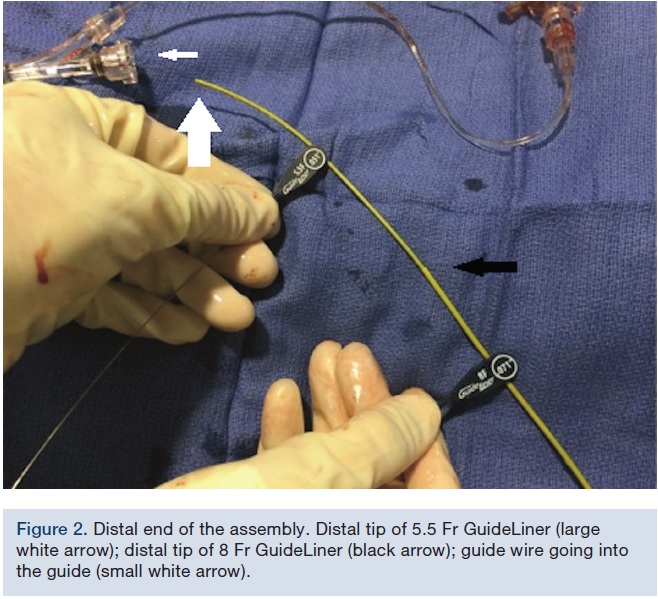 Every interventionalist will eventually face a situation when even what is considered very good support is insufficient for completing PCI. Here, we present a novel technique of extreme PCI support, as depicted in our case series, which allowed completion of PCI otherwise not possible by using conventional means. We describe a triple telescopic system, involving a smaller in a larger GuideLiner catheter (Vascular Solutions) in a large guide catheter (Figures 1-2).
Every interventionalist will eventually face a situation when even what is considered very good support is insufficient for completing PCI. Here, we present a novel technique of extreme PCI support, as depicted in our case series, which allowed completion of PCI otherwise not possible by using conventional means. We describe a triple telescopic system, involving a smaller in a larger GuideLiner catheter (Vascular Solutions) in a large guide catheter (Figures 1-2).
Case 1
 An 81-year-old female continued to experience effort angina with activities of daily living in spite of optimal medical therapy. She had a PCI of her left anterior descending artery (LAD) and obtuse marginal branch (OM) 7 years prior. Medications included aspirin, metoprolol, amlodipine, rosuvastatin, furosemide, and sublingual nitroglycerine. Cardiovascular examination was unremarkable except for a grade 2/6 systolic murmur at the left sternal border, radiating to the carotid arteries. Electrocardiogram (EKG) showed sinus rhythm with first-degree atrioventricular block. An echocardiogram revealed preserved left ventricular function with mild aortic stenosis. Coronary angiogram showed patent stents and mild non-obstructive disease in the left system. A large, severely tortuous, fully calcified right coronary artery (RCA) was noted to have a 90% distal stenosis followed by a 70% lesion (Figure 3).
An 81-year-old female continued to experience effort angina with activities of daily living in spite of optimal medical therapy. She had a PCI of her left anterior descending artery (LAD) and obtuse marginal branch (OM) 7 years prior. Medications included aspirin, metoprolol, amlodipine, rosuvastatin, furosemide, and sublingual nitroglycerine. Cardiovascular examination was unremarkable except for a grade 2/6 systolic murmur at the left sternal border, radiating to the carotid arteries. Electrocardiogram (EKG) showed sinus rhythm with first-degree atrioventricular block. An echocardiogram revealed preserved left ventricular function with mild aortic stenosis. Coronary angiogram showed patent stents and mild non-obstructive disease in the left system. A large, severely tortuous, fully calcified right coronary artery (RCA) was noted to have a 90% distal stenosis followed by a 70% lesion (Figure 3). 