


While ovarian cancer is the second most common gynecologic cancer in the United States, behind uterine cancer,1 it is the top gynecologic cancer in mortality.2 In 2020, an estimated 21,750 new cases of ovarian cancer will be diagnosed, accounting for only 1.2% of all new cancer cases in the United States. Ovarian cancer will cause an estimated 13,940 deaths this year, making up 2.3% of the country’s cancer mortalities.3 An estimated 233,364 women lived with ovarian cancer in 2017,3 diagnosed at a median age of 63 years; 71.1% of all new diagnoses are in women aged 65 and older.3
The 5-year survival rate is 48.6% for 2010-2016, greatly differing by the stage at diagnosis. For a patient diagnosed with localized ovarian cancer, the 5-year survival rate is 92.6%; for a regional staging at initial diagnosis, the survival rate is 74.8%; and for a patient diagnosed with metastases, the survival rate is 30.2%.3 Fortunately, diagnosis and mortality rates declined between 2008 and 2017: the age-adjusted average annual rate was 2.5% for new diagnoses and 2.2% for mortality rates.3
Ovarian cancer risk factors include age, nulliparity or first pregnancy after age 35 years, postmenopausal hormone therapy, and pelvic inflammatory disease. There is an association with women who develop early-onset ovarian cancer (about 15% of ovarian cancer patients) with family history of ovarian cancer and BRCA1/2 mutations, and with Lynch syndrome.4
About 70% of ovarian cancer patients present with advanced disease,4 typically stage III.4 No regular screenings are available. Symptoms include swelling, pain, feelings of pressure in the pelvis or abdomen; heavy/irregular vaginal bleeding, particularly after menopause; clear, white or blood-tinged vaginal discharge; gastrointestinal issues; pelvic area lump,5 urinary symptoms; and eating difficulties or feeling full too quickly.4
Staging and Classification
The more than 30 types of ovarian cancer are broken down by three cell types: epithelial, germ cell, and stromal cell. 6 About 90% of ovarian cancers are epithelial,6 and thus is the focus of this overview. Ovarian cancer stages range from stages I-IV, with additional subgroups (Box 1).
 Ovarian Cancer Workup
Ovarian Cancer Workup
The workup for an undiagnosed pelvic mass or symptoms should include imaging (abdominal/pelvic ultrasound initially or computerized tomography/magnetic resonance imaging scan with contrast if indicated) and lab tests. A biopsy or surgical specimen would evaluate positive or unclear imaging results. The National Comprehensive Cancer Network (NCCN) Guidelines recommend avoiding fine-needle aspiration (FNA) for potential early-stage disease, to avoid cyst rupture. FNA is acceptable for nonsurgical candidates with bulky disease.4
The patient’s histology should be evaluated, to determine the epithelial ovarian cancer subtype: serous, endometrioid, mucinous, or clear cell. About 70% of patients have serous histology. Molecular characterization of mutations in these histologies is likely different for low- vs higher-grade tumors. Based on the molecular mutations, the cancer is further divided into grades 1 and 2. Grade 1 (low-grade) serous tumors are considered relatively resistant to chemotherapy treatment.4
Surgical Management
The Guidelines recommend that those at risk for hereditary breast and ovarian cancer syndrome (HBOC) receive a risk-reducing salpingo-oophorectomy. Surgical debulking and staging as primary treatment is standard for presumed ovarian cancer, usually followed by systemic chemotherapy. Surgery is typically a total abdominal hysterectomy (TAH), along with bilateral salpingo-oophorectomy (BSO), unless the patient wants to maintain her fertility. In that case, patients at stage IA or IC and/or with a low risk ovarian tumor can undergo a unilateral salpingo-oophorectomy. Those with stage IB tumors wanting to maintain fertility may undergo a BSO. Comprehensive staging would be done for all; about 30% of those undergoing complete surgical staging are upstaged postoperatively.4
The Guidelines recommend that patients with stage II-IV disease undergo debulking surgery as initial treatment, aiming for residual tumor nodules <1 cm thick/maximum diameter, ideally resecting to R0. Patients with upper abdominal metastases should undergo extensive resection if tolerated. All gross disease should be removed if possible, with ascites aspirated or peritoneal lavage performed when entering the abdomen, for cytologic evaluation. This evaluation is not helpful for staging or management if gross or obvious disease is found beyond the ovaries.
