

Multimodality Imaging of an Extracardiac Shunt Due to an Anomalous Left Pulmonary Artery to Left Upper Pulmonary Vein Communication
A direct connection between a pulmonary artery (PA) and one of the pulmonary veins (PVs) is a rarity. Because of their unspecific symptoms (eg, dyspnea) and clinical signs (eg, central cyanosis, decreased arterial oxygen saturation), these pulmonary arteriovenous fistulas still remain a diagnostic challenge requiring multimodal imaging.
Even though the vast majority of extracardiac shunts are due to pulmonary atrioventricular malformations in hereditary diseases, we are presenting a case of an extracardiac shunt between the left pulmonary artery (LPA) and the left upper pulmonary vein (LUPV) in a young patient without known malformations.
CASE PRESENTATION
 A 40-year-old woman presented in our emergency department due to a presyncope with palpitations and vertigo. The physical examination did not reveal any pathological findings nor were there any hints for a cardiac disease in her past history to be found. Sinus rhythm without pre-excitation or repolarization disturbances was documented by the 12-lead electrocardiogram.
A 40-year-old woman presented in our emergency department due to a presyncope with palpitations and vertigo. The physical examination did not reveal any pathological findings nor were there any hints for a cardiac disease in her past history to be found. Sinus rhythm without pre-excitation or repolarization disturbances was documented by the 12-lead electrocardiogram.
A transthoracic echocardiography (TTE) was performed because of the vertigo. The only abnormality was an atrial septum aneurysm (Figure 1) with excessive mobility of the interatrial septum. To exclude the presence of a persistent foramen ovale (PFO), a contrast agent (Gelafusal air-succinil gelatin) was injected via a left-sided superficial brachial vein. Despite a well-performed Valsalva maneuver, no contrast agent crossed the interatrial septum. However, after two heartbeats, the contrast agent was flooding into the left atrium via the LUPV (Figure 2).
Gelafusal is a colloidal volume replacement agent for intravenous use in Ringer's acetate as a carrier solution. In this case, it was used as an alternative to agitated saline as the resulting microbubbles are more stable than with saline. Just as with agitated saline solution, a transpulmonary transfer of the contrast agent is not possible since the microbubbles would be filtered out in the alveolar capillaries.
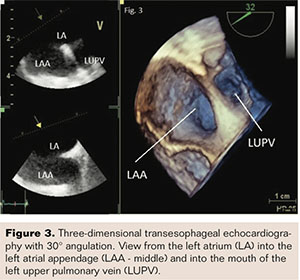
For the verification of the shunt via the LUPV and to further elucidate other possible cardiac reasons for the presyncope (eg, intracardiac thrombi), three-dimensional (3D) transesophageal echocardiography (TEE) was performed using the same contrast agent. The influx of the contrast agent into the left atrium exclusively via the LUPV could be confirmed nicely by two-dimensional (2D) and 3D echocardiographic imaging (Figures 3 and  4) with no further pathological findings in cardiac structures or function. This hardened the suspicion of an intrapulmonary shunt between the LPA and the LUPV.
4) with no further pathological findings in cardiac structures or function. This hardened the suspicion of an intrapulmonary shunt between the LPA and the LUPV.
To strengthen the diagnosis and to exclude other congenital anomalies of the thoracic vessels, we decided to add a computed tomography (CT) with a contrast agent to our diagnostic work-up. The presence of an intrapulmonary shunt was confirmed by demonstrating a direct connection between the LPA and the LUPV with a length of 2-3 mm and minimal diameter of 4 mm. Because of the limited and unspecific symptoms of the patient (no limitations of physical capacity, no desaturation, and no dyspnea), we decided in an interdisciplinary consensus simply to do regular clinical follow-ups of the patient and further echocardiography if necessary.
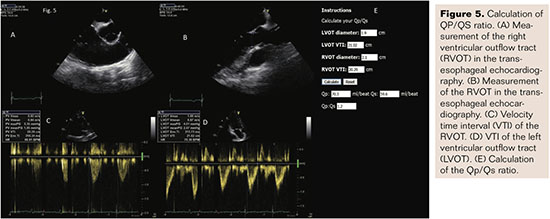
Due to a missing hemodynamic relevance of the shunt as measured echocardiographically (comparing the stroke volumes calculated by the velocity time integral in the right and left ventricular outflow tract yielded a minor left-to-right shunt, Qp/Qs 1.2; Figure 5), no invasive measurements were undertaken. The patient's consent for a publication of this case was obtained.