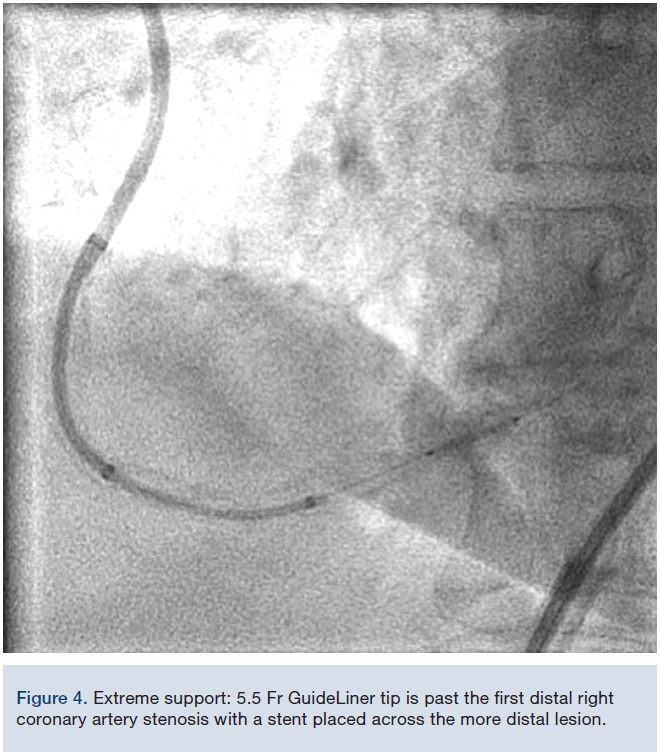 Given the tortuosity and calcification, very good catheter support was needed for PCI. An 8 French (Fr), 45 cm sheath was inserted into the femoral artery and an 8 Fr multipurpose guide catheter was chosen. After deep intubation of the RCA with the guide catheter, a Balance Middleweight guide wire (BMW) (Medtronic) was used to cross the lesion; however, just as the BMW crossed, the guide catheter prolapsed back into the aorta. At this point, an 8 Fr GuideLiner was inserted into the guide catheter with a 5.5 Fr GuideLiner inserted into it (outside the patient) over a BMW (Figures 1-2). This system was advanced into the RCA with the guide catheter deeply seated. The 8 Fr GuideLiner tip was advanced to the mid RCA and the 5.5 Fr GuideLiner tip reached mid vessel. With this support system, both stenoses were predilated with a 2.5 x 15 mm non-compliant balloon. First, a 3.5 x 12 mm Xience stent (Abbott Vascular) was placed in the distal coronary lesion, which required pushing of the 5.5 Fr GuideLiner further into the distal vessel, past the first lesion (Figure 4). Next, a 4.0 x 28 mm Xience stent was advanced to the distal tip of the 5.5 Fr GuideLiner and it was “de-sheathed” by pulling the GuideLiner back. With a good final result, the patient was discharged home the following day in good condition and remained angina free.
Given the tortuosity and calcification, very good catheter support was needed for PCI. An 8 French (Fr), 45 cm sheath was inserted into the femoral artery and an 8 Fr multipurpose guide catheter was chosen. After deep intubation of the RCA with the guide catheter, a Balance Middleweight guide wire (BMW) (Medtronic) was used to cross the lesion; however, just as the BMW crossed, the guide catheter prolapsed back into the aorta. At this point, an 8 Fr GuideLiner was inserted into the guide catheter with a 5.5 Fr GuideLiner inserted into it (outside the patient) over a BMW (Figures 1-2). This system was advanced into the RCA with the guide catheter deeply seated. The 8 Fr GuideLiner tip was advanced to the mid RCA and the 5.5 Fr GuideLiner tip reached mid vessel. With this support system, both stenoses were predilated with a 2.5 x 15 mm non-compliant balloon. First, a 3.5 x 12 mm Xience stent (Abbott Vascular) was placed in the distal coronary lesion, which required pushing of the 5.5 Fr GuideLiner further into the distal vessel, past the first lesion (Figure 4). Next, a 4.0 x 28 mm Xience stent was advanced to the distal tip of the 5.5 Fr GuideLiner and it was “de-sheathed” by pulling the GuideLiner back. With a good final result, the patient was discharged home the following day in good condition and remained angina free.