The surgeon should remove encapsulated masses intact, if possible, plus all involved omentum and resect suspicious/enlarged lymph nodes. The Guidelines suggest higher overall survival rates for those with advanced ovarian cancer undergoing complete debulking with systematic lymphadenectomy. Patients with stage II or III invasive epithelial ovarian cancer undergoing surgical debulking and with low-volume residual disease are candidates for intraperitoneal therapy (IP); surgeons might place an IP catheter intraoperatively.4
Neoadjuvant Therapy
When maximum debulking is not possible for stage III or IV disease, or patients are poor surgical candidates, the clinician may recommend neoadjuvant therapy. This is not appropriate for patients with disease likely confined to the ovary.
Before neoadjuvant therapy, clinicians should obtain histologic confirmation, preferably with a core biopsy; a CA-125:CEA ratio is also recommended. If neoadjuvant therapy and interval debulking surgery (IDS) is planned, the patient should be evaluated for surgery after the third chemotherapy cycle. If surgery is indicated, the Guidelines recommend a TAH with BSO and staging, followed by three additional rounds of adjuvant therapy.
The Guidelines recommend intravenous (IV) taxane/carboplatin and liposomal doxorubicin/carboplatin regimens for both neoadjuvant and adjuvant therapy following debulking surgery. After these regimens, IP/IV therapy consisting of paclitaxel/cisplatin can be used.
Postoperative Chemotherapy
For women with stage IA or IB, grade 1 or 2 tumors, observation is recommended if the disease was surgically debulked and staged, as survival is more than 90% with this treatment.
IV chemotherapy: IP chemotherapy is not recommended for stage I or IV disease. The Guidelines recommend six cycles of initial IV combination chemotherapy for those with stage II-IV of disease. For earlier stages, the Guidelines recommend three to six cycles, with a potential survival advantage for six cycles for some with serous cytology.
Recommended IV chemotherapy regimens include several variations of paclitaxel/carboplatin dosing; docetaxel/carboplatin; or carboplatin/doxorubicin. These regimens can be used for neoadjuvant therapy as well.
Patients unable to receive IP therapy or combination IV therapies can receive single platinum agents, including carboplatin or cisplatin. Weekly carboplatin/paclitaxel regimen can be given to elderly patients or those with poor performance status and advanced ovarian cancer, as the phase III MITO-7 trial showed it was associated with fewer side effects and better quality of life than the standard therapy, IV carboplatin/paclitaxel given every 3 weeks.7
Another first-line IV treatment includes carboplatin/liposomal doxorubicin for advanced ovarian cancer patients, with a category 2A recommendation. The Guidelines include this category 2B recommendation, adding an anti-angiogenesis agent to the chemotherapy combination and maintenance. Bevacizumab can be added to initial therapy of carboplatin/paclitaxel, followed by bevacizumab maintenance therapy.
IV/IP chemotherapy: For other stages, complete resection of visible disease is the optimal course, followed by IP if appropriate, along with IV postoperative chemotherapy for most patients, according to the Guidelines. The Guidelines recommend IV/IP chemotherapy for those with Stage III optimally debulked disease (<1cm residual). Survival in this group increased by 16 months after IP therapy using cisplatin/paclitaxel compared with standard IV therapies. Women with stage II optimally debulked disease may also receive IV/IP chemotherapy, though the Guidelines note there is no published randomized evidence for this stage.
Recommended IP chemotherapy includes paclitaxel /cisplatin. The Guidelines note that the randomized phase 3 trial for the IP/IV regimen used paclitaxel continuously infused over 24 hours; the alternative paclitaxel infusion over 3 hours was more convenient and less toxic but not equivalent to the 24-hour infusion. Guidelines note that candidates for IP cisplatin and IV/IP paclitaxel regimen should begin with normal renal functioning, a medically appropriate performance status, and no preexisting conditions that could worsen as a result of chemotherapy.
