

ADVERTISEMENT
Novel Microsnare Successfully Used to Remove Small Debris from the Right Coronary Artery
ABSTRACT: Soutenir (Asahi-Intecc, Nagoya, Japan), a novel microsnare, was used to grip and pull a retrograde guidewire through arteries with chronic total occlusions during percutaneous coronary intervention (PCI). Soutenir can pass through a microcatheter with a 0.020˝ lumen, and it can easily enter distal lesions in the coronary artery. Here, we introduce a method for retrieving the tip of a broken intravascular ultrasound (IVUS) catheter by using this microsnare. We present the case of a 64-year-old man who was referred to our hospital for narrowing of the proximal right coronary artery (RCA). After IVUS examination, the catheter was removed from the artery with some difficulty, and the catheter tip broke. The broken tip remained in the RCA and was carried along with the blood to the distal part of the RCA. The conventional gooseneck snare and filter device failed to retrieve the broken tip. However, Soutenir easily passed beyond the catheter tip and reached the distal part of the atrioventricular branch. It snared the tip of the catheter, whereby the tip could easily be removed. Thus, without damaging the RCA, we successfully removed the broken catheter tip from the RCA using this microsnare.
J INVASIVE CARDIOL 2011;23:E161–E163
__________________________________________
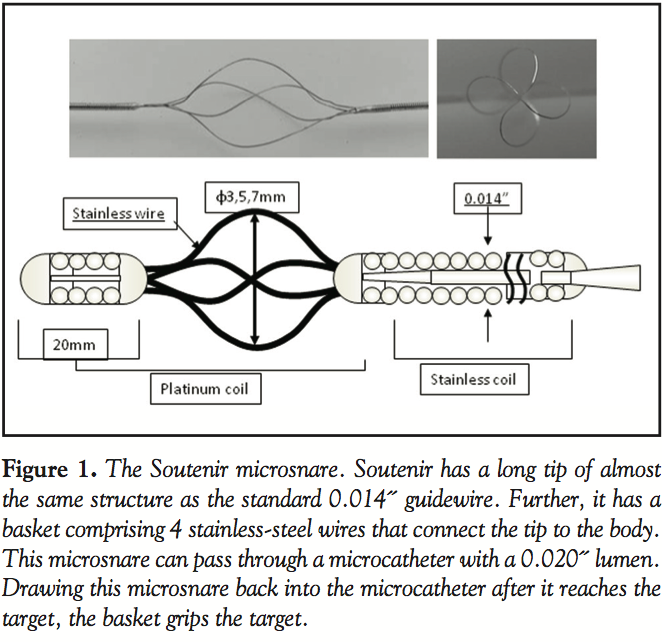 Soutenir (Asahi-Intecc, Nagoya, Japan), a novel microsnare, has been used to catch thrombus in the carotid artery.1 It also has been used to grip and pull a retrograde guidewire through arteries with chronic total occlusion (CTO) during percutaneous coronary intervention (PCI).2 This device has a long tip that is similar in structure to the standard 0.014˝ coronary guidewires, whereby it can access distal lesions of the coronary artery. Furthermore, it has a small stainless wire basket that grips the guidewire that passes through the CTO lesion via the collateral artery with retrograde manner (Figure 1). Soutenir can pass through a microcatheter with a 0.020˝ lumen. By using this novel microsnare, we successfully retrieved the tip of a broken intravascular ultrasound (IVUS) catheter from the distal right coronary artery (RCA).
Soutenir (Asahi-Intecc, Nagoya, Japan), a novel microsnare, has been used to catch thrombus in the carotid artery.1 It also has been used to grip and pull a retrograde guidewire through arteries with chronic total occlusion (CTO) during percutaneous coronary intervention (PCI).2 This device has a long tip that is similar in structure to the standard 0.014˝ coronary guidewires, whereby it can access distal lesions of the coronary artery. Furthermore, it has a small stainless wire basket that grips the guidewire that passes through the CTO lesion via the collateral artery with retrograde manner (Figure 1). Soutenir can pass through a microcatheter with a 0.020˝ lumen. By using this novel microsnare, we successfully retrieved the tip of a broken intravascular ultrasound (IVUS) catheter from the distal right coronary artery (RCA).
