


Nitroglycerin Revisited: Update for the Cath Lab*
Recently I read an impressive cath lab study by Asrress et al on nitroglycerin (NTG) and its physiologic mechanisms of action to relieve exercise-induced ischemia in patients.1 The measurements of coronary translesional hemodynamics during bicycle exercise and how NTG relieved ischemia are unique, and prompted me to review what we know about NTG and share these insights with CLD readers.
Before discussing the new observations, we should recall that nitroglycerin is routinely administered sublingually, intravenously, or intra-arterially during coronary and left ventricular angiography. NTG produces significant coronary vasodilation, increasing vessel caliber and to a lesser extent, flow responses, and at the same time, reduces afterload (systemic arterial dilation) and preload due to venodilation. Practically speaking, both effects contribute to a reduction of left ventricular filling pressures (LVEDP).3,4 However, variable hemodynamic influences of nitroglycerin are reported during acute myocardial ischemia5,6 which may not be readily apparent in stable coronary artery disease patients.
Nitroglycerin Before LV Angiography
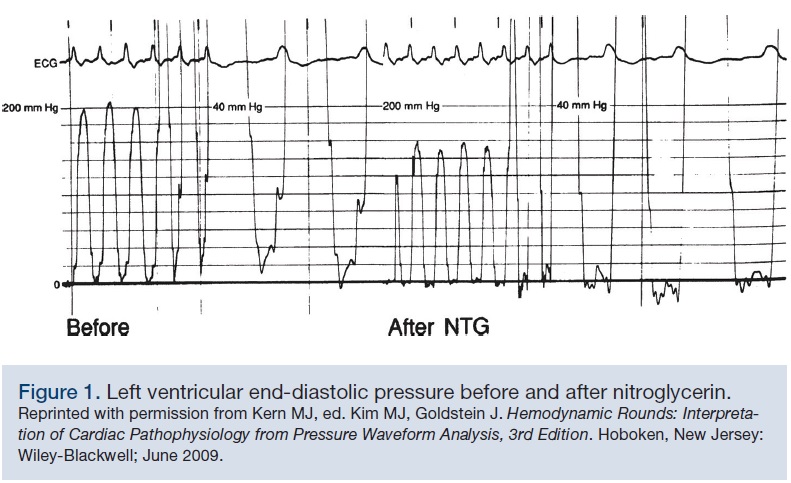 It is common practice to treat patients with high left ventricular end-diastolic pressure (LVEDP) with NTG prior to LV angiography. NTG helps unload the LV and increase the margin of safety, reducing the chance of inducing pulmonary edema with contrast injection and volume overload. An example of the effect of NTG on left ventricular hemodynamics is shown in Figure 1. LV systolic pressure is 200 mmHg and LVEDP is approximately 22 mmHg. Prior to contrast ventriculography, 0.4 mg sublingual nitroglycerin reduced the systolic pressure from 200 mmHg to 155 mmHg, and LVEDP was reduced to to approximately 2 mmHg. The decrease in LVEDP with vasodilators such as nitroglycerin (and sodium nitroprusside) is characterized by a downward shift in the left ventricular pressure volume relationship.5,6 At rest, nitrates routinely reduce left ventricular systolic pressure 10-15 mmHg, while reducing LV end-diastolic volume 25-30% and LV end-systolic volume 30-35%. During the ischemic stress of supine exercise, systemic nitroglycerin also produces a significant reduction in end-diastolic pressures and LV end-systolic volume in comparison to intracoronary nitrates.7 These findings appeared to support the conventional wisdom that preload reduction more than coronary dilation is the predominant anti-ischemic mechanism.