Clinical trials: Select women with stage I, grade 1 tumors, and a survival rate of more than 95%, should not be encouraged to enter clinical trials. The Guidelines suggest that all other ovarian cancer patients should be encouraged to enter clinical trials for primary or recurrent treatment.
Radiation therapy: Whole abdominal radiation therapy is not recommended. Localized radiation therapy can be used for palliative treatment to control for symptoms of recurrent disease.
Maintenance therapy: There are several maintenance therapies for patients with advanced ovarian cancer and complete clinical remission following first-line therapy. Single agent use of paclitaxel or pazopanib are category 2B recommendations for maintenance therapy. The Guidelines note that bevacizumab can be continued as maintenance only following primary IV therapy that included the agent.
The Guidelines recommend the poly ADP ribose polymerase (PARP) inhibitor olaparib for maintenance therapy in advanced ovarian cancer patients if they received two or more chemotherapy lines. Niraparib, another PARP inhibitor, is recommended maintenance therapy for patients with platinum-sensitive ovarian cancer with two or more prior lines of platinum-based therapy and a complete or partial response to the most recent therapy line.
While not in the Guidelines, in April 2020 the Food and Drug Administration (FDA) recently approved niraparib for maintenance therapy for those with complete or partial response to first-line platinum-based therapy.8 In May 2020, the FDA also approved the combination of olaparib and bevacizumab as a first-line maintenance therapy for advanced epithelial ovarian cancer for those with complete or partial response to first-line platinum-based chemotherapy, whose cancer is homologous recombination deficiency-positive.9
After Primary Treatment
Clinical reevaluation is recommended after finishing primary therapy. Those in complete clinical remission (no definitive evidence of disease) should be observed with follow-ups. This may identify recurrent disease through symptoms like weight loss or pelvic pain, biochemically using CA-125 levels, and/or with imaging.
Patients whose disease progressed, patients with persistent disease, or patients with stable disease during initial treatment, should receive a second-line approach. Those with advanced epithelial cancer in complete clinical remission after primary treatment can be observed, enter a clinical trial, or receive maintenance systemic therapy of paclitaxel or pazopanib (shown to prolong progression-free survival [PFS] after initial chemotherapy), or receive bevacizumab as previously discussed.
The Guidelines do not fully recommend immediate treatment for those with an increasing CA-125 level but without recurrent disease symptoms or positive imaging studies. Immediate treatment is a category 2B recommendation; patients can enter a clinical trial or continue with observation until clinical symptoms arise. If the patient elects treatment, tamoxifen (or other hormonal agents) or other recurrence therapy, could be administered.
 Treatment of Recurrence
Treatment of Recurrence
Patients with disease recurrence, patients refractory to two consecutive chemotherapy regimens, and those with disease recurrence in <6 months (platinum-resistant) have a poor prognosis. The Guidelines recommend enrolling in clinical trials to find active agents for this cohort. The Guidelines do not recommend additional treatment with paclitaxel or a platinum-based agent. The patient’s renal and hepatic status should be evaluated before recommending further treatment.
Platinum-sensitive: Patients who relapse >6 months after initial chemotherapy are platinum-sensitive, and the Guidelines recommend they receive six cycles of combination platinum-based chemotherapy for a first recurrence, with reevaluation after two to four cycles. Lower doses for recurrent therapies may be needed for patient tolerance. Patients progressing on two consecutive chemotherapy regimens with no evidence of clinical benefit may not benefit from further regimens.
The Guidelines do not recommend a specific therapeutic agent for treating recurrent ovarian cancer. Consider six cycles of a platinum-based therapy for platinum-sensitive patients, including carboplatin/paclitaxel, carboplatin/liposomal doxorubicin, carboplatin/weekly paclitaxel, carboplatin/albumin-bound paclitaxel, carboplatin/docetaxel, carboplatin/gemcitabine, cisplatin/gemcitabine, or carboplatin/gemcitabine/bevacizumab. Patients who cannot tolerate a combination may receive single agent carboplatin or cisplatin.