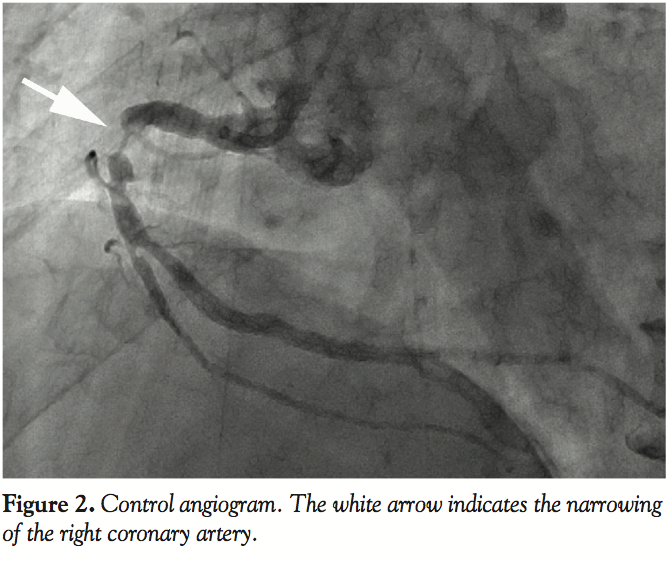 Case Report. A 64-year-old man was referred to our hospital with exertional chest pain. An angiogram showed severe narrowing of the proximal RCA (Figure 2). We decided to perform PCI, and the patient was administered antiplatelet agents. A 6 French (Fr) guide catheter (JR 4.0) was advanced into the RCA via the right radial artery. A 0.014˝ guidewire easily passed through the narrowed artery and entered the atrioventricular (AV) branch. IVUS was performed to evaluate the plaque characteristics. The IVUS catheter passed through the lesion with some difficulty.
Case Report. A 64-year-old man was referred to our hospital with exertional chest pain. An angiogram showed severe narrowing of the proximal RCA (Figure 2). We decided to perform PCI, and the patient was administered antiplatelet agents. A 6 French (Fr) guide catheter (JR 4.0) was advanced into the RCA via the right radial artery. A 0.014˝ guidewire easily passed through the narrowed artery and entered the atrioventricular (AV) branch. IVUS was performed to evaluate the plaque characteristics. The IVUS catheter passed through the lesion with some difficulty.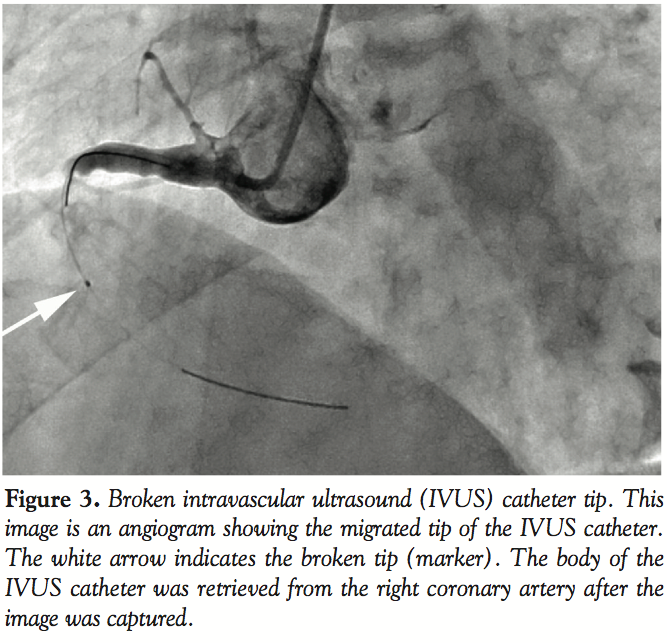 We captured plaque images and decided to perform direct stenting with a 4.0 mm bare-metal stent. After the examination, we removed the catheter with some difficulty, but the tip of the IVUS catheter (marker) broke and remained in the distal part of the narrowing of the RCA (Figure 3). We attempted to dilate the narrowing with a balloon catheter and a stent, so that a retrieval device could be introduced into the narrowed artery to remove the broken tip. When balloon angioplasty with a
We captured plaque images and decided to perform direct stenting with a 4.0 mm bare-metal stent. After the examination, we removed the catheter with some difficulty, but the tip of the IVUS catheter (marker) broke and remained in the distal part of the narrowing of the RCA (Figure 3). We attempted to dilate the narrowing with a balloon catheter and a stent, so that a retrieval device could be introduced into the narrowed artery to remove the broken tip. When