It is common practice to treat patients with high left ventricular end-diastolic pressure (LVEDP) with NTG prior to LV angiography. NTG helps unload the LV and increase the margin of safety, reducing the chance of inducing pulmonary edema with contrast injection and volume overload. An example of the effect of NTG on left ventricular hemodynamics is shown in Figure 1. LV systolic pressure is 200 mmHg and LVEDP is approximately 22 mmHg. Prior to contrast ventriculography, 0.4 mg sublingual nitroglycerin reduced the systolic pressure from 200 mmHg to 155 mmHg, and LVEDP was reduced to to approximately 2 mmHg. The decrease in LVEDP with vasodilators such as nitroglycerin (and sodium nitroprusside) is characterized by a downward shift in the left ventricular pressure volume relationship.5,6 At rest, nitrates routinely reduce left ventricular systolic pressure 10-15 mmHg, while reducing LV end-diastolic volume 25-30% and LV end-systolic volume 30-35%. During the ischemic stress of supine exercise, systemic nitroglycerin also produces a significant reduction in end-diastolic pressures and LV end-systolic volume in comparison to intracoronary nitrates.7 These findings appeared to support the conventional wisdom that preload reduction more than coronary dilation is the predominant anti-ischemic mechanism. Furthermore, high LVEDP (>30 mmHg) is associated with the development of accelerated angina and congestive heart failure in some patients. Common practice suggests that nitroglycerin should be routinely administered (either sublingual or systemically) for left ventricular end-diastolic pressures > 20 mmHg. However, and depending on the volume status of the individual, small doses of nitroglycerin can result in a significant decrease in LVEDP and hypotension. To maintain a satisfactory systemic pressure after ventriculography, fluid resuscitation may be needed to maintain an LVEDP of at least 5-10 mmHg. Routine administration of volume after nitroglycerin is not necessary, but the hypotensive effect of nitroglycerin can be used as an indicator of the volume status either following contrast-induced vasodilatation or later in the post-catheterization period, especially prior to percutaneous coronary intervention (PCI) and induction of ischemia during stenting.
NTG, LV Compliance and Volume
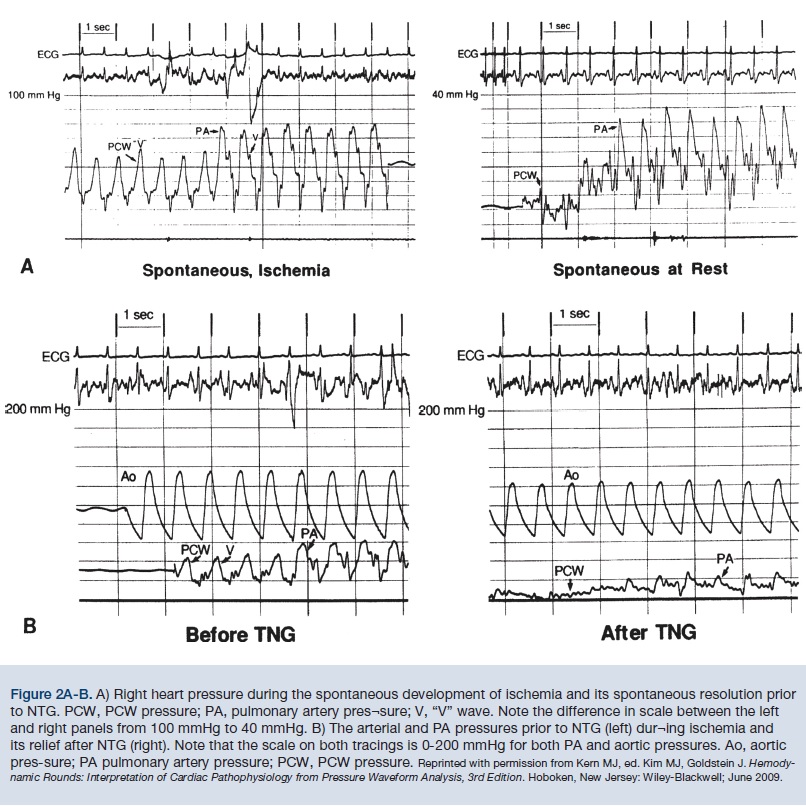 Ischemia changes the compliance of both the LV and left atrial (LA) chambers, often manifested by an increase in LVEDP, transient papillary muscle dysfunction, and mitral regurgitation, at times with large V waves. An example of the hemodynamics of ischemia and its response to NTG are shown by the tracings of a 61-yr-old woman with unstable angina. Right and left heart hemodynamic measurements were obtained before coronary angiography and ventriculography. During these measurements, the patient complained of her typical chest pain. Pulmonary capillary wedge (PCW) and pulmonary artery (PA) pressures were measured during and after spontaneous resolution of angina (Figure 2A, left). During spontaneous ischemia, a giant V wave is seen on the PCW (nearly 60 mmHg) with a mean of 35 mmHg. Before we could give NTG, chest pain spontaneously resolved, with dramatic changes in the PCW (Figure 2B). After relief of ischemia, PA pressure was 32/16 mmHg and the PCW mean was reduced to approximately 10 mmHg. A few minutes later, ischemia recurred (Figure 2B), aortic pressure was 138/64 mmHg, mean PCW pressure was 30 mmHg with V waves to 42 mmHg, and PA pressure was 60/20 mmHg. Within 3 minutes, NTG (0.4 mg sublingual) reduced aortic pressure (122/68 mmHg) and mean PCW to 6-8 mmHg without V waves, and PA pressure to 22/10 mmHg with complete relief of chest pain. The most striking difference between spontaneous and nitroglycerin-induced relief of ischemia is the dramatic preload reduction noted by the greater decline in mean PCW and PA pressures. Spontaneous resolution of ischemia causes less of a shift in the pressure-volume relationship of the LV than the nitroglycerin-induced reduction in ischemia.