The Guidelines recommend PARP inhibitor olaparib as a single agent recurrence therapy for select patients with BRCA1/2 mutations and advanced ovarian cancer. They should be platinum-sensitive or platinum-resistant and have received three or more lines of chemotherapy. Single agent rucaparib is also recommended as recurrence therapy for platinum-sensitive or resistant ovarian cancer patients treated with two or more chemotherapy lines and with BRCA mutations.
Platinum-resistant: The Guidelines recommend that those with platinum-resistant disease receive nonplatinum-based agents or regimens, which includes sequential therapy using single agents: docetaxel, oral etoposide, gemcitabine, weekly paclitaxel with/without pazopanib, liposomal doxorubicin with/without bevacizumab, weekly paclitaxel/bevacizumab, topotecan with/without bevacizumab, or a single agent therapy. The Guidelines do not recommend combination therapy over single agent therapy for platinum-resistant disease.
Other potentially active agents for this group include altretamine, capecitabine, cyclophosphamide, doxorubicin, ifosfamide, irinotecan, melphalan, oxaliplatin, paclitaxel, nanoparticle albumin-bound paclitaxel (nab-paclitaxel), pemetrexed, and vinorelbine. If resistant to platinum and taxanes, patients might receive capecitabine or alkylating agents cyclophosphamide and melphan. Tamoxifen or other hormonal therapies are also acceptable for patients who cannot tolerate or have not responded to cytotoxic regimens.
Patients who relapse >6 months after primary treatment can consider cytoreductive surgery for potential complete debulking.
Summary of Changes Since NCCN 3.2019
The workup for epithelial ovarian cancer was expanded in the NCCN 1.2020 version to include genetic risk and evaluation for germline and somatic testing instead of only genetic risk and evaluation of BRCA1/2. The new version notes that germline and/or somatic BRCA1/2 status informs maintenance therapy; previous Guidelines said that primary treatment should not be delayed for a genetic counseling referral. The new version added that, in the absence of a BRCA1/2 mutation, homologous recombination deficiency status may help inform about possible success of PARP inhibitor therapy.
The new Guidelines significantly clarified recommendations for patients referred with newly diagnosed ovarian cancer (page OV-3) after a surgical procedure.
The new version has a modified pathology staging for stage IC: from grade 1 endometrioid to high-grade serous or grade 2/3 endometrioid. For stage IA or IB, grade 2 endometrioid, the Panel recommended eliminating the number of platinum-based cycles to instead link to page OV-C, 6 of 9, which has a chart of regimens.
Page OV-5 was significantly changed for post-primary treatment of stages II-IV. The Guidelines added niraparib to maintenance therapy options for those with complete or partial remission if they have BRCA1/2 wild-type or unknown and did not use bevacizumab as primary therapy or for those with germline or somatic BRCA1/2 mutation (category 1 if bevacizumab was not used as a primary therapy, and category 2A if it was). The Guidelines modified a category of evidence for olaparib for patients with a germline or somatic BRCA1/2 mutation who did not receive bevacizumab during primary therapy and deleted the category 1 recommendation for germline mutations and the category 2A recommendation for somatic mutations.
That page also changed to add the option of bevacizumab plus olaparib and category 2A recommendation for those who are in complete or partial remission if bevacizumab was used as primary therapy. The Guidelines removed bevacizumab for postremission therapy for those with stable disease after initial therapy with a regimen containing that agent. The panel modified the indications for postremission use of bevacizumab, adding it as an option for women with complete or partial remission after treatment with a combination with the agent if the patient has BRCA1/2 wild-type or unknown and not recommending it for patients with BRCA1/2 mutation. Guidelines were modified to note that, after first-line therapy with bevacizumab, the data are limited on maintenance therapy with a single PARP inhibitor (olaparib or niraparib) for patients with a germline or somatic BRCA1/2 mutation, but single agent PARP inhibitors can be considered given the benefit they have shown in maintenance therapy for other subgroups. They added that data are limited for using a PARP inhibitor for maintenance therapy in patients with stage II disease.