balloon angioplasty with a 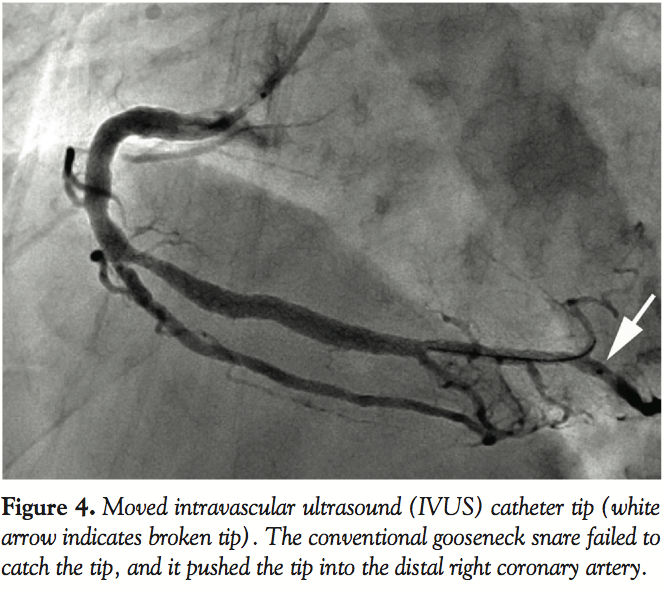 3.0 mm balloon catheter was performed, the tip shifted to the middle of the RCA. A 4.0 mm bare-metal stent was successfully implanted into the proximal RCA and dilated the narrow part. We first tried to remove the tip with a conventional gooseneck snare. However, this snare pushed the tip further into the AV branch, and we could not retrieve it from the AV branch with a conventional gooseneck snare (Figure 4).
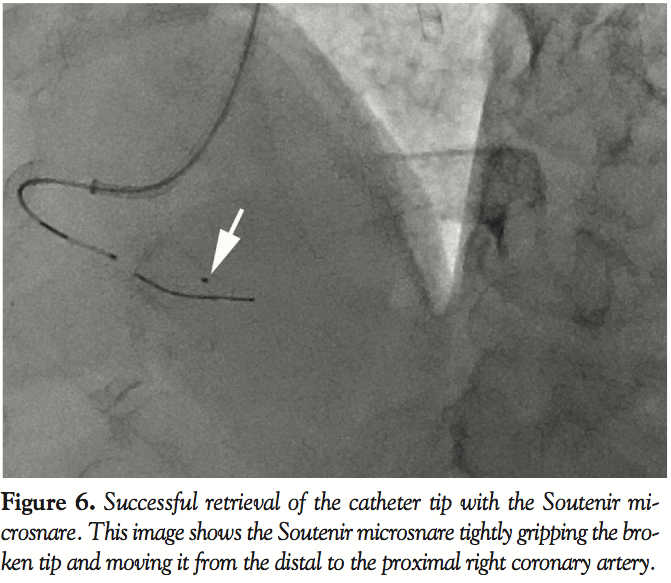
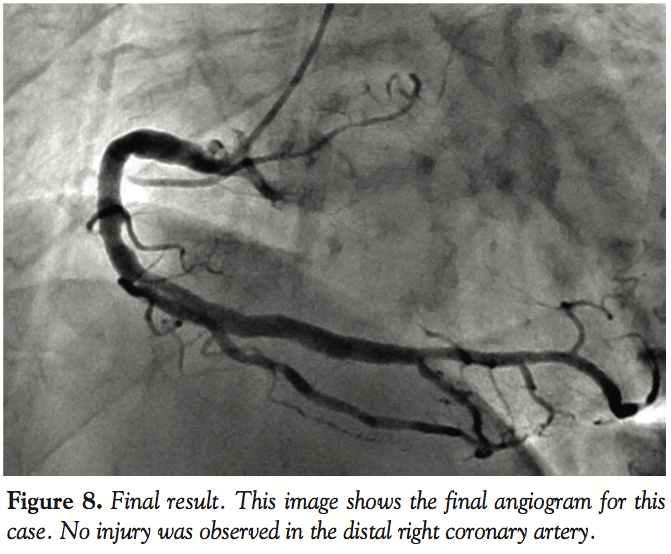
3.0 mm balloon catheter was performed, the tip shifted to the middle of the RCA. A 4.0 mm bare-metal stent was successfully implanted into the proximal RCA and dilated the narrow part. We first tried to remove the tip with a conventional gooseneck snare. However, this snare pushed the tip further into the AV branch, and we could not retrieve it from the AV branch with a conventional gooseneck snare (Figure 4).  We then used a filter device that passed through the broken tip and succeeded in returning it to the middle of the RCA; however, the filter was unable to remove the tip out of the artery because it had entered the space on a side of the broken tip. Hence, although the filter reached the tip, it could not capture it (Figure 5). Thus, we selected the Soutenir device to remove the tip. First, the microcatheter, which had a 0.020˝ lumen, advanced into the AV branch with the conventional guidewire. The Soutenir easily passed through the microcatheter and reached the distal AV branch. The Soutenir basket remained in the microcatheter during its advancement through the RCA; however, on reaching the distal AV branch, the basket protruded out from the microcatheter. Using the basket, we very gently pulled the Soutenir microsnare out of the right ventricular branch. It had successfully captured the broken catheter tip, and the snare along with the retrieved catheter tip was easily drawn out through the guide catheter (Figures 6 and 7). A final angiogram showed that the procedure caused no injury to the distal RCA (Figure 8).