Case 2
 A 78-year-old male with a history of hypertension, hyperlipidemia, and coronary artery disease (CAD) presented to the office with complaints of severe fatigue and dyspnea on exertion. Patient underwent coronary artery bypass surgery 4 years ago. His left internal mammary artery was anastomosed to the diagonal branch, with 2 vein grafts anastomosed to the LAD and OM. The RCA was not bypassed, but was known to be a chronic total occlusion (CTO). The patient was treated with aspirin, amlodipine, isosorbide, simvastatin, and lisinopril. Cardiovascular exam was unremarkable. An echocardiogram showed a left ventricular ejection fraction of 40%. An EKG was normal. Angiography showed a 40% distal left main artery stenosis,
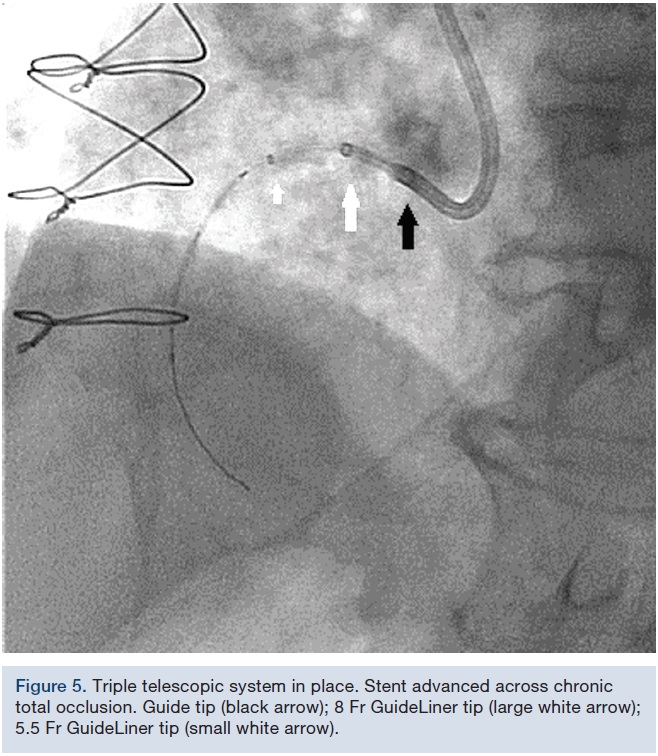
A 78-year-old male with a history of hypertension, hyperlipidemia, and coronary artery disease (CAD) presented to the office with complaints of severe fatigue and dyspnea on exertion. Patient underwent coronary artery bypass surgery 4 years ago. His left internal mammary artery was anastomosed to the diagonal branch, with 2 vein grafts anastomosed to the LAD and OM. The RCA was not bypassed, but was known to be a chronic total occlusion (CTO). The patient was treated with aspirin, amlodipine, isosorbide, simvastatin, and lisinopril. Cardiovascular exam was unremarkable. An echocardiogram showed a left ventricular ejection fraction of 40%. An EKG was normal. Angiography showed a 40% distal left main artery stenosis, 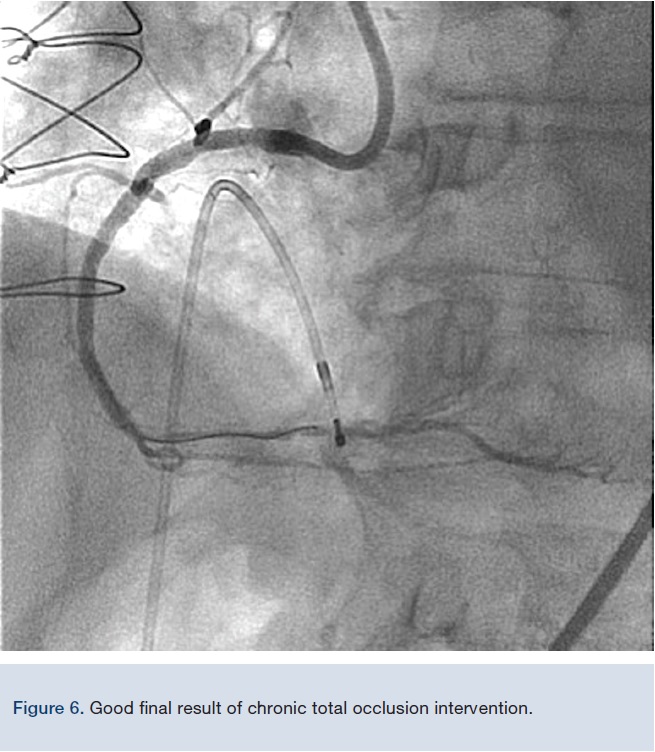 proximal 100% occlusion of the LAD, and 70% proximal stenosis of the OM. All bypass grafts were patent. CTO PCI of the RCA was begun with an 8 Fr, 45 cm sheath via the femoral artery and Amplatz left 0.75 8 Fr guide catheter. A Pilot 200 guidewire (Abbott Vascular) was used to traverse the proximal cap and MiracleBros 6 wire (Asahi Intecc) was needed for distal cap crossing. An attempt at crossing the proximal cap with a small balloon was unsuccessful due to inadequate support. A similar telescopic system was used, as described in Case 1. Once an 8 Fr GuideLiner with a 6 Fr GuideLiner extension was inserted into the proximal RCA, the balloon crossing was relatively easy (Figure 5). PCI was concluded with a good result (Figure 6) and the patient was asymptomatic afterwards.