On the page for therapy for persistent or recurrent disease, OV-7, the panel modified the original recommendation for patients with platinum-sensitive disease who completed two or more lines of platinum-based therapy, adding that this is preferred course for those with a BRCA mutation. They also modified the statement that there are limited data for using a maintenance PARP inhibitor. They added that this is in patients who previously received a PARP inhibitor or after recurrence therapy with bevacizumab.
Under principles of surgery, OV-A (3 of 4), the panel made a slight modification to change the IDS to completing a hysterectomy instead of TAH after three to four cycles of neoadjuvant chemotherapy, instead of after four cycles.
They slightly modified the College for American Pathologists protocol for pathology assessment to substitute these tumor sites (ovary, fallopian tube, or primary peritoneum) for these (pelvic/abdominal peritoneum, uterus, cervix, and omentum). They also recommended scalp cooling to reduce alopecia.
Patients receiving neoadjuvant therapy with stable disease may now continue past six cycles if tolerant.
The Panel added categories for preferred regimens for primary systemic therapies. They also modified the notation that alternate dosing of IV regimens in elderly patients with epithelial ovarian cancer may be appropriate, based on clinical judgment and expected tolerance. They updated primary systemic therapy regimen dosing information and removed infusion times. The Panel added the recommendation for six cycles of chemotherapy for stage II-IV disease for certain chemotherapy regimens.
For olarparib, used as a recurrence therapy, it is now recommended for patients with deleterious germline BRCA-mutated advanced ovarian cancer to be used with patients treated with two or more lines of chemotherapy, lowered from three lines of therapy previously.
Review of Clinical Data Leading to the Changes
The addition of niraparib is based on the NOVA phase 3 trial, which assessed the agent for effectiveness as maintenance therapy in platinum-sensitive patients responding to recurrence therapy. In a previous update, the Panel recommended repeating prior imaging to assess response. Data showed that niraparib increased PFS in patients with/without the BRCA mutation compared to placebo. Patients without a germline BRCA mutation had an increased PFS (12.9 months vs 3.8 months), while women with a germline mutation had an increased PFS (21.0 months vs 5.5 months).10 The Panel previously recommended niraparib as maintenance therapy for platinum-sensitive patients who and already had two or more lines of platinum-based therapy with a complete or partial response to the most recent line.
Several studies cited in the Guidelines included olaparib as a therapeutic agent. The PARP inhibitor is active in some patients, notably those with BRCA1/2 mutations, who have higher response rates than those who are BRCA1/2 negative, particularly for those who are platinum-sensitive. Patients resistant or refractory to platinum (and with BRCA1/2 mutations) tend to have a lower olaparib response rate, according to the research. In one trial of patients with recurrent advanced ovarian cancer, patients experienced a 34% response rate, mostly a partial response rate.11 The FDA approved the agent for advanced ovarian cancer treated with 3+ chemotherapy lines and with germline BRCA mutation.12 The Panel recommended using olaparib as a single agent for recurrence therapy for those with platinum-sensitive or platinum-resistant advanced ovarian cancer for women with a germline BRCA mutation, after three lines of treatment.