We then used a filter device that passed through the broken tip and succeeded in returning it to the middle of the RCA; however, the filter was unable to remove the tip out of the artery because it had entered the space on a side of the broken tip. Hence, although the filter reached the tip, it could not capture it (Figure 5). Thus, we selected the Soutenir device to remove the tip. First, the microcatheter, which had a 0.020˝ lumen, advanced into the AV branch with the conventional guidewire. The Soutenir easily passed through the microcatheter and reached the distal AV branch. The Soutenir basket remained in the microcatheter during its advancement through the RCA; however, on reaching the distal AV branch, the basket protruded out from the microcatheter. Using the basket, we very gently pulled the Soutenir microsnare out of the right ventricular branch. It had successfully captured the broken catheter tip, and the snare along with the retrieved catheter tip was easily drawn out through the guide catheter (Figures 6 and 7). A final angiogram showed that the procedure caused no injury to the distal RCA (Figure 8).
During and after this procedure, the patient did not experience chest pain, and no ST-T changes were noted in the electrocardiogram. The following day, the patient was discharged from the hospital.
 Discussion. In this case report, we introduce the use of the novel microsnare, Soutenir, for retrieving the tip of a broken catheter from the distal coronary artery. Recently, retrograde wire manipulation became a very important technique to treat occluded coronary arteries.3 Soutenir was used to hold and pull the guidewire through lesions in the distal or middle part of the coronary artery during retrograde CTO manipulation.2 Soutenir has a long tip, with which it can easily be advanced through a specific branch of the coronary artery. Furthermore, one can select the size of the Soutenir basket (3, 5, or 7 mm) according to the size of the selected branch of the coronary artery. The Soutenir basket can expand to a size similar to that of the target coronary artery branch; hence, the Soutenir is better able to pull the guidewire than other retrieval devices.