proximal 100% occlusion of the LAD, and 70% proximal stenosis of the OM. All bypass grafts were patent. CTO PCI of the RCA was begun with an 8 Fr, 45 cm sheath via the femoral artery and Amplatz left 0.75 8 Fr guide catheter. A Pilot 200 guidewire (Abbott Vascular) was used to traverse the proximal cap and MiracleBros 6 wire (Asahi Intecc) was needed for distal cap crossing. An attempt at crossing the proximal cap with a small balloon was unsuccessful due to inadequate support. A similar telescopic system was used, as described in Case 1. Once an 8 Fr GuideLiner with a 6 Fr GuideLiner extension was inserted into the proximal RCA, the balloon crossing was relatively easy (Figure 5). PCI was concluded with a good result (Figure 6) and the patient was asymptomatic afterwards.
Case 3
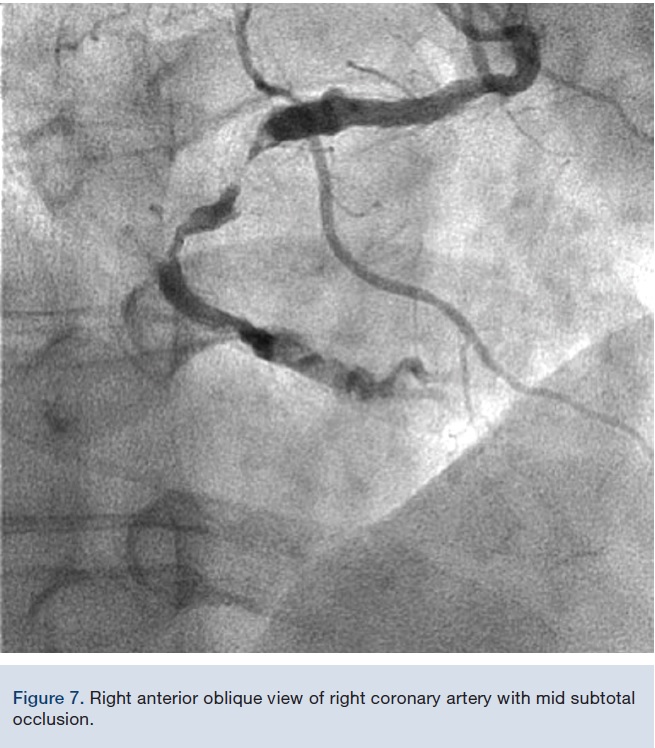 A 58-year-old male presented for cardiac evaluation prior to renal transplantation. He complained of dyspnea on exertion and fatigue. He had a history of hypertension, hyperlipidemia, diabetes mellitus, end-stage renal disease and stroke. Medications included aspirin, diltiazem, carvedilol, atorvastatin and losartan. Cardiovascular exam was unremarkable. An echocardiogram showed normal left ventricular systolic function. An EKG was normal. An exercise nuclear stress test was stopped in the 6th minute of standard Bruce protocol due to fatigue and dyspnea. In the inferolateral leads, 2 mm ST depressions were noted, with a myocardial perfusion study showing a medium-sized inferior infarct with peri-infarct ischemia. Coronary angiogram revealed mild to moderate disease in the left system. The RCA was dominant, with a 99% mid stenosis followed by a 60% distal lesion (Figure 7). Left to right collaterals were noted. The RCA was severely calcified and tortuous with a downward take-off ostium (Figure 7). An 8 Fr multipurpose guide catheter was inserted through a 45 cm, 8 Fr femoral sheath. A BMW wire tip would not progress beyond the mid lesion, with the guide catheter disengagement from the RCA ostium just by pushing the wire. At this point, a telescopic system utilizing an 8 Fr and a 5.5 Fr GuideLiner was assembled outside the patient and advanced to the mid RCA, as detailed above. The BMW wire could then be advanced to the distal vessel without difficulty. After pre-dilating the mid RCA with a noncompliant balloon, the 5.5 Fr GuideLiner was advanced over the balloon beyond this lesion. A 4 x 28 mm Xience stent was advanced and “desheathed” off the GuideLiner. After stent deployment, a good final result was obtained. The patient was discharged home the following day and he remains asymptomatic.