The olaparib maintenace therapy recommendation was based on the SOLO2/ENGOT-Ov21 phase 3 randomized trial for women who received 2+ lines of therapy. The study showed median PFS as significantly higher for those receiving the agent compared to placebo (19.1 months vs 5.5 months).13 The FDA approved olaparib tablets for maintenance therapy for those with recurrent epithelial ovarian cancer who had complete or partial responses to platinum-based therapies.14
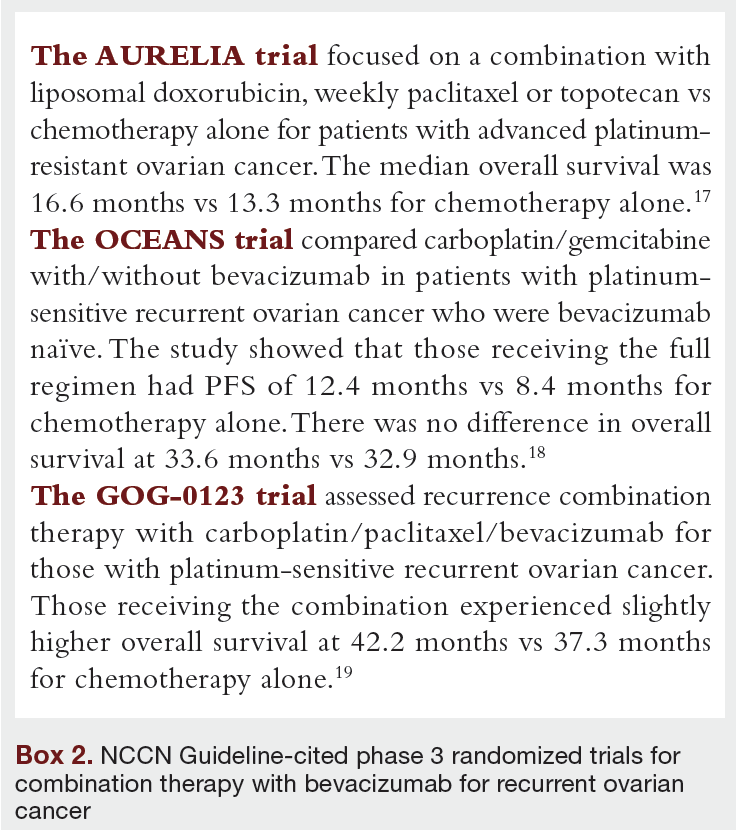
Bevacizumab was chosen as a preferred single agent option for those with recurrent disease (especially for those with ascites) for women with platinum-sensitive or resistent disease based on phase 2 trials.15,16 When used as a single agent, the response rate was about 20%. The Panel noted that bevacizumab may be used as a single agent maintenace therapy if patients responded to initial recurrence chemotherapy/bevacizumab regimens until disease progression or until the patient experiences unacceptable toxicity. The Panel cited several phase 3 randomized trials for combination therapy with bevacizumab for recurrent ovarian cancer (Box 2).
 Discussion
Discussion
While rates of ovarian cancer are decreasing slightly, as are rates of death, there are no good screening methods and most ovarian cancers are discovered at an advanced stage. Management usually includes sugery and systemic chemotherapy. Genetic testing is recommended, as it can influence treatment choices. Patients are often treated with multiple lines as recurrence occurs. Sometimes IP therapy is indicated as well. Studies continue to focus on new combinations as well as PARP therapies, usually for maintenance and recurrence.
References
1. US Cancer Statistics Working Group. US Cancer Statistics Data Visualizations Tool, based on November 2018 submission data (1999-2016): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute. June 2019. Accessed May 22, 2020. www.cdc.gov/cancer/dataviz
2. Ovarian Cancer Statistics. Centers for Disease Control and Prevention. Updated May 28, 2019. Accessed May 22, 2020. https://www.cdc.gov/cancer/ovarian/statistics/index.htm
3. Cancer Stat Facts: Ovarian Cancer. National Cancer Institute. Accessed May 22, 2020. https://seer.cancer.gov/statfacts/html/ovary.html
4. NCCN Clinical Practice Guidelines in Oncology: Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer, Version 1.2020 – March 11, 2020. Accessed May 22, 2020. https://www.nccn.org/professionals/physician_gls/default.aspx#ovarian
5. Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer Treatment (PDQ) Patient Version. National Cancer Institute. Accessed May 22, 2020. https://www.cancer.gov/types/ovarian/patient/ovarian-epithelial-treatment-pdq#_130
6. Types and Stages of Ovarian Cancer. National Ovarian Cancer Coalition. Accessed May 22, 2020. https://ovarian.org/about-ovarian-cancer/what-is-ovarian-cancer/types-a-stages
7. Pignata S, Scambia G, Lauria R, et al. A randomized multicenter phase III study comparing weekly versus every 3 weeks carboplatin (C) plus paclitaxel (P) in patients with advanced ovarian cancer (AOC): Multicenter Italian Trials in Ovarian Cancer (MITO-7)—European Network of Gynaecological Oncological Trial Groups (ENGOT-ov-10) and Gynecologic Cancer Intergroup (GCIG) trial. J Clin Oncol. 2017;31(suppl 18). doi:10.1200/jco.2013.31.18_suppl.lba5501