Discussion. In this case report, we introduce the use of the novel microsnare, Soutenir, for retrieving the tip of a broken catheter from the distal coronary artery. Recently, retrograde wire manipulation became a very important technique to treat occluded coronary arteries.3 Soutenir was used to hold and pull the guidewire through lesions in the distal or middle part of the coronary artery during retrograde CTO manipulation.2 Soutenir has a long tip, with which it can easily be advanced through a specific branch of the coronary artery. Furthermore, one can select the size of the Soutenir basket (3, 5, or 7 mm) according to the size of the selected branch of the coronary artery. The Soutenir basket can expand to a size similar to that of the target coronary artery branch; hence, the Soutenir is better able to pull the guidewire than other retrieval devices.
 In the present case, the conventional gooseneck snare failed to capture the broken catheter tip remaining in the RCA. Some studies have shown the efficacy of the conventional gooseneck snare in the retrieval of migrated stents in the proximal coronary artery.4,5 However, in our study, delivering a gooseneck snare to the distal RCA was difficult. Moreover, on reaching the broken tip, the snare was unable to capture it and in fact pushed the tip further into the artery. The other devices we used in this study easily entered the distal RCA; this is because they had longer tips than the gooseneck snare, which helped them enter the arteries.
In the present case, the conventional gooseneck snare failed to capture the broken catheter tip remaining in the RCA. Some studies have shown the efficacy of the conventional gooseneck snare in the retrieval of migrated stents in the proximal coronary artery.4,5 However, in our study, delivering a gooseneck snare to the distal RCA was difficult. Moreover, on reaching the broken tip, the snare was unable to capture it and in fact pushed the tip further into the artery. The other devices we used in this study easily entered the distal RCA; this is because they had longer tips than the gooseneck snare, which helped them enter the arteries.
 In this case, filter devices were more appropriate for retrieval than the conventional gooseneck snare because they could easily enter the distal RCA, thereby reaching the catheter tip. However, the filter devices failed to capture the tip. We used a small 3.5 mm filter to avoid injury to the RCA. However, this device may have been too small to capture the catheter tip in the middle of the RCA (Figure 5).
In this case, filter devices were more appropriate for retrieval than the conventional gooseneck snare because they could easily enter the distal RCA, thereby reaching the catheter tip. However, the filter devices failed to capture the tip. We used a small 3.5 mm filter to avoid injury to the RCA. However, this device may have been too small to capture the catheter tip in the middle of the RCA (Figure 5).
Since Soutenir was developed to grip the guidewire in the middle or distal sites of the coronary artery, it may be ideal for capturing debris such as broken wires, broken tubes, and migrated stents from the distal coronary artery. Thus, Soutenir should henceforth be considered an option for debris removal from the RCA.
References
- Imai K, Mori T, Izumoto H, et al. Clot removal therapy by aspiration and extraction for acute embolic carotid occlusion. Am J Neuroradiol 2006;27:1521–1527.
- Rathore S, Katoh O, Tuschikane E, et al. A novel modification of the retrograde approach for the recanalization of chronic total occlusion of the coronary arteries. J Am Coll Cardiol Interv 2010;3:155–164.
- Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheter Cardiovasc Interv 2008;71:8–19.
- Yang Soon C, Chong E, Sangiorgi GM. A challenging case of dislodged stent retrieval with the use of gooseneck snare kit. Catheter Cardiovasc Interv 2010;75:634–635.
- Wani SP, Rha SW, Park JY. Entrapment of a drug-eluting stent in left descending artery and left main artery leading to a life-threatening complication. J Invasive Cardiol 2010;22:90–92.
__________________________________________
From the Department of Cardiovascular Medicine and Advanced Cardiovascular Center, Shinshu University Graduate School of Medicine, Matsumoto, Japan.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 29, 2010, provisional acceptance given November 17, 2010, final version accepted November 29, 2010.
Address for correspondence: Dr. Yusuke Miyashita, Shinshu University Graduate School of Medicine, Department of Cardiovascular Medicine, 3-1-1 Asahi, Matsumoto, Japan. Email: ybm1965@shinshu-u.ac.jp