Ischemia changes the compliance of both the LV and left atrial (LA) chambers, often manifested by an increase in LVEDP, transient papillary muscle dysfunction, and mitral regurgitation, at times with large V waves. An example of the hemodynamics of ischemia and its response to NTG are shown by the tracings of a 61-yr-old woman with unstable angina. Right and left heart hemodynamic measurements were obtained before coronary angiography and ventriculography. During these measurements, the patient complained of her typical chest pain. Pulmonary capillary wedge (PCW) and pulmonary artery (PA) pressures were measured during and after spontaneous resolution of angina (Figure 2A, left). During spontaneous ischemia, a giant V wave is seen on the PCW (nearly 60 mmHg) with a mean of 35 mmHg. Before we could give NTG, chest pain spontaneously resolved, with dramatic changes in the PCW (Figure 2B). After relief of ischemia, PA pressure was 32/16 mmHg and the PCW mean was reduced to approximately 10 mmHg. A few minutes later, ischemia recurred (Figure 2B), aortic pressure was 138/64 mmHg, mean PCW pressure was 30 mmHg with V waves to 42 mmHg, and PA pressure was 60/20 mmHg. Within 3 minutes, NTG (0.4 mg sublingual) reduced aortic pressure (122/68 mmHg) and mean PCW to 6-8 mmHg without V waves, and PA pressure to 22/10 mmHg with complete relief of chest pain. The most striking difference between spontaneous and nitroglycerin-induced relief of ischemia is the dramatic preload reduction noted by the greater decline in mean PCW and PA pressures. Spontaneous resolution of ischemia causes less of a shift in the pressure-volume relationship of the LV than the nitroglycerin-induced reduction in ischemia. Nitroglycerin, Angina, and Coronary Stenosis Hemodynamics
Sublingual nitroglycerin marginally improves coronary blood flow, but does more by reducing preload to relieve myocardial ischemia in patients with coronary artery disease.8 Nitrate-induced increase in coronary blood flow to ischemic myocardium through reversal of coronary vasoconstriction has been a controversial subject.5,6 Coronary blood flow responses are highly variable, as is the degree of coronary vasodilation related to the degree of endothelial function.
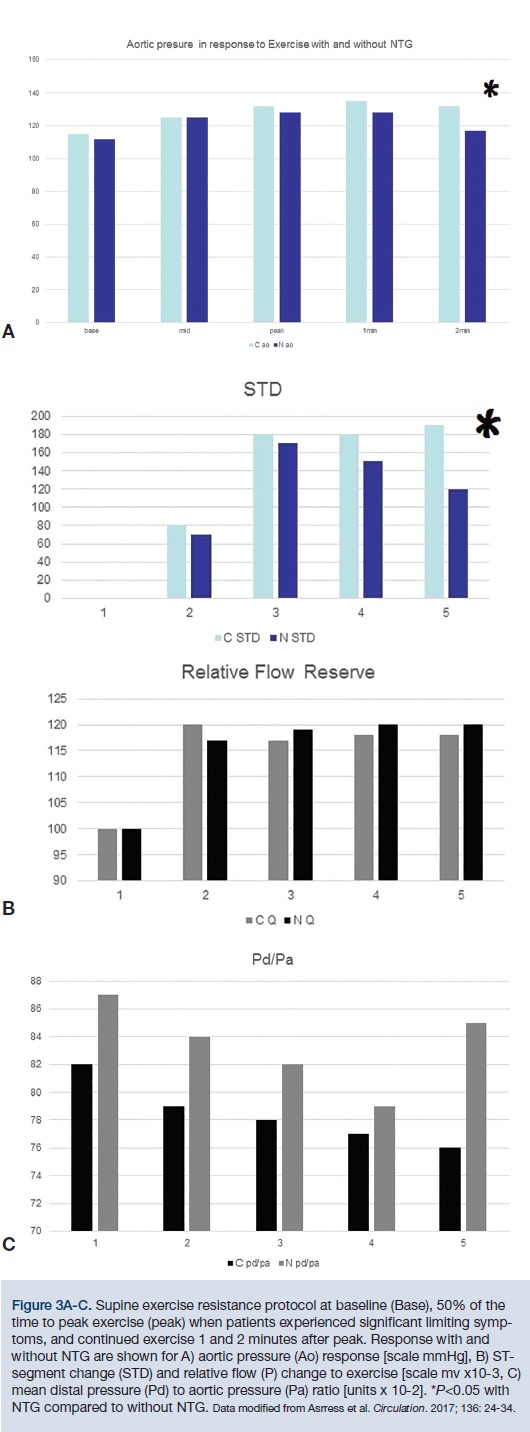 Asrress et al1 and an accompanying editorial by Drs. Gould and Johnson2, examine and discuss the remarkably well-delineated physiology and the implications of this study. Asress KN et al1 studied 40 patients with exertional angina and CAD, instrumenting the coronary stenosis from the radial approach. Patients exercised to angina continuously, measuring aortic and distal coronary