8. FDA approves niraparib for first-line maintenance of advanced ovarian cancer. Food and Drug Administration. April 29, 2020. Accessed May 22, 2020. https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-niraparib-first-line-maintenance-advanced-ovarian-cancer
9. FDA approves olaparib plus bevacizumab as maintenance treatment for ovarian, fallopian tube, or primary peritoneal cancers. The ASCO Post. May 8, 2020. Accessed May 22, 2020. https://www.ascopost.com/news/may-2020/fda-approves-olaparib-plus-bevacizumab-as-maintenance-treatment-for-ovarian-fallopian-tube-or-primary-peritoneal-cancers/
10. Gupta S, Nag S, Aggarwal S, Rauthan A, Warrier N. Maintenance therapy for recurrent epithelial ovarian cancer: current therapies and future perspectives–a review.
J Ovarian Res. 2019;12:103. doi:10.1186/s13048-019-0579-0
11. Domchek SM, Aghajanian C, Shapira-Frommer R, et al. Efficacy and safety of olaparib monotherapy in germline BRCA1/2 mutation carriers with advanced ovarian cancer and three or more lines of prior therapy. Gynecol Oncol. 2016;140(2):199-203. doi:10.1016/j.ygyno.2015.12.020
12. Kim G, Ison G, McKee AE, et al. FDA approval summary: olaparib monotherapy in patients with deleterious germline BRCA-mutated advanced ovarian cancer treated with three or more lines of chemotherapy. Clin Cancer Res. 2015;21(19):4257-4261. doi:10.1158/1078-0432.CCR-15-0887
13. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): a double-blind, randomized, placebo-controlled, phase 3 trial. Lancet Oncol. 2017;18(9):1274-1284. doi:10.1016/S1470-2045(17)30469-2
14. FDA approves olaparib tablets for maintenance treatment in ovarian cancer. Food and Drug Administration. August 17, 2017. Accessed May 22, 2020. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-olaparib-tablets-maintenance-treatment-ovarian-cancer
15. Cannistra SA, Matulonis UA, Penson RT, et al. Phase II study of bevacizumab in patients with platinum-resistant ovarian cancer or peritoneal serous cancer. J Clin Oncol. 2007;25(33):5180-5186. doi:10.1200/JCO.2007.12.0782
16. Burger RA, Sill MW, Monk BJ, Greer BE, Sorosky JI. Phase II trial of bevacizumab in persistent or recurrent epithelial ovarian cancer or primary peritoneal cancer: a gynecologic oncology group study. J Clin Oncol. 2007;25(33):5165-5171. doi:10.1200/JCO.2007.11.5345
17. Pujade-Lauraine E, Hilpert F, Weber B, et al. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: The AURELIA open-label randomized phase III trial. J Clin Oncol. 2014;32(13):1302-1308. doi:10.1200/JCO.2013.51.4489
18. Aghajanian C, Goff B, Nycum LR, Wang YV, Husain A, Blank SV. Final overall survival and safety analysis of OCEANS, a phase 3 trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent ovarian cancer. Gynecol Oncol. 2015;139(1):10-16. doi:10.1016/j.ygyno.2015.08.004
19. Coleman RL, Brady MF, Herzog TJ, et al. Bevacizumab and paclitaxel-carboplatin chemotherapy and secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (NRG Oncology/Gynecologic Oncology Group Study GOG-0213): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017;18(6):779-791. doi:10.1016/S1470-2045(17)30279-6