DISCUSSION
 In this case, a shunt between the LPA and LUPV could be detected by multimodal imaging. This shunt localization is a rarity in the current literature (pulmonary arteriovenous fistulas with a frequency of 0.02% in the general population),1,2 whereas a shunt between the right PA and the left atrium seems to be more common.3,4 A partial anomalous pulmonary vein connection (PAPVC) involving the PVs draining into the right atrium directly or indirectly by a venous connection is another rare congenital abnormal cardiac defect (0.4%-0.7% of the general population at autopsy)5 often (80%-90%) associated with an atrial septum defect. A drainage directly into the coronary sinus occurs in about 3% of these patients with a PAPVC, and in some cases a coexisting mitral valve disease is present.6,7 Again, TEE is a very suitable tool for the evaluation of such complex cardiac anomalies.8,9
In this case, a shunt between the LPA and LUPV could be detected by multimodal imaging. This shunt localization is a rarity in the current literature (pulmonary arteriovenous fistulas with a frequency of 0.02% in the general population),1,2 whereas a shunt between the right PA and the left atrium seems to be more common.3,4 A partial anomalous pulmonary vein connection (PAPVC) involving the PVs draining into the right atrium directly or indirectly by a venous connection is another rare congenital abnormal cardiac defect (0.4%-0.7% of the general population at autopsy)5 often (80%-90%) associated with an atrial septum defect. A drainage directly into the coronary sinus occurs in about 3% of these patients with a PAPVC, and in some cases a coexisting mitral valve disease is present.6,7 Again, TEE is a very suitable tool for the evaluation of such complex cardiac anomalies.8,9
Contrast echocardiography – even if performed transthoracically – is the best diagnostic tool for the initial evaluation of intracardiac or intrapulmonary shunts. The contrast agent should by applied via a vein of the left upper limb in order to 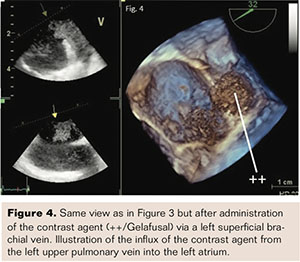 simultaneously exclude a persistent left superior caval vein.10,11 For the detection of a shunt, air-succinil gelatin should be preferred.12
simultaneously exclude a persistent left superior caval vein.10,11 For the detection of a shunt, air-succinil gelatin should be preferred.12
Further multimodal imaging techniques, including 2D- and 3D-TEE and CT or cardiac magnetic resonance imaging, can be performed to clearly delineate the size and localize the shunt.
Despite our extensive imaging work-up, the reason for the patient’s presyncope could not be identified. The presence of an intrapulmonary shunt possesses an increased risk for a paradoxical embolism,1 especially in situations with an elevated thromboembolic susceptibility (hereditary or acquired coagulation abnormalities) accompanied by an increased right atrial pressure like during pregnancy or surgery. In such situations, an interventional therapy should be considered for the shunt.
CONCLUSION
 Atypical localizations of extracardiac shunts can be observed even in the absence of known arteriovenous malformations through the use of multimodal imaging including contrast echocardiography and CT/magnetic resonance imaging.
Atypical localizations of extracardiac shunts can be observed even in the absence of known arteriovenous malformations through the use of multimodal imaging including contrast echocardiography and CT/magnetic resonance imaging.
REFERENCES
1. Dubrava J, Vulev I, Richter D. Isolated pulmonary arteriovenous fistulas with massive right-to-left shunt as a rare cause of cryptogenic stroke in a young woman. Isr Med Assoc J. 2014;16(5):320-321.
2. Friedlich A, Bling RJ, Blount SG. Physiological studies in congenital heart disease. Circulatory dynamics in the anomalies of venous return to the heart including pulmonary arteriovenous fistula. Bull Johns Hopkins Hosp. 1950;86(1):20-57.
3. Zeebregts CJAM, Nijveld A, Lam J, Oort AM, Lacquet LK. Surgical treatment of a fistula between the right pulmonary artery and the left atrium: presentation of two cases and review of literature. Eur J Cardiothorac Surg. 1997;11(6):1056-1061.
4. Schernthaner C, Danmayr F, Daburger A, Eichinger J, Hammerer M, Strohmer B. High incidence of echocardiographic abnormalities of the interatrial septum in patients undergoing ablation for atrial fibrillation. Echocardiography. 2013;4(4):402-4066.
5. Mikubo M, Ikeda S, Hoshino T. Pulmonary resection of lung cancer in a patient with partial anomalous pulmonary venous connection. Ann Thorac Surg. 2013;95(5):1799-1801.
6. Michalski B, Lipiec P, Chrzanowski L, Kasprzak JD. Giant coronary sinus secondary to partial anomalous pulmonary venous connection with combined mitral valve disease. Arch Med Sci. 2018;14(2):463-465.
7. Shioi K, Nagata Y, Mase T, Uwatoko K, Kato S, Tsuchioka H. Surgical repair of partial anomalous pulmonary venous connection to the coronary sinus: a case report of PAPVC with mitral and tricuspid valve regurgitation in adult. Nihon Kyobu Geka Gakkai Zasshi. 1991;39(1):108-112.
8. Ammash NM, Seward JB, Warnes CA, Connolly HM, O’Leary PW, Danielson GK. Partial anomalous pulmonary venous connection: diagnosis by transesophageal echocardiography. J Am Coll Cardiol. 1997;29(6):1351-1358.
9. Singhal K, Newton AD, Corbett C, Predina JD. Management of partial anomalous pulmonary venous connections in patients requiring pulmonary resection: a case report and systematic review. J Thorac Dis. 2017;9(12):5434-5439.
10. Wilhelm J, Issa H, Behrmann C, Werdan K, Heinroth K. Atypical course of a persistent left superior vena cava through the left atrium. Eur J Echocardiogr. 2011;12(8):635.
11. Woods TD, Patel A. A critical review of patent foramen ovale detection using saline contrast echocardiography: when bubbles lie. J Am Soc Echocardiogr. 2006;19(2):215-222.
12. Puledda F, Toscana M, Pieroni A, Veneroso G, Di Piero V, Vicenzini E. Right-to-left shunt detection sensitivity with air-saline and air-succinil gelatin transcranial Doppler. Int J Stroke. 2016; 11(2):229-238.