pressure and flow velocity with sensor wires. At peak exercise, half the patients were given 800mcg sublinguinal NTG and exercised continued for 2 more minutes. The results showed that NTG reduced ST-segment depression (P=0.003, (Figure 3), afterload (aortic pressure, P=0.030), and myocardial oxygen demand (tension-time index, P=0.024; rate-pressure product, P=0.046). At the same time, NTG increased myocardial oxygen supply (Buckberg index, P=0.017). During exercise, the translesional coronary pressure gradient, stenosis resistance, and flow velocity increased, but not to statistical significance. Of note, the diastolic flow velocity-pressure gradient relation (P-V curves) showed an increase in relative stenosis severity, likely due to exercise-induced stenosis vasoconstriction with dilatation of normal segments, with trends toward reversal with nitroglycerin (Figure 3).
Asrress et al1 and an accompanying editorial by Drs. Gould and Johnson2, examine and discuss the remarkably well-delineated physiology and the implications of this study. Asress KN et al1 studied 40 patients with exertional angina and CAD, instrumenting the coronary stenosis from the radial approach. Patients exercised to angina continuously, measuring aortic and distal coronary pressure and flow velocity with sensor wires. At peak exercise, half the patients were given 800mcg sublinguinal NTG and exercised continued for 2 more minutes. The results showed that NTG reduced ST-segment depression (P=0.003, (Figure 3), afterload (aortic pressure, P=0.030), and myocardial oxygen demand (tension-time index, P=0.024; rate-pressure product, P=0.046). At the same time, NTG increased myocardial oxygen supply (Buckberg index, P=0.017). During exercise, the translesional coronary pressure gradient, stenosis resistance, and flow velocity increased, but not to statistical significance. Of note, the diastolic flow velocity-pressure gradient relation (P-V curves) showed an increase in relative stenosis severity, likely due to exercise-induced stenosis vasoconstriction with dilatation of normal segments, with trends toward reversal with nitroglycerin (Figure 3). 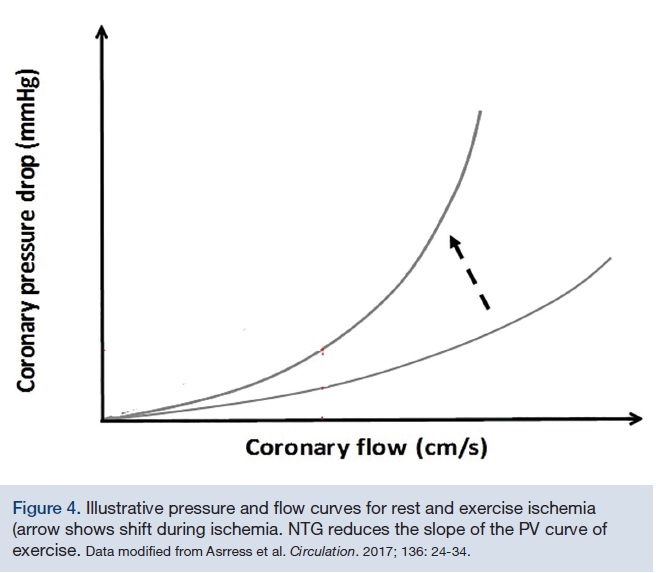 Simply put, NTG lowers the slope of the ischemic pressure/flow velocity curves (Figure 4), reducing the physiological stenosis severity (noted by increasing the Pd/Pa ratio pressure ratio despite a lowered aortic pressure, and accompanying reduced cardiac work and oxygen demand). The documented change in stenosis vasoconstrictor tone and dilation of the normal arterial segment, a response reversed by NTG, confirms one previously postulated mechanism of NTG angina relief.