A 58-year-old male presented for cardiac evaluation prior to renal transplantation. He complained of dyspnea on exertion and fatigue. He had a history of hypertension, hyperlipidemia, diabetes mellitus, end-stage renal disease and stroke. Medications included aspirin, diltiazem, carvedilol, atorvastatin and losartan. Cardiovascular exam was unremarkable. An echocardiogram showed normal left ventricular systolic function. An EKG was normal. An exercise nuclear stress test was stopped in the 6th minute of standard Bruce protocol due to fatigue and dyspnea. In the inferolateral leads, 2 mm ST depressions were noted, with a myocardial perfusion study showing a medium-sized inferior infarct with peri-infarct ischemia. Coronary angiogram revealed mild to moderate disease in the left system. The RCA was dominant, with a 99% mid stenosis followed by a 60% distal lesion (Figure 7). Left to right collaterals were noted. The RCA was severely calcified and tortuous with a downward take-off ostium (Figure 7). An 8 Fr multipurpose guide catheter was inserted through a 45 cm, 8 Fr femoral sheath. A BMW wire tip would not progress beyond the mid lesion, with the guide catheter disengagement from the RCA ostium just by pushing the wire. At this point, a telescopic system utilizing an 8 Fr and a 5.5 Fr GuideLiner was assembled outside the patient and advanced to the mid RCA, as detailed above. The BMW wire could then be advanced to the distal vessel without difficulty. After pre-dilating the mid RCA with a noncompliant balloon, the 5.5 Fr GuideLiner was advanced over the balloon beyond this lesion. A 4 x 28 mm Xience stent was advanced and “desheathed” off the GuideLiner. After stent deployment, a good final result was obtained. The patient was discharged home the following day and he remains asymptomatic.
Discussion
Guide catheter support during complex PCI is the key determinant for successful completion of the procedure. Good support depends mainly on the guide catheter. A first step in improving support is using a larger lumen guide designed for extra support (i.e., Amplatz or Extra Back Up [EBU] curves). Sometimes it is not enough, even when extra support guidewire(s) are applied. In these cases, advanced techniques have been developed, including use of an “anchoring balloon”, deeper intubation of the coronary artery with a guide catheter, buddy wire techniques, a Tornus catheter (Asahi Intecc), or “armed guide catheter” technique, to name a few.1-3 A dedicated catheter for telescopic technique (the GuideLiner) received U.S. Food and Drug Administration (FDA) approval in 2009 and at least in some practices, revolutionized complex PCI.
The GuideLiner is a single-lumen, 145 cm device with a distal 20 cm catheter, with the remainder comprised of a stainless steel shaft. The distal part is soft, flexible, and straight. The GuideLiner is used as a “mother and child” system for extra support where deep intubation of a coronary artery is performed. It is available in 4 sizes, from 5.5 Fr up to 8 Fr. The GuideLiner has been used for other than the above purposes. Its use as a thrombectomy device or as a support device for guide catheter exchange over a coronary guide wire has been described.4,5
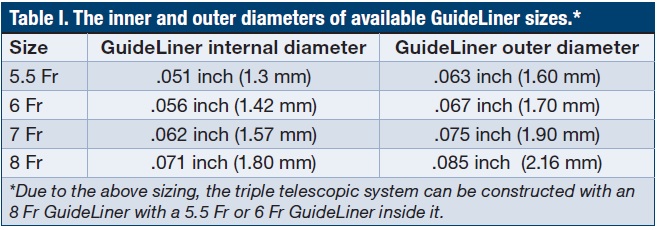 We took the telescopic technique one step further by creating a double GuideLiner system for even better support for PCI. The 5.5 Fr and 6 Fr GuideLiner fit into an 8 Fr GuideLiner, but not into a 7 Fr GuideLiner (Table I).6 Our triple telescopic guide support system has allowed us to complete complex PCIs of severely calcified and tortuous vessels, as well as a CTO, with relative ease, when more conventional techniques failed. We believe that this system is relatively safe, thanks to the “mother and child” GuideLiner catheters (soft tips) in the “grandmother” large guide. The system is easy to deploy (Figures 1-2) and can be used as a fallback technique, added during the case, without loss of guidewire position. This GuideLiner “generations” system is quite versatile, as support can be graded by simple extension of one or both GuideLiner catheters into the coronary artery, while guide catheter tip is parked at the ostium or is advanced over them for deep sitting. The smaller size GuideLiner can also be advanced past a predilated stenosis (“desheathing” stent) and stent delivery becomes even easier.
We took the telescopic technique one step further by creating a double GuideLiner system for even better support for PCI. The 5.5 Fr and 6 Fr GuideLiner fit into an 8 Fr GuideLiner, but not into a 7 Fr GuideLiner (Table I).6 Our triple telescopic guide support system has allowed us to complete complex PCIs of severely calcified and tortuous vessels, as well as a CTO, with relative ease, when more conventional techniques failed. We believe that this system is relatively safe, thanks to the “mother and child” GuideLiner catheters (soft tips) in the “grandmother” large guide. The system is easy to deploy (Figures 1-2) and can be used as a fallback technique, added during the case, without loss of guidewire position. This GuideLiner “generations” system is quite versatile, as support can be graded by simple extension of one or both GuideLiner catheters into the coronary artery, while guide catheter tip is parked at the ostium or is advanced over them for deep sitting. The smaller size GuideLiner can also be advanced past a predilated stenosis (“desheathing” stent) and stent delivery becomes even easier.
Any 8 Fr guide catheter can be used for this technique. A disadvantage of our system is the inability to place two guidewires and a stent in the 5.5 or 6 Fr GuideLiner (i.e., for bifurcation intervention). Also, this system requires, at the minimum, use of an 8 Fr guide catheter. An 8 Fr guide catheter also requires femoral artery access, as radial access cannot be used with a guide catheter of this size. A guide catheter of this size requires meticulous attention to arterial stick technique and longer bed rest after manual compression or stick site closure device. In our practice, we use manual compression as the primary method for hemostasis. Closure devices can be used based on local expertise and availability.
Conclusion
Our triple telescopic system constructed by adding a second GuideLiner catheter to a classical GuideLiner setup adds extreme support at a level difficult to equal with other techniques. We can complete complex cases relatively easily with this system that otherwise would be failures. While relatively safe, we recommend use of this system by operators experienced in GuideLiner classical techniques and when conventional methods are not successful. The technique cannot be used via the radial artery due to the size of the guide catheter and longer bed rest is needed after stick site control.
References
- Di Mario C, Ramasami N. Techniques to enhance guide catheter support. Catheter Cardiovasc Interv. 2008 Oct 1; 72(4): 505-512.
- Stys AT, Lawson W, Brown D. Extreme coronary guide catheter support: a case of a novel telescopic guide catheter system with a contralateral aortic wall support. J Invasive Cardiol. 2007 Apr; 19(4): E107-E110.
- Stys A, Lawson W, Brown D. Extreme coronary guide catheter support: Report of two cases of a novel telescopic guide catheter system. Catheter Cardiovasc Interv. 2006; 67: 908-911.
- Stys TP, Khan MA, Rajpurohit N, Stys AT. A new technique for coronary guide catheter exchange over coronary guidewire using GuideLiner catheter. J Invasive Cardiol. 2014 May; 26(5): E56-E58.
- Stys AT, Stys TP, Rajpurohit N, Khan MA. A novel application of GuideLiner catheter for thrombectomy in acute myocardial infarction: a case series. J Invasive Cardiol. 2013; 25(11): 620-624.
- GuideLiner V3 Catheter. Available online at https://vasc.com/flash/Catalogs/US/#16. Page 1. Accessed February 19, 2017.
The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Muhammad Khan, MD, at aleekhan@gmail.com.