Simply put, NTG lowers the slope of the ischemic pressure/flow velocity curves (Figure 4), reducing the physiological stenosis severity (noted by increasing the Pd/Pa ratio pressure ratio despite a lowered aortic pressure, and accompanying reduced cardiac work and oxygen demand). The documented change in stenosis vasoconstrictor tone and dilation of the normal arterial segment, a response reversed by NTG, confirms one previously postulated mechanism of NTG angina relief.Gould and Johnson2 provide additional insight into this superb study and summarize the findings that NTG relieves exercise angina by 1) reducing aortic pressure and oxygen demand for myocardial blood flow, 2) reducing physiological stenosis severity by geometric vasodilation, and 3) increasing coronary perfusion pressure, which then improves subendocardial perfusion. Any decrease in average transmural perfusion is because of more severe subendocardial hypoperfusion. The redistribution of subendocardial/subepicardial blood flow and ischemia is not directly measurable in the epicardial coronary vessel by pressure-derived fractional flow reserve (FFR). Finally, it seems that there is likely a difference between exercise ischemia and its influence on stenosis hemodynamics compared to adenosine-induced hyperemic gradient changes that we see with FFR. This observation opens more doors to understanding ischemia and coronary translesional hemodynamics.
The Bottom Line
Nitroglycerin has dependable, short-lived venous and arterial vasodilatory effects ameliorating ischemia through both reduction of myocardial oxygen demand (reduced aortic pressure and preload reduction by venodilation), and attenuation or reversal coronary vasoconstrictor tone, especially notable during exercise, convincingly shown by Asrress et al1. In practical terms, NTG reduces left ventricular preload, LVEDP, and LV end systolic volume. Next time we use NTG, we should incorporate these mechanisms into our treatment plans.
References
- Asrress KN, Williams R, Lockie T, Khawaja MZ, De Silva K, Lumley M, et al. Physiology of angina and its alleviation with nitroglycerine: insights from invasive catheter laboratory measurements during exercise. Circulation. 2017; 136: 24-34. doi: 10.1161/CIRCULATIONAHA.116.025856.
- Gould KL and Johnson NP. Nitroglycerine and angina evolving clinical coronary physiology beyond fractional flow reserve and coronary flow reserve. Circulation. 2017; 136: 35-38. doi: 10.1161/CIRCULATIONAHA.117.028791
- McGregor M. The nitrates and myocardial ischemia. Circulation. 1982; 66: 689-692.
- Kaski JC, Plaza LR, Meran DO, Araujo L, Chierchia S, Maseri A. An improved coronary supply: prevailing mechanisms of action of nitrates in chronic stable angina. Am Heart J. 1985; 110: 238-245.
- Liu P, Houle S, Burns RS, Kimball B, Warbick-Cecrone A, Johnston L, et al. Effect of intracoronary nitroglycerin on myocardial blood flow and distribution on pacing-induced angina pectoris. Am J Cardiol. 1985; 55: 1270-1276.
- Ganz W, Marcus HR: Failure of intracoronary nitroglycerin to alleviate pacing-induced angina. Circulation. 1972; 46: 880-889.
- Kingma I, Smiseth OA, Belenkie I, Knudtson ML, MacDonald RPR, Tyberg JV, Smith ER. A mechanism for the nitroglycerin-induced downward shift of the left ventricular diastolic pressure diameter relation. Am J Cardiol. 1986; 57: 673-677.
- Kern MJ, Eilen SD, O’Rourke R. Coronary vasomotion in angina at rest and effect of sublingual nitroglycerin on coronary blood flow. Am J Cardiol. 1985; 56: 484-485.
*Portions of this editor’s page have been taken with permission from Kern MJ, Aguirre FV, Hilton TC. Hemodynamic rounds: interpretation of cardiac pathophysiology from pressure waveform analysis. The effects of nitroglycerin. Cathet Cardiovasc Diagn. 1992; 25: 241-248.
Disclosure: Dr. Kern is a consultant for Abiomed, Merit Medical, Abbott Vascular, Philips Volcano, ACIST Medical, Opsens Inc., and Heartflow Inc